ABSTRACT
Objective: To describe
hernia repair under local anesthesia with regard to the technique, morbidity
and hospital admissions after the procedure.
Methods: Two-hundred
hernia repairs were performed under local anesthesia for 178 patients at King Hussein
Medical Center
and at Prince Hashem Hospital
between January 2005 and January 2007. All patients were assessed
preoperatively by a senior surgeon and written consent was obtained. The anesthesia protocol used included 0.5%
lignocaine and 0.25% bupivacaine as local anesthesia supplemented with
intravenous sedation by the anesthesiologist as necessary. Patients were monitored intraoperatively for
heart rate, blood pressure and pulse oximetry.
Results: The procedure was successfully performed for 197 hernias
under local anesthesia. Only three
patients required general anesthesia. The
first 50 patients were admitted overnight for observation, the rest were all planned
as day case surgeries and were followed up over a three month period. Four
patients developed wound hematoma, two patients developed wound infection, one
patient developed post operative urine retention, and two patients showed
evidence of recurrence when reviewed after one year.
Conclusion: Our study confirmed the safety and
convenience of using local anesthesia for hernia repair. Less post operative discomfort and low morbidity
rate was obtained. Hernia repair under local anesthesia can be learnt easily
and quickly, therefore it is the recommended procedure to be used in our
practice for the repair of inguinal hernia.
Key words: Inguinal hernias, Local anesthesia, Repair
JRMS
September 2010; 17(3): 57-60
Introduction
Hernia repair continues to
be one of the commonest operations in general surgery with 10% of the male
population having a hernia in their life time. Inguinal hernias are the most
common type of hernia and once a hernia occurs it usually enlarges with time,
at the very best it stays the same but will never cure itself. A growing
interest in the use of local anesthesia for inguinal hernia repair with
increasing popularity of day case surgery, it certainly seems to be an
acceptable alternative for the elderly and to patients with co-morbidities.(1)
This study was conducted to
describe hernia repair under local anesthesia with regard to technique,
morbidity, and hospital admissions after the procedure.
Methods
This is a retrospective
analysis of 178 male patients who underwent hernia repair under local
anesthesia, performed at King Hussein medical Center and at Prince Hashem
Hospital between January 2005
and January 2007. A total of 200 inguinal
hernia repairs
were done for 178
male patients, 22 of which had bilateral
hernias, 104 had right a sided hernia and 52 had a left sided hernia.
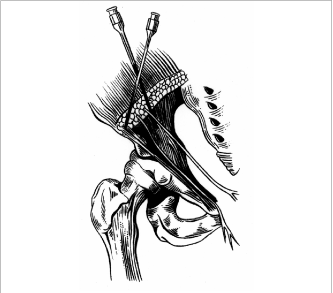
Fig. 1. Local
anesthetic given to the ileoinguinal nerve region
Fig. 2
Local infiltration along the incision
Table I.
Number of hernias according to site and type
|
No. of hernias according to site
|
No. of hernias according to type
|
|
Right sided
|
104
|
Direct
|
51
|
|
Left sided
|
52
|
Indirect
|
145
|
|
Bilateral
|
22
|
Pantaloon
|
4
|
|
Total
|
200
|
Total
|
200
|
One hundred forty-five patients had an indirect hernia, 51 patients had a direct hernia, four patients had a pantaloon hernia, and 12 patients had an
operation for recurrent hernia (Table I).
In order to assess for the possibility of day case surgery, they were
diagnosed and assessed initially by a senior surgeon in the outpatient department,
and were listed for surgery. On the week prior to their surgery, they were
reassessed, clinically examined, and a written consent was obtained from all
patients. Preoperative investigations
were only performed whenever indicated.
Patients with bilateral inguinal hernia were operated initially only on the
more symptomatic side while the other side was repaired within 4-6 months from
the first surgery.
All patients were operated
upon under local anesthesia supplemented with intravenous sedation by the
anesthesiologist whenever necessary. The sedation used included Dormicum
0.05-0.1 mg/kg and Ketamin 1-1.5 mg/kg with short acting opioids.(2,3)
A second generation Cephalosporin was given before starting the operation.(4,5)
The local anesthesia mixture used was 0.5% lignocaine (2-3 mg/kg if plain or
5mg/kg with adrenaline if it was felt that the patient would need extra
amount), 5 mls of 0.25% bupivacaine to prolong the action of the anesthesia,
and 2-3 ml of sodium bicarbonate 7.5% to
reduce the burning sensation and to reduce onset time.( 6)
Before the scrubbing and putting gowns to give
extra time for the block to develop the local anesthesia was introduced by 22
gauge needle as a field block, 10 ml were given one inch medial to the anterior
superior iliac spine in the neurovascular plane in a fan - like manner, 15 ml were
infiltrated in the subdermic and deep subcutaneous area along the line of
incision, 15 ml were infiltrated at the deep inguinal ring and the needle was advanced
along the inguinal canal, 5-10 ml were infiltrated over the pubic tubercle in a
fan-like manner as shown in figures 1 and 2.(7)
Patients were monitored
intraoperatively for heart rate, blood pressure and pulse oximetry and an anesthetist
was present to intervene if required. Once
we became confident with the procedure, monitoring was limited to pulse
oximetry with verbal contact between the surgeon and the patient and the
anesthetist was available upon request but not in the theatre.
The procedure was completed
successfully in all but three patients where it was converted to general
anesthesia. In two cases it was due to high
anxiety and in one case the level of anesthesia was felt to be unsatisfactory
to carry on with the procedure.
In the indirect inguinal
hernias the sac was transfixed at the internal ring, while with direct hernias
the sac was dissected and reduced. Shouldice repair was performed for all
patients using non absorbable prolene stitches. The first 50 patients they were
admitted overnight for observation, but the rest were all planed day case
surgeries. Patients were discharged from the day case unit at the end of the
working day by the operating surgeon.
They were given a prescription of diclofenac sodium or paracetamol and a
physician’s contact number to report anything abnormal or for any queries that
may arise.
Patients were seen at three
weeks, three months, and one year after surgery unless otherwise indicated. Simple
descriptive statistics were used to analyze the findings.
Results
Fifty-three patients (29.8%)
were discharged the day after surgery and 125 (70.2%) patients were discharged on
the same day and their mean hospital stay was 4.2 hours (range 3 -5 hours). The total mean hospital stay for all the
patients after surgery was 9.6 hours (range 3-24 hours). In three patients (1.7%) the procedure was converted
to general anesthesia. The first 50
patients (28.1%) were admitted overnight for observation and the rest had their
procedure as a day case.
Follow-up over a three month
period revealed no perioperative deaths, however four patients (2.2%) developed
wound hematoma, two patients (1.1%) developed wound infection, one patient
(0.56%) developed post operative urine retention which proved to be due to
benign prostatic enlargement that required transurethral prostatectomy at a
later stage. In no instance was
postoperative neuralgia or chronic pain reported. Two patients (1.1%) showed
evidence of recurrence when reviewed after one year.
Discussion
Elective surgical repair of
an inguinal hernia is a common surgical procedure. The treatment, however,
presents several challenges regarding type of anesthesia used for the
procedure, post operative analgesia, as well as, planning of the procedure.
Local, general, and regional anesthesia are all used for the repair, but to
different degrees, primarily depending on traditions, experience and whether
the institution has specific interest in hernia surgery.(9)
Thus, the use of local anesthesia varies from a few percent in Sweden, to 6% in
France, 60% in Denmark, 83% in USA and up to almost 100% in specialized
institutions dedicated to hernia surgery.
The feasibility of local
anesthesia is high, as judged by the low rate of conversion to general
anesthesia (1%).(8) The generally low rate of serious
complications do not allow firm conclusions, but the rate of less serious
complications is lower in local anesthesia, compared to the other anesthetic
techniques. Of special interest is that the rate of urinary retention can be
eliminated by the use of local anesthesia. In comparative studies, local
anesthesia gained a higher degree of patient's acceptance and satisfaction than
other anesthetic techniques.(10)
Local anesthesia also allows faster mobilization and earlier
discharge from post anesthetic care units than other anesthetic techniques.
Pain after hernia repair is
more pronounced at mobilization or coughing than during rest and younger
patients seem to have more pain than older patients. The pain ceases over time,
and it is most pronounced the day after surgery, where two thirds have moderate
or sever pain during activity, while one third still have moderate or sever
pain after one week, and approximately 10% after four weeks. Postoperative pain
is best treated with a combination of local analgesia and peripherally acting
agents (paracetamole, NSAID or their combination),(11) while opioids should be avoided due to side
affects, primarily nausea and sedation.
Moderate or severe pain one
year postoperatively is seen in 5-12% of patients. The following factors have
been related to a higher rate of chronic pain: previous or subsequent hernia
surgery on the same side, young age, and pain before surgery, high pain scores
in the immediate postoperative period, postoperative complications and
prolonged convalescence. Patients should be informed about the risk of chronic
pain, particularly if the hernia is asymptomatic.(12)
Patients should be informed
that they can immediately resume all activity if the pain permits, but also to
expect that pain may limit activities of daily living during the first
postoperative week.(13,14) Hernia surgery, including
treatment of recurrent hernias, can and ought to be performed as day case
surgery, irrespective of the chosen anesthetic technique, as there are no
medical or surgical contraindications to this. Social causes may indicate that
overnight stay may be advised or desirable, preferably in a patient hotel
facility. A day case hernia surgery service should be organized with
standardized patient records, including descriptions of surgery performed, type
of anesthesia used and post discharge medication given.
As large numbers of patients
undergo hernia surgery each year, the surgical technique should be a simple
one. The results obtained by general surgeons using various open, tension-free
techniques, irrespective of the anesthetic used, are excellent and appear to
approach those of specialists. Surgical residents should be taught repairs
under local anesthesia, since with an aging population we may soon be faced
with an increasing number of patients who are not fit for general anesthesia.(15)
Finally, when consulting a patient with an inguinal hernia, primary or
recurrent, the surgeon should pose the question "which combination of
anesthesia and hernia repair is the safest and best for my patient?" Local
anesthesia with appropriate analgesia and sedation is the safest of all
techniques and is suitable for most if not all open repairs. Attention to
surgical technique is paramount, and given the number of hernias repaired
annually, it is pertinent to recall the words of Wakely, who said "A
surgeon can do more for the community by operating on hernia cases and seeing
that his recurrence rate is lower, than he can by operating on cases of malignant
disease". (16)
Conclusion
Our study has confirmed the safety, and
convenience of using local anesthesia for inguinal hernia repairs. Both post operative discomfort and morbidity
rates are low. The procedure can be
learnt easily and quickly therefore it is the recommended procedure to be used
in our practice for the repair of inguinal hernia.
References
1.
Parviz A, Alex G, Irving L.
Local anesthesia for inguinal hernia repair step by step procedure. Ann of
surgery 1994; 220: 737-745.
2.
Kehlet H, White PF. Optimizing
anesthesia for inguinal herniorrhaphy: general, regional or local? Anesth
Analg 2001; 93:1367-9.
3.
Callesen T, Bech K, Kehlet H.
One thousand consecutive inguinal hernia repairs under unmonitored local
anesthesia. Anesth Analg 2001; 93: 1373-6.
4.
Sanabria A, Domingues L,
Valdivieso E, et al. Prophylactic
antibiotics for mesh inguinal hernioplasty. Ann of surgery 2007; 245: 392-396.
5.
Aufenacker T, Dirk V, Taco VM, et
al. The role of antibiotic
prophylaxis in prevention of wound infection after
lichtenstien open mesh repair of primary inguinal hernia. Ann of surgery
2004; 240: 955-961.
6. Anderson FH, Nielson K, Kehlet H. Combined ilioinguinal blockage and local infiltration anesthesia for
groin hernia repair-a double- blind randomized study. British Journal of Anesthesia
2005; 94(4): 520-3.
7.
Jose M, Hemerson P, Paulo P, et al. Inguinal hernia repair in children: importance of
local anesthesia association. Arq
Gastroenterol 2002; 39: 204-208.
8.
Hung L, Francis L, Jensen P,
Clinical factors influencing return to work after ambulatory inguinal
herniorrhaphy in Hong Kong. Ambulatory Surgery
2001; 9: 73-75.
9.
Patrick O, Michael S, Keith M, Caron, et al Local or general anesthesia for open hernia
repair: a randomized study. Ann of surgery 2003; 237:574-579.
10. Putnis S, Merville-Tugg R,
Atkinson S. One-step inguinal hernia
surgery-day-case referral, diagnosis and treatment. Ann R Coll Surg Engl 2004; 86:
425-427.
11. Romsing J, Moiniche S, Dahi J.
Rectal and parentral paracetamol, and
paracetamol combination with NSAIDs, for postoperative analgesia. British Journal
of Anesthesia 2002; 88 (2): 215-226.
12. Dennis R, O'Rionrdan D.Risk factors for chronic pain after inguinal
hernia repair. Ann R Coll Surg Engl 2007; 89: 218-220.
13. Poobalan AS, Bruce J, King Pm,
Chambers WA, et al. Chronic
pain and quality of life following open inguinal hernia repair, British Journal
of Anesthesia 2001; 88(8): 1122-6.
14. Biemans
J, Schmitz R, Pierik E, et al. Patient
satisfaction after laparoscopic and conventional day case inguinal hernia
repair. Ambulatory Surgery 1998; 6: 169-173.
15. Davies BW, Campbell WB, Inguinal hernia repair: see one, do one, teach one.
Ann R Coll Surg Engl 1995; 77: 299-301.
16. Stephenson BM, Complication of open groin hernia repairs.
Surgical Clinic in North America 2003; 83(5):1255-78.