Abstract
Objective: To evaluate the results of lateral
closing wedge humeral osteotomy and K-wire fixation following isolation and
protection of the ulnar nerve when used to correct cubitus varus deformity.
Methods: Forty-one cases of cubitus varus
deformity following supracondylar fractures of the humerus were operated by
lateral closing wedge osteotomy of the humerus during February 1999 to June
2007 at King Hussein Medical
Center. The mean age of
the patients at the time of corrective surgery was 7.2 years (range 4.7-12.3
years). The osteotomy was internally fixed with two crossed, smooth, K-wires.
After surgery, the patients were observed closely for more than one and half
year. We compared preoperative and postoperative humerus-elbow-wrist angle,
range of motion, and carrying angle for all patients. The results were
evaluated according to the criteria of Oppenheim et al.
Results: There were 36 excellent, four good and
one poor result. The average amount of correction of the humerus-elbow-wrist
angle was 24.3° and the carrying angle was 25.5°. Preoperatively, the range of
motion averaged 4.7° of extension to 125° of flexion, to a mean postoperative
range of motion of 4° of extension and 123° of flexion. The only one poor
result was due to early removal of the K-wires. However, in all patients, the
desired range of motion, good alignment, and complete union of the bone were
achieved.
Conclusion: We report that lateral closing wedge
supracodylar humeral osteotomy to correct post-traumatic cubitus varus through
posterior approach with isolation and direct vision control of the ulnar nerve
is relatively safe, simple and effective procedure with low rate of
complications, which is important in a procedure performed purely for cosmetic
indication.
Key
words: Cubitus Varus,
supracondylar fracture, supracondylar osteotomy.
JRMS
September 2010; 17(3): 33-38
Introduction
Cubitus
varus or “gunstock deformity” (Fig. 1) is the most common complication of
supracondylar humerus fracture with an incidence varying from 9 to 57%.(1-3)
Immediate and late causes of cubitus varus deformity are medial angulation,
medial rotation, overgrowth of lateral condyle and osteonecrosis or delayed
growth of medial condyle.(2) The medial angulation
is the major determinant for the deformity while medial rotation contributes to
it.(4) Cosmetic
appearance is the common indication for surgery, which more authors now agree,
should be performed as early as deformity becomes established.(4-6) Delayed ulnar nerve palsy and tardy posterolateral
rotary instability of the elbow can accompany cubitus varus and may require
treatment.(7) Various
corrective osteotomy procedures have been advocated in the treatment of cubitus
varus.

Fig. 1. Cubitus varus deformity
Fig. 2. Preoperative radiograph
showing the HEW angle of 20° varus and the
(19mm) planned width of supracondylar wedge to produce correction of the varus deformity
However, most of the osteotomies have been described, if not all are technically demanding and are being replaced for need of better stabilization, three dimensional correction and above all simplicity.(8-13) Medial open wedge osteotomy fell in to disrepute because of its inherent instability, need of bone graft and neurological complications.(5,14,15) Various newer techniques have been tried to correct the deformity in three dimensional planes but to achieve that, accurate preoperative planning, calculations and special attention to surgical details are needed,(1,12,13) and still results are no better than simple lateral closing wedge osteotomy.(4,5) Reconstructive procedures to correct cubitus varus deformity have many complications such as infection, loss of fixation, stiffness, nerve palsy and brachial aneurysm. Ulnar nerve palsy is reported in the literatures as high as 27% which is not accepted for a procedure performed for cosmetic reason.(4,15-18)
This
study was conducted to evaluate lateral closing wedge humeral osteotomy to
correct cubitus varus deformity, fixed with smooth, crossed K-wires after identification
of the ulnar nerve and protecting it.
Methods
Between
1999 and 2007, 41 lateral closing wedge supracondylar osteotomies fixed with
crossed smooth K-wires were performed to correct cubitus varus deformities
resulting from supracondylar fractures of the humerus at King Hussein
Medical Center.
The deformity which was secondary to fracture malunion was not progressive in
any patient. The primary indication for operation in all patients was
correction of cosmetic deformity. None of the patient or family members
recognized any functional deficit resulting from the cubitus varus deformity.
Among
the 41 patients, 26 were males and 15 were females. The right elbow was involved in 29 patients
and the left was involved in 12. The mean age at the time of injury was 3.9
years (range 15 months to 8 years), mean age at osteotomy was 7.2 years (range
4.7-12.3 years). The average follow-up was 5.9 years with a range of 1.5 years
to 8.8 years (Table I).
The
preoperative carrying angle was determined clinically by measuring the angle
formed by the intersection of the longitudinal axis of the upper arm and the
forearm, with the elbow in extension and supination. A radiographic
humerus-elbow-wrist (HEW) angle was also obtained with elbow in extension and
supination. Carrying angle and HEW angle were measured for both the injured and
normal extremity. Preoperative range of motion (ROM) of the involved elbow was
measured using a goniometer.
The wedge
shape osteotomy of the distal humerus is planned by measuring
the HEW of
the involved extremity then compared with that of the contralateral normal arm
and the difference between these radiographic angles is determined. This angle
is then plotted on the preoperative radiograph to define the size of the lateral wedge to be removed from
the supracondylar region of the distal humerus (Fig. 2). The base of the wedge is drawn
perpendicular to the olecranon fossa. The thickness of the wedge at the lateral
humeral cortex is measured and determines the amount of the bone to be resected
during the operation.
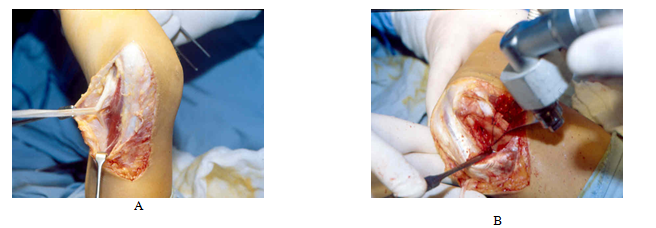
Fig. 3. A- Exposed ulnar nerve. B- Laterally based wedge removed after saw cuts were made

Fig. 4. Post-operative clinical correction for the
same patient in Fig 1
Operative
Procedure
The
procedure is performed under general anesthesia, full aseptic conditions,
pneumatic tourniquet and supine position. Posterior longitudinal incision is
made along the posterior aspect of the elbow for about 8 to 10 cm in length
starting from just below elbow joint upwards. The fascia is incised in line
with the skin incision, superficial dissection, the ulnar nerve is exposed,
isolated and protected under direct vision during the procedure (Fig. 3A). At
the lateral side of the elbow through the same incision, the interval between
the Brachioradialis muscle anteriorly and the Triceps muscle posteriorly is
developed. The distal humerus is then exposed by subperiosteal, without the
radial nerve exposure. Two osteotomy cuts necessary to form the laterally based
wedge are made with an osteotomy power saw perpendicular to the shaft of the
humerus across the width of the metaphyseal bone just superior to the olecranon
fossa. A second oblique cut is made proximally to form the preoperatively determined
thickness of the laterally based wedge (Fig. 3B) (an existing extension deformity
can also be corrected by removing additional bone anteriorly from the proximal
humeral segment).
An
attempt is made to preserve the medial cortex and periosteum to act as a
controlling “hinge” in closing the osteotomy site. A smooth 0.062 inch K-wire is
drilled through the distal fragment in retrograde fashion, so that it emerges
from the lateral epicondyle. The osteotomy site is closed, and the K-wire is
passed across to exit from the medial cortex of the proximal humeral segment.
This provides sufficient stabilization to allow a second 0.062 inch K-wire to
be driven percutaneously through the medial epicondyle (anterior to the ulnar nerve)
across the osteotomy site and to exit from the lateral
cortex of the proximal humeral segment. A third K-wire occasionally is passed
percutaneously from the lateral condyle across the osteotomy site for
additional stability.
The
elbow is extended, and final intraoperative correction is assessed by comparing
the clinical carrying angle of the involved extremity to the opposite normal
arm and by measurement of the HEW angle on an intraoperative radiograph. The
incision is closed in layers, and the K-wires are cut off beneath the surface
of the skin. The extremity is placed in a long-arm posterior splint with the
elbow at 90° of flexion. On postoperative day 2 or 3, this splint is changed to
a snugly fitting long-arm cast. The extremity is maintained in plaster until roentgengraphic
signs of healing are evident, usually in 4-6 weeks. The cast and K-wires are
then removed, and active exercises are initiated. The elbow is protected in a
sling or posterior splint until full motion is regained, HEW angle, and ROM are
determined at final postoperative follow-up.
Results
The
forty one patients had complete bone union by 12 weeks postoperatively, good
alignment and the desired range of motion of the elbow.
The
preoperative clinical carrying angle of the involved elbow was measured for all
patients and averaged 22.8° of varus (range 14.5°-34°). Postoperatively, the
involved elbow improved to a carrying angle of 3.3° of valgus (range 4° of
varus to 15° of valgus); this compared to a carrying angle of the opposite
normal elbow of 9.3° of valgus (range 7° to 15° of valgus). The average
correction of carrying angle was 25.5° (range 15°-36°).
The
average HEW of the normal extremity was 12° of valgus (range 4°-20°). The HEW
of the involved elbow averaged 20.7° of varus (range10°-33°).
|
Table I. Results of correction
of cubitus varus in the study group as per demographic characteristics
|
Parameter
|
Average
|
Range
|
|
Age at injury (year . month)
Age at operation (year . month)
Follow up (year . month)
Preoperative clinical carrying angle (varus)
Preoperative HEW angle (varus)
Postoperative clinical carrying angle (valgus)
Postoperative HEW angle (valgus)
Normal extremity HEW angle (valgus)
Correction clinical carrying angle
Correction HEW angle
ROM of injured extremity
Preoperative
Postoperative
|
3.9
7.2
5.9
22.8°
20.7°
3.3°
4.9°
12°
25.5°
24.3°
-4.7°-125°
-4°-123°
|
1.3 - 8
4.7 - 12.3
1.5 - 8.8
14.5° – 34°
10° – 33°
4° varus – 15° valgus
8° varus – 16° valgus
4° – 20°
15° – 36°
16° – 36°
-12° – 140°
-10° - 135°
|
|
|
Fig. 4. Post-operative clinical correction for the
same patient in Fig 1
|
Postoperatively,
this improved to a HEW angle of 4.9° (range 8° of varus -16° of valgus); the
average of correction was 24.3° (range 16°-36°).
Pre and postoperative range of motion were
measured for all patients. Preoperatively, the arc of motion averaged 4.7° of
extension (range 12°-35°) to 125° of flexion (range 110°-140°).
Postoperatively, average ROM was 4° of extension (range 0-10°) and 123° of
flexion (range 110°-135°). No extremity had a loss of arc of motion more than 5°
(Table 1).
Results
were categorized by the method of Oppenheim et al.(4)
An excellent required correction of the HEW angle to within 5° of the opposite
elbow, while maintaining ROM within 5° of preoperative arc of elbow motion. A
good result included a valgus position and motion within 10° of the
preoperative arc of elbow motion. A poor result included any case with a
perioperative complication, a residual varus position or loss of more than 10°
of motion, According to these strict criteria there were 36 excellent, four
good, and one poor result.
The
only one poor result exhibited residual radiographic varus postoperatively.
Review of radiographs showed removal of the K-Wires without enough callus
formation around the osteotomy.
No
complications were related to surgical approach, type of osteotomy, use of K-Wires fixation,
or postoperative protocol.
Discussion
Outward
angulation of the supinated forearm at the extended elbow, the carrying angle,
is present in utero and is completely developed in the newborn baby.(15)
A change in the carrying angle after treatment of a supracondylar fracture may
result from inadequate reduction, from loss of reduction with consequent
malunion, or from disturbance of growth at the lower end of the humerus. Most
authors consider that the medial angulation is the major determinant for the
deformity while medial rotation contributes to it.(4)
Cubitus
varus deformity represents a serious and common complication of supracondylar
fracture.(1-3) We recommend surgical correction anytime after
fracture union and full elbow motion has been obtained. Despite the cosmetic
appearance, there are other functional disturbances such as delayed ulnar nerve
palsy and tardy posterolateral rotary instability of the elbow.(7)
There
are several techniques of corrective osteotomy of the distal humerus. The medial opening
wedge osteotomy leads to instability and stretching of the ulnar nerve, and is
difficult to fix.(15) A dome osteotomy
can reorient the distal fragment in both the coronal and the horizontal
plane; thus, residual prominence of the medial and lateral condyle can be
avoided.(13) However,
because of contracture of the surrounding soft tissue, it is often difficult to
rotate the distal portion in the coronal plane and frequently some prominence
of the condyle remains. The simple cut translation osteotomy has a wide soft
tissue dissection regarding the tripces tendon and the joint capsule with high
incidence of ulnar nerve palsy.(18) A pentagonal osteotomy corrects angular
deformity, translating the distal fragment medially.(11) Protrusion of the lateral condyle can be
avoided with this approach, but the technique is complicated and difficult to
perform consistently. The external fixation method decreases the protrusion of
the lateral condyle, translating the distal fragment medially.(19)
However, there may be neurovascular injury, and the method causes discomfort to
the patient. Lateral closing wedge
osteotomy is the most common method reported in the literature.(4,16-18)
It is the easiest, safest and inherently the most stable osteotomy; however
serious complications have been reported including infection, loss of fixation,
skin loss, nerve palsy and brachial aneurysm.(4,15-19) Functional disability as a result of nerve
palsy following distal humeral osteotomy is not justifying a procedure
performed for cosmetic reason.
In
our study, we always isolated the ulnar nerve and released the cubital tunnel
before we performed the osteotomy in our patients. Identification of the ulnar nerve
is important to avoid nerve damage at the medial end of the wedge osteotomy and
percutaneous Kirschner wire fixation of the osteotomy site from the medial
condyle. None of our patients had ulnar nerve palsy or significant decrease in
arc of motion. In addition to avoiding potential adhesions and contractures
that could occur if the triceps is taken down posteriorly, the interval between
the Brachioradialis muscle anetriorly and the triceps muscle posteriorly
provides a safe exposure of the distal humerus without placing major
neurovascular structures at direct risk.
The
results of our study compare favorably with those previously reported in the literature.
The only poor result was from overestimation of the radiographic signs of the
healing process followed by removal of K-wires which resulted in partial recurrence
of the deformity. The patients and the parents were satisfied from the end result
of the surgery (Fig. 4).
Conclusion
We
report that lateral closing wedge supracodylar humeral osteotomy to correct
post-traumatic cubitus varus through posterior approach with isolation and
direct vision control of the ulnar nerve is relatively safe, simple and
effective procedure with low rate of complications, which is important in a
procedure performed purely for cosmetic indication.
References
1. McCoy GF, Piggot J. Supracondylar osteotomy
for cubitus varus: the value of the straight arm position. J Bone Joint Surg
[Br] 1988:70-B: 283-6.
2. Kasser JR, Voss FR. Uniplanar Supracondylar
osteotomy with pre set K-wire for cubits varus. J Paediatr Orthop 1994;
14:47.
3.Chess DG, Leahy JL. Cubitus Varus:
Significant Factors. Journal of
Pediatric Orthopedic 1994; 14; 190-192
4. Oppenheim WL, Clader TJ, Smith C, Bayer M. Supracondylar humeral
osteotomy for traumatic childhood cubitus varus deformity. Clin Orthop
1984; 188:34-39.
5. Bellemore MC. Barrett IR, Middleton RWD,
Scougall JS, Whiteway EW. Supracondylar osteotomy of the humerus for
correction of cubitus varus. J Bone Joint Surg (B) 1984; 66:566-572
6.Danielsson LG, Hussein S, EI-Haddad I, Gupta RP. Staple fixation of
osteotomy for cubitus varus. A simple technique used in 11 children. Acta
Orthop Scand 1991; 62:55-57.
7. O’Drisol SW, Spinner RJ, Morrey BF. Tardy Posterolateral rotary instability of the
elbow due to cubitus varus due to cubitus varus. J Bone Joint Surg Am
2001; 83: 1358-1369.
8. Takahashi M, Arika N. Arc osteotomy of the
humerus to correct cubitus varus. Clinical Orthopedics and related Research
1997; 336: 111-115.
9. Song
HR, Cho SH, Jeong ST,
Park YJ, Koo KH. Supracondylar
osteotomy with Ilizarov fixation for elbow deformities in adults. J Bone
Joint Surg Br 1997; 79:748 -52.
10.
Tahdjian MR. Osteotomy of distal
humerus for correction of cubitus varus. In Smith AB (ed).
Pediatric Orthopedics. Philadelphia,
WB Saunders 1972; 1588-1591.
11.
Laupattarakasem W, Mahaisavariya B, Kowsuwon W,
Saengnipanthkul S. Pentalateral osteotomy for cubitus varus. Clinical
experiences of a new technique. J Bone Joint Surg Br 1989; 71:667 -70.
12.
Murase T, Oka K, Moritomo H, Goto A. Three-dimensional
corrective osteotomy of malunited fractures of upper extremity with use of a
computer simulation system. J Bone Joint Surg Am 2008; 90:2375-2389.
13.
Kanaujia RR, IkutaY, Muneshige H, Higaki T,
Shimogaki K.
Dome osteotomy for cubitus varus in children. Acta Orthop Scand 1988;
59:314-7.
14.
Attenborough CG. Remodelling of the
humerus after supracondylar fractures in childhood. J Bone Joint Surg [B] 1953;
35: 286-295.
15.
King D, Secor C. Bow elbow. J Bone
Joint Surg Am 1951; 33:572-6.
16.
Miguel A, James W. Corrective Osteotomy
for cubitus varus deformity. J Paediatr Orthop 1994;
487:491.
17.
Ippolito E, Moneta MR, d’Arrigo C. Post-traumatic cubitus
varus .Long term follow-up of corrective humeral osteotomy in children. Bone
Joint Surg Am 1990; 72: 757-765.
18.
Kim HT, Lee JS, Yoo CI. Management varus and valgus. Bone Joint
Surg Am 2005; 87: 771-780.
19.
Karatosum V, Alekberov C, Alicic E, Ardic CO,
Aksu G.
Treatment of cubitus varus using the Ilizarov technique of distraction
osteogenesis. J Bone Joint Surg Br 2000; 82-B: 1030
Related References
1. Hahn SB, Choi YR, Kang HJ. Corrective dome osteotomy for cubitus varus and valgus in adults. J Shoulder Elbow Surg 2009 Jan-Feb; 18(1):38-43.
2. Cho CH, Song KS, Min BW, Bae KC, Lee KJ. Long-term results of remodeling of lateral condylar prominence after lateral closed-wedge osteotomy for cubitus varus. J Shoulder Elbow Surg 2009 May-Jun; 18(3):478-83.
3. Ozkan C, Dogramaci Y, Kalaci A, Gülşen M, Bayram H. Results of using Ilizarov distraction osteogenesis technique for the treatment of cubitus varus deformities in adults. Arch Orthop Trauma Surg 2009 May 14.
4. Gong HS, Chung MS, Oh JH, Cho HE, Baek GH. Oblique closing wedge osteotomy and lateral plating for cubitus varus in adults. Clin Orthop Relat Res 2008 Apr; 466(4):899-906.