IntroductionEfforts have been made to define dry socket more accurately through the use of terms such as alveolar osteitis, localized osteitis, post extraction osteomyelitis syndrome, alveolalgia, avascular socket, and fibrinolytic alveolitis (1,2).
However, the term dry socket is still the most common term to be used for this condition. The clinical features of dry socket present as necrosis or disintegration of the originally occurred blood clot, halitosis, pain from the extraction socket which usually occurs 2 - 3 days after tooth extraction and may last for several days to weeks, hyperemic surrounding gingival tissue, as well as pain radiating to different adjacent parts or organs such as ear, temporal region, angle of mandible, eye and forehead.
Dry socket continues to be common in oral surgical practice. Despite numerous investigations carried out through the last century, its etiology is still not fully understood. Most authors believe it to have a multifactorial etiology which can be divided into general factors such as age, sex, decreased body resistance due to systemic disease, nutritional deficiency, and local factors such as anatomical location, traumatic surgery, smoking, fibrinolysis of the clot, local circulation, local anesthesia and vasoconstrictors (1-3).
The incidence of dry socket has varied greatly from one study to another, being reported as low as 0.5% and as high as 68.4% with an average ranging from 1%-3% (1). The aim of the present study was to investigate the incidence of dry socket, and to evaluate the effect of age, sex, site of extraction, multiple and single extraction, kind of extraction, general health, oral hygiene and smoking on the incidence of dry socket.
MethodsData were collected from records kept in the department of oral and maxillofacial surgery. The study population included patients who returned in pain following dental extraction, either by simple extraction or by a minor surgical procedure. All patients had local anesthesia; no general anesthesia cases were included.
In 1994, a total of 270 patients attended in pain following their dental surgery. These patients' files were fully reviewed and it was found that 115 of these were diagnosed as having dry socket. Six files could not be found and 149 patients were back in pain with different conditions e.g. post apicectomy, dental abscesses, pericoronitis, etc.
Of these 115 patients diagnosed as having dry socket, seven patients had had teeth extracted elsewhere and were therefore excluded from the study. The final total number of dry socket cases was therefore 108.
Junior hospital staff made the diagnosis of the majority of dry sockets; the remainders were diagnosed by more senior staff in charge.
After reviewing the files of the 108 patients, the following data were collected:
• Age and sex of the patient.
• Medical history, which included any concurrent systemic disease, medication and allergy.
• Social habits, especially smoking.
• Oral hygiene.
• Diagnosis made prior to extraction e.g. pulpits, dental abscess, pericoronitis, periodontal disease, etc.
• Date of return in pain and diagnosis of dry socket.
• Treatment administered.
• Duration of treatment i.e. from day of return to final visit or until the patient failed to attend for review.
In this study, and in order to carry out statistical tests for the incidence of dry socket in relation to different parameters e.g. age, sex, etc, a random sample of 100 patients who underwent dental extraction (patients other than dry socket cases) was taken. From this representative sample, the proportions of patients from the whole population in relation to different parameters (such as age, sex, chief complaint, medical history, diagnosis before extraction, etc) have been estimated.
The Chi square test was used for statistical analysis where appropriate.
Results Incidence of Dry Socket From the present survey, the total number of the patients who underwent dental extraction in 1994 was 4092, of whom 3176 underwent routine extraction and 916 teeth were extracted by a trans-alveolar approach. All the teeth were extracted with local anesthesia.
The number of teeth extracted was 5516, of which 4460 were removed routinely and 1056 were removed surgically.
108 patients returned with 115 dry sockets giving a dry socket incidence of 2.6 % of cases and 2.1 % of teeth extracted.
The Effect of Sex and AgeThe Patients who returned with dry socket comprised 48 females (44.4 %) and 60 males (55.6 %). From the sample that was taken, it has been found that the percentage was 63% and 37% for males and females, respectively.
Extrapolating this to the whole population, this gave an estimate of 2578 males and 1514 females who underwent dental extraction in 1994, with an incidence of dry socket for males and females equal to 2.3% and 3.2%, respectively. The difference was found to be statistically not significant; for this difference X2 = 2.61 (d.f. = 1; p >0.05).
The patients in this series have been divided into six age groups as shown in Fig. 1.
It has been observed that up to the age of 18 years no cases of dry socket were noted. The highest frequency was seen in the 19 - 30 years age group, the next in the order of frequency was in the group 31 - 40 years. The youngest age recorded having a dry socket was 19 years old, while the oldest was 83 years old.
The Site of ExtractionThe teeth were grouped into anatomical sites for the purpose of analyzing dry socket incidence. The numbers of teeth extracted in each site, together with the numbers of dry socket resulting are shown in Table I (A + B).
The highest incidence of dry socket formation was found to be in the lower jaw (2.7 %), which was twice more than the upper jaw (1.4 %), the difference was found to be statistically significant; X2 = 11.54 (d.f. = 1; p <0.05).
The highest incidence of dry socket formation was in the lower first molar region (4.8%) and the lowest was in the lower incisors region. Chi square analysis of these data showed that the incidence of dry socket was significantly influenced by site in the lower jaw, for this difference X2 = 19.93 (d.f. = 6; p < 0.05), but not in the upper jaw, for this difference X2 = 6.84 (d. f. = 6; p > 0.05).
Effect of Single and Multiple ExtractionsIt has been found that the incidence of dry socket in cases of single extraction was much higher than in multiple extractions. Using Chi square analysis of these data showed that the difference between single and multiple extractions was statistically significant, for this difference X2 = 21.13 (d. f.=1; p <0.05). The number of teeth extracted, together with the number of dry sockets and patients with their percentages are shown in table II.
The Effect of Routine and Surgical ExtractionThe incidence of dry socket was found to be higher in cases of routine dental extraction than in surgical ones.
Chi square analysis revealed that the difference between routine and surgical extraction was statistically significant, for this difference X2 = 6.95 (d.f. = 1; p <0.05).
Numbers of extracted teeth and dry sockets with percentage of occurrence are detailed in table III.
The Effect of General Health of The PatientThe patients have been classified into two groups according to the American Society of Anesthetists (ASA):
Healthy subjects or ASA 1: Those individuals have no systemic disease.
ASA 2 or 3 subjects: Those individuals who gave a history of systemic illness and / or those patients under regular medications (except females on the contraceptive pills).
From the sample of 100 patients taken, 76% of the samples were ASA 1. This gives an estimate of 3110 patients from the whole population with 81 dry sockets giving an incidence of 2.6%. Twenty four percent of the sample was ASA 2 or 3, which gives an estimate of 982 patients from the population with 27 dry sockets, giving an incidence of 2.7%. These findings were found to be statistically not significant when Chi square analysis was used, for this difference X2 = 0.05 (d.f. = 1; p >0.05).
The numbers of the cases of dry socket and their incidence in relation to health condition of the patients are represented in Table IV.
Effect of Smoking and Oral Hygiene ConditionsRegarding smoking, patients have been classified into three groups: smokers , non-smokers or unknown.
The results of sampling 100 patients showed that 30% of the sample were smokers which, when extrapolated represents 1227 patients in the whole group. The number of dry sockets in this group was 53, an incidence of 4.3%. Fifty six percent of the sample were nonsmokers, extrapolated to 2292 patients in the whole population. This group had 48 dry sockets, an incidence of 2.1%. Fourteen percent of the sample were unknown, representing 573 patients with 7 cases of dry sockets, an incidence of 1.2%. This group was excluded from statistical tests (Table V).
Chi square analysis of smokers versus non-smokers showed the difference to be statistically significant; X2 = 14.59 (d.f. = 1; P <0.05).
The oral hygiene condition of the patients was divided into 4 categories: good, fair, poor and unknown (Table V).
From the 100 patient samples taken, 16% of the sample had good oral hygiene, extrapolated to 655 patients from the whole population. The number of dry socket cases related to this group was 5, an incidence of 0.8%; 36% of the sample was fair, representing a total of 1473 patients with 51 dry socket cases, an incidence of 3.5%, 28% of the sample had poor oral hygiene, representing 1146 with 44 cases of dry socket, an incidence of 3.8%. The last group (unknown) representing 20% of the sample, which is equal to 818 patients with 8 cases of dry socket with an incidence of 1%.
By using Chi square test to analyze these data and by excluding the last group (unknown) from this analysis, the difference was seen to be statistically significant, for this difference X2 = 14.81 (d.f. = 2; p <0.05). The exclusion of the unknown group may result in some bias in the final result of the statistical test as this group contains 818 patients with 8 dry socket cases with an unknown number of good, fair and bad oral hygiene.
Pre-Extraction Condition of the TeethThe data related to reasons for extraction of the teeth have been obtained from the case history of the patients after reviewing their files. The pre-extraction conditions of the teeth (as diagnosed by the dental staff) have been categorized into either pathological conditions or non-pathological conditions (Table VI).
From the sample of 100 patients taken, the following percentages were found: Thirty eight percent pulpitis, 41% periapical pathology, 3% periodontal disease, 8% pericoronitis, 7% restorable teeth but patients were not willing to continue treatment, 3% prosthetic and orthodontic reasons. The overall incidence of dry socket for the pathological group was 1.8% and for the non-pathological group was 5%. By applying the Chi square test in analyzing this data, it was shown that the difference between pathological and non-pathological groups was statistically significant; X2 = 24.34 (d.f. = 1; p <0.05). The difference between various pathological conditions was found to be statistically not significant; X2 = 1.9 (d.f. = 3; p >0.05).
Time Lapse from Extraction Until Diagnosis of the Condition
The time taken from extraction until the patient returned in pain and dry socket diagnosis was calculated.
The analysis of data revealed that the peak of cases of dry socket was found to be after 2 days of extraction. One case returned back in pain and was diagnosed as dry socket after 24 hours from extraction, 25 cases were back in pain in the second 24 hours, 17 cases were diagnosed on the third day after extraction, 18 cases on the fourth day, 23 cases on the fifth day and 15 cases on the sixth day.
The number of cases of dry socket in relation to the time lapse from extraction is represented graphically in Fig. 2.
Of the total 108 patients, 77 (71.2%) received one treatment visit, while 28 (26%) received two treatment visits and only 3 (2.8%) had three treatment visits.
Type and Duration of TreatmentAs there was a wide range of treatment methods that have been used in the treatment of dry socket by the staff of the dental hospital, these methods as well as the number of cases of dry socket in relation to type of treatment are illustrated in Table VII.
Duration of treatment of dry socket was calculated from the day of reporting to the final visit or until the patient failed to attend for review of healing.
Analysis of the present data revealed that for the majority of the patients, it took an average of one week for improvement and healing. Many patients failed to attend their first appointment, the number being 77. Cases of dry socket in relation to duration of treatment are demonstrated graphically in Fig. 3.
It has been noticed that the type of treatment did not affect the duration of treatment and this will be discussed later.
Discussion The incidence of dry socket in this study was 2.6% of all extracted teeth and 2.1% for all cases, and this is in accordance with most previous studies (3-6).
Early studies reported that there was no difference in the sex distribution in relation to dry socket (4,5). Later studies showed that there was a tendency of dry socket to occur in females more than males (3,6-9). This may be due to the fact that before 1960 oral contraceptives were not appreciably used. As they became increasingly popular and widely available, more women began using them, and the incidence of dry socket has noticeably increased (10,11).
In this study, the results showed that although the incidence of dry socket in females (3.2%) was higher than in males (2.3%), this difference was statistically not significant. The findings in this study in relation to age revealed that the highest incidence was in the 19 - 30 years age group. The number decreased dramatically after this age group, supporting most other studies (3,5,6,9).
The incidence of dry socket in this study was significantly higher in the lower jaw (2.7%) than in the upper jaw (1.4%). It has been found that the molar area and in particular the first molar region in both jaws has the highest incidence of dry socket followed by the third molar region in the lower jaw and second premolar in the upper jaw. This is in accordance with many studies (3,4,8,9). An interesting finding was that the incidence of dry socket in lower canine region occupied the third place after first and third molar region, and this is in contrast to other studies where most authors agreed that it is rare for dry socket to take place in the anterior region (8,9). A number of studies have indicated that the incidence of dry socket is lower after multiple than after a single extraction (3,4,8), and this is confirmed by the present survey in which dry socket incidence was 1% for multiple extractions and 2.7% for a single extraction; the difference was found to be statistically significant (P <0.05).
Opposite findings were reported by some authors where they reported a higher dry socket incidence following multiple extractions than a single extraction. This was justified by those authors by the fact that patients in recent years have become less tolerant of pain and discomfort (9,12).
As far as the type of extraction is concerned, the results in this survey revealed that the incidence of dry socket was higher after routine than surgical (trans-alveolar) extraction and the difference was statistically significant (p <0.05).
These findings were in contrary to most previous studies, where most of the authors agreed that traumatic extraction is an important etiological factor in dry socket (3,4,13-15).
The role of general health in dry socket incidence is still controversial. Some authors believe that certain diseases (e.g. uncontrolled diabetes, anemia, liver disease) result in impairment of the immune system of the body and increase the incidence of dry socket following dental extraction (13). On the other hand, other authors did not find any correlation between the incidence of dry socket and medically compromised patients (3,16). The results in this study support the latter results, where the incidence of dry socket was nearly the same and the difference was statistically not significant (p >0.05), i.e. there was no correlation in this study between incidence of dry socket and general health of the patient.
It has been argued whether smoking has a role in the incidence of dry socket. Sweet and Butler (17) have reported that smokers are four times likely to develop dry socket than non-smokers. Meechan et al (18) have reported a higher incidence of dry socket in heavy smokers than light and non-smokers. In contrast, other authors have denied such an effect (19,20). The result of this study showed that the incidence of dry socket in smokers was twice that in non-smokers and the difference was statistically significant providing that the unknown group was excluded from the statistical test.
The result obtained from this survey suggested that the incidence of dry socket increased with poor oral hygiene.
Several authors have emphasized that periapical or marginal infection in the alveolus and the blood clot may predispose to the development of dry socket. Meyer (21) has reported a high incidence of dry socket following pericoronitis 14%. In this study, it has been observed that the incidence of dry socket following extraction of healthy teeth is much higher than in diseased teeth, with this difference being statistically significant (p < 0.05). This suggests that the role of pre-existing infection is not significant. In the pathological group, the highest incidence of dry socket was found to be in the periodontal disease group, followed by periapical pathology, then pulpitis, and finally pericoronitis. The difference in the incidence of dry socket between these groups was found to be not significant.
In this study, a wide variety of techniques and
materials have been used in the treatment of dry socket, the results have suggested that whatever the type of treatment used, it did not affect the course of the disease. It could therefore be suggested that dry socket is a self-limiting condition taking 10 - 14 days to resolve.
One case reported 46 days until resolution, but this was due to presence of a bone fragment in the socket and when the fragment was removed surgically and the condition resolved.
Conclusion The incidence of dry socket in this study was 2.6% of extraction cases and 2.1% of extracted teeth. Dry socket incidence was found to be affected significantly by the age of the patient, the site of extraction, type of extraction, single or multiple extraction, smoking and oral hygiene level. Also it was concluded that dry socket is a self-limiting condition and the different types of treatment did not affect the course of the disease which usually takes 10 - 14 days to resolve.
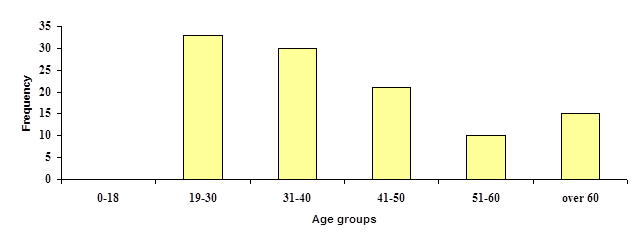
Fig. 1. Incidence of dry socket in relation to age.
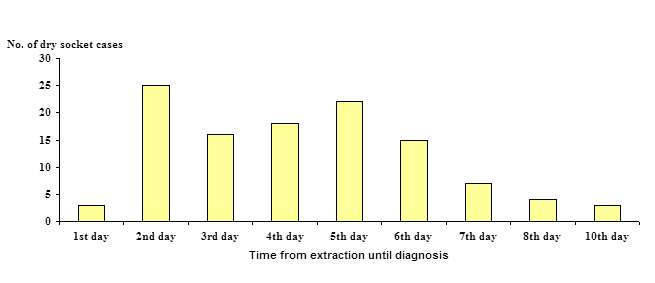
Fig. 2. Number of cases of dry socket in relation to time lapse from extraction until diagnosis.
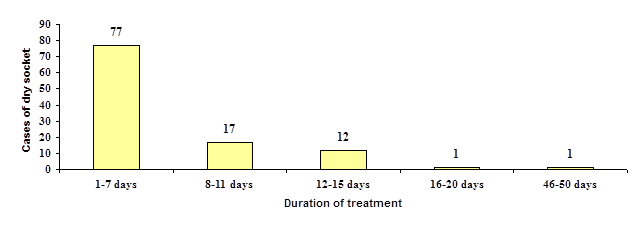
Fig. 3. Cases of dry socket in relation to duration of treatment
Table I-A: Localization of extraction and dry socket in the upper jaw
** = American Society of Anesthetists.
Table V. Incidence of dry socket in relation to smoking and oral hygiene condition