Objective: To evaluate the outcome of modified Mitchell’s osteotomy for treatment of hallux valgus.
Methods:
We reviewed the results of 69 patients (84 feet) in whom the modified
Mitchell’s osteotomy with Y shape advancement of medial capsule, lateral
adductor tenotomy and lateral capsule release, was done between
1993-2001 with an average follow up of 30 months (range 10-48 months).
Results:
Radiographic and subjective results were evaluated. Preoperative
criteria included intermetatarsal angle of greater than 14 degrees
(average 16.16), average metatarsophalangeal angle was 38.4 degrees
(range 32-48 degrees) and painful Hallux valgus deformity. The average
postoperative intermetatarsal angle was 7.9 with relative correction of 8
degrees. The average postoperative metatarsophalangeal angle was 9.2
degrees (range from 2-18). Subjectively, all patients were satisfied
with their results and stated they would have the procedure again. There
were no complications noted in the patients such as avascular necrosis,
Hallux varus, and recurrence of deformity. There were 6 delayed union
cases for 6 months, and one infection.
Conclusion: The
modified Mitchell’s osteotomy is an appropriate operative method that
produces satisfactory results, and can be recommended in the treatment
of moderate to severe Hallux valgus.
Key words: Modified Mitchell’s Osteotomy, Hallux valgus, Surgical outcome.
JRMS Dec 2003; 10(2): 6-10Introduction
Hallux valgus is a complex deformity of multifactorial etiology that causes pain, different shoe fitting, and dissatisfaction with the appearance of the foot. There are over 130 surgical procedures for the treatment of Hallux valgus, some include soft tissue procedures, others bony procedures and some combine both soft tissue and bony correction.
Hallux valgus was an uncommon deformity of the foot, until wearing fully enclosed shoes and boots was introduced (1-7).
The earliest mentioning of such deformity in the literature was in the eighteenth century. It is rarely seen in those who do not wear shoes.
Hawkins and associates (1) the first described the Mitchell operation for hallux valgus in literature in 1945.
C. Leslie Mitchell subsequently published an article in 1958 describing this procedure, and from this point on it became known as Mitchell bunionectomy including osteotomy of the distal portion of the first metatarsal, lateral displacement and angulation of the head of the metatarsal and bunionectomy and capsulorrhaphy (1,2,8,9).
The modified Mitchell’s osteotomy with Y-shape advancement of the medial capsule and lateral adductor tenotomy is recommended for correction of moderate to severe hallux valgus when pain and discomfort persist despite conservative treatment (1-3,8,10).
Numerous surgical procedures for correction of this deformity have been described, and the choice of procedure depends primarily on severity, location, and nature of the pathology.
Many factors are considered for Mitchell’s osteotomy, including general health, level of pain, range of movement, quality of bone and tissue, life style, foot wear and age (4,11-13).
The indications for Mitchell’s hallux valgus corrective osteotomy include:
1. Young patients with severe hallux valgus.
2. Moderate to severe pain
3. Deformity and joint instability.
4. Inability to wear normal footwear.
5. Failure of conservative treatment to restore the foot problem.
This procedure has been used at King Hussein Medical Center since 1993 for the correction of moderate and severe hallux valgus deformity of intermetatarsal (IM) angle >14º, and metatarsophalangeal (MTP) angle >32º. The purpose of this retrospective study was to review the results of all patients who have undergone modified Mitchell’s osteotomies with Y-shape advancement of medial capsule and lateral adductor tenotomy for hallux valgus between 1993 and 2001.
The IM angle is formed by the intersection of longitudinal axes of the first and second metatarsals. A normal angle is less than 9 degrees. The metatarsophalangeal angle (MTP) is formed by the intersection of longitudinal axes of the first metatarsal and the proximal phalanx. A normal angle is less than 15 degrees. (Fig. 1).
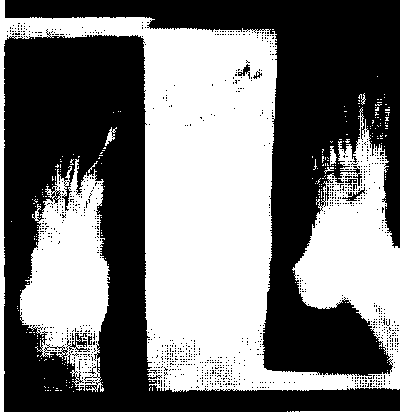
Fig. 1: Intermetatarsal (IM) angle and the metatarsophalangeal angle (MTP)
MethodsWe retrospectively studied 69 patients (84 feet) in whom modified Mitchell’s osteotomies with Y-shape advancement of the medial capsule and lateral adductor tenotomy were performed between 1993 and 2001 at King Hussein Medical Center in Jordan, for moderate to severe and painful hallu valgus, with average follow up of 30 months (10-48 months).
Female patients were 51; male patients were 18 (female to male ratio 2.8:1) right side 38 feet, left side 31 feet, and bilateral 30 feet in 15 patients.
The patients ranged in age from 16-47 years (average 23.7 years).
Indications for surgery included shoe problems, persistent pain and discomfort despite conservative management. Two surgeons performed the operations.
Weight-bearing dorsoplanter and lateral radiographs of the foot were obtained preoperatively and postoperatively and IM and MTP angles were measured. (Figs. 2, 3).
 Fig. 2:
Fig. 2: Preoperative weight bearing radiographs.
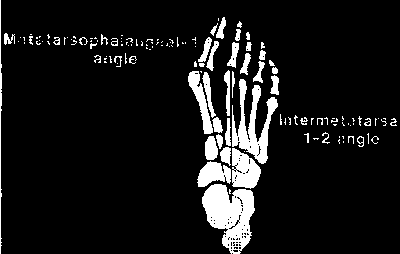 Fig. 3:
Fig. 3: Postoperative weight bearing radiographs.
The Modified Mitchell is OsteotomyThe Mitchell is osteotomy is a metatarsal osteotomy that displaces the metatarsal head slightly lateral ward in order to correct the hallux valgus deformity. This procedure can be conducted in deformities of any degree of severity.
Surgical TechniqueLongitudinal skin incision was centered over the dorsomedial aspect of the first metatarso-phalangeal joint and extended from the mid-portion of the proximal phalanx to the mid portion of the first metatarsal.
A V-Y capsular flap was created over the medial aspect of the MTP joint.
The medial eminence was exposed and the osteotomy created through a transverse cut in the metatarsal neck leaving a lateral piece of cortex about 3 mm wide. The second cut was made 2 mm more proximal and parallel to the first cut in order to create a step-off in the distal fragment.
Two dorsal to planter drill-holes were made: One in the distal fragment and the second hole in the proximal fragment about 1 cm apart.
The capital fragment was then displaced laterally until the lateral shelf locked over the lateral aspect at proximal fragment of the shaft.
The site of osteotomy was then fixed using non-absorbable sutures, through the two dorsal to planter drill-holes.
Capsular closure (medial capsulorrhaphy) The V-shaped incision then advanced into the straight limb of the Y-shaped incision while holding the hallux in planter flexion.
A 3 cm dorsal longitudinal incision was made centered over the first intermetatarsal space to expose the conjoined adductor tendon, the tendon was dissected from the lateral sesamoid bone, and the transverse intermetatarsal ligament was released. (Fig. 4).
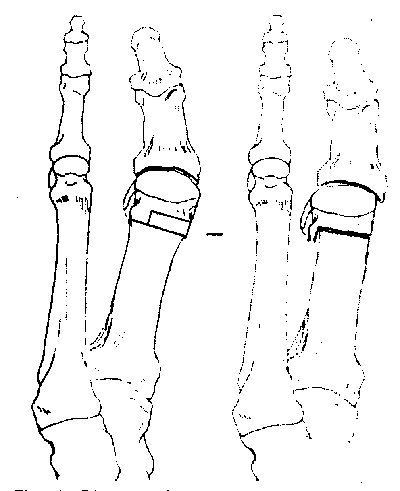
Fig. 4: Diagrammatic representation of Mitchell’s osteotomy.
Post-Operative CareThe patients remained non-weight bearing with crutches until sutures were removed at 14 days post operation. The foot was then placed in a non weight-bearing fiber- plaster cast which was removed at 6-8 weeks post operatively, after which walking was permitted with the foot immobilized in a below-knee cast until the site of osteotomy healed at 10 to 12 weeks, post-operatively.
ResultsThe patients were assessed before undergoing the operation and at follow-up of average of 30 months after operation. Assessment was made by interviews and clinical examination by the two authors. (Table I)
Table I:Clinical results in 69 patients.