ABSTRACT
Objective: To assess the clinical outcome
of patients with isolated ventricular septal defects small enough not to
require surgical closure.
Methods: Between January 2001
and May 2003 a total of 118 patients who were recently or previously
diagnosed to have isolated ventricular septal defects small enough not
to require surgical closure were included in this study. Inclusion
criteria for the study were single ventricular septal defect with a size
less than 5 mm in diameter on a 2-D echo, normal or borderline left
ventricular end diastolic diameter (20-44 mm), normal left ventricular
fractional shortening (0.30-0.40), normal or slightly raised pulmonary
artery pressure (less than 30/15 mmHg, with a mean less than 197 mmHg)
and absent ventricular septal defect-related clinical symptoms.
Exclusion criteria were symptomatic small ventricular septal defect
patients and those who had an additional hemodynamically relevant heart
defects. Follow up period was recorded.
Results: Mean
age of the study population at presentation was 13.3 +1.4 months (range,
one week-10 years) and at last follow-up visit 6.0+ 0.7 years (range
2.5-12.5 years). Follow-up was performed for 111 patients (94%). The
mean follow up period was 5.5+0.6 years (pre- and post enrollment).
Spontaneous closure was observed in 12 of perimembranous, and 10 of
muscular ventricular septal defects (overall rate of spontaneous closure
19.8%), by the end of the study. None of the patients died nor required
medical or surgical treatment. Two patients developed mild aortic
insufficiency and two patients had infective endocarditis during the
follow-up period. None of the patients had definite increasing
dimensions or functional deterioration of the left ventricle.
Twenty-five
patients underwent exercise treadmill testing; 84% of those achieved a
target heart rate more than 80% of age-predicted maximum heart rate.
None had a target less than 70% of predicted maximum heart rate or any
exercise-induced significant arrhythmias. On the other hand 21% showed
non-significant rhythm abnormalities either at resting electrocardiogram
or 24-hour Holter monitoring.
Conclusion: The overall
clinical outcome of asymptomatic children with small isolated
ventricular septal defect is excellent. Spontaneous closure may occur
and these children may be allowed to participate freely in physical
exercise and engage in competitive sports. Clinical and 2-D echo
follow-up are indicated.
Key words: Congenital, Septal defect, Outcome.
JRMS June 2005; 12(1): 10-14
Introduction
Most centers now report VSD as the most commonly encountered congenital cardiac lesion if one excludes a bicuspid aortic valve from consideration, as 20% of congenital heart patients have a VSD as a solitary lesion (1). The size of the VSD is the most helpful predictor of whether the patient will have symptoms; a VSD size >0.5 cm or VSD indexed for body surface area >1.8 cm/m2 was found to be a critical size for increased likelihood of developing symptoms (2).
Roger in 1879 first defined the clinical signs of an underlying VSD, the term Roger defect is used to indicate small VSDs (3) and the natural history of isolated ventricular septal defect (VSD) shows that many of these defects either close or diminish in size spontaneously (4,5,6). Clinicians have placed great importance on predicting the outcome of ventricular septal defects; the highly refined technique of Doppler echocardiography now makes it practical to document the very small ventricular septal defect and to follow its fate (7). In view of this we conducted this study to assess the clinical outcome of small ventricular septal defects.
Methods
The patients population consisted of 118 consecutive patients who had isolated small VSDs, considered too small to require surgical closure. There were 62 males and 56 females. All patients fulfilled the following inclusion criteria: 1. Absence of VSD clinically related symptoms (tachypnea, dyspnea, tiring when feeding, poor weight gain) or loud pulmonary component of the second heart sound. 2. Two-dimensional and Doppler echocardiography (2-DE) findings that include: isolated small VSD size (less than 5 mm in diameter), normal or borderline left ventricular end diastolic diameter (LVEDD) (20-44 mm), normal fractional shortening (0.30-0.40), and normal or slightly raised estimated pulmonary artery pressure (PAP) (less than 30/15 mmHg, with a mean less than 197 mmHg). Since not all defects are perfectly circular, the size of VSD was recorded at the maximal distance from any of the echocardiography imaging planes (i.e., parasternal long- and short-axis, apical, subcostal).
Exclusion criteria were symptomatic patients, and patients who had an additional hemodynamically relevant heart defects. The patient population represents the total number of patients, followed in the congenital heart disease program of Pediatrics Cardiology Division, in Queen Alia Heart Institute, Jordan.
Study protocol At first visit, the study protocol included: patient history, physical examination, electrocardiogram, chest x-ray and transthoracic 2-DE, all except chest x-ray were repeated in approximately every 6 to 12- months interval. In infants careful observation of the changes in VSD diameters by periodic 2-DE is important in predicting the clinical coarse and in deciding the operation indication (8). In older patients, it is indeed indicated to detect closure and complications of small VSDs (i.e., aortic insufficiency). 24-hour Holter monitoring during follow up was optionally performed in 57 patients (51%) and in order to assess their exercise capacity for the purpose of the study, we performed exercise treadmill testing in 25 patients (22.5%).
EchocardiographyStandard transthoracic two dimensional and Doppler echocardiography with Doppler color flow mapping was performed with a Hewlett-Packard 5500 sonos imaging system. A staff cardiologist reported all studies. Parasternal long- and short-axis, subcostal, and apical four-chamber views were routinely performed. The types of VSD were classified into: Perimembraneous, outlet, inlet, or muscular (diagram) (Fig. 1) (1). Perimembraneous VSDs were viewed in short axis image obtained from projection near the semilunar valves while muscular VSDs appeared in the short axis image obtained near the tip of mitral valve leaflets (1). Right ventricular systolic pressure was estimated with the peak pressure gradient from the tricuspid valve regurgitant jet. If no adequate Doppler signal of the tricuspid regurgitant flow could be obtained, pulmonary artery pressure was calculated by subtracting the left ventricular to right ventricular systolic gradient from the systemic arterial pressure.
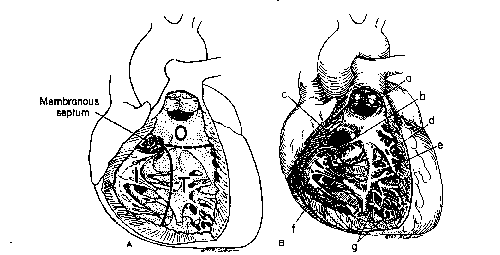
Fig. 1. A: Ventricular septum viewed from right ventricular side is made up of four components. I: Inlet component extends from tricuspid annulus to attachments of tricuspid valve. T: Trabecular septum extends from inlet out to apex and up to smooth-walled outlet. O: Outlet septum or infundibular septum, which extends up to pulmonary valve, and membranous septum.
B: Anatomic position of defects. a: Outlet defect
, b: Papillary muscle of the conus, c: Perimembranous defect, d: Marginal muscular defects, e: Central muscular defects, f: Inlet defect, g: Apical muscular defects.
Cardiac catheterization
Management of patients with VSD requires information regarding pulmonary artery pressure (PAP) (9). Noninvasive methods to assess PAP include: Doppler estimation of VSD gradient, ventricular hypertrophy, interventricular septal orientation, and VSD size had a predictive value for mean PAP (p<0.01). Only normal findings for all four significant variables did predict normal PAP. However, any other combination of normal and abnormal findings for the four significant variables did not reliably predict PAP and such patients might require catheterization to directly measure PAP (9).
A full hemodynamic study was performed in 52 selected patients (47%) who were suggestive to have large shunts on follow up as suggested by loud pulmonary component of second heart sound on auscultation, mild left ventricle hypertrophy (overload) on ECG, borderline LVEDD and/or raised estimated right ventricle pressure. In addition catheterization in these patients was done as preselection in preparing them for transcatheterizaion device closure of their VSDs with measurement of pressures, saturations, and calculation of the pulmonary to systemic flow ratio.
Follow- up
Between January 2001 to May 2003, patients were prospectively followed. Patients were seen in approximately 6 to 12-months interval. History, physical examination, echocardiogram, and electrocardiogram were repeated in each visit. Cardiac catheterization and hemodynamic study were performed in 52 patients. For the assessment of clinical outcome, the following events were defined: symptoms of heart failure, arrhythmias, development of aortic insufficiency or endocarditis, enlarging left ventricle or deteriorating left ventricle function, spontaneous closure of VSD and the major event of death.
Results
Seven patients were excluded from the study and the follow up was completed in 111 patients (94%). The mean age at presentation was 13.31.4 months (range, one week-10 years). While at the time of last visit, the mean age was 6.00.70 year (range 2.5 -12.5 years). There were 58 males and 53 females (52% males/48% females). The mean follow up of the entire study group was 5.50.60 years.
Clinically all patients were free of VSD related symptoms (tachypnea, dyspnea, tiring when feeding, poor weight gain) at time of presentation; referral to cardiac center was due to the accidental finding of systolic heart murmur during evaluation for other illnesses. No patient required medical or surgical treatment. Chest X-ray was done for every patient at the first time of presentation, where it showed normal cardio-thoracic ratio (less than 0.60 in infants and less than 0.50 in older children) in 104 patients (93.6%) and normal lungs vascularity in all patients.
Electrocardiogram which was done on first presentation and at every visit on follow up showed mild left ventricle hypertrophy (overload) by voltage in 21 patients (19%), evidenced by prominent R wave in lead II and prominent R and Q waves in leads V6 or peaked T wave in leads II and V6 (1). While incomplete right bundle branch block was found in 4 patients (3.6%), sinus arrhythmias and benign premature ventricular ectopies were found in 17 patients (15.3%).
Echocardiography was performed in each visit (every 6 to 12 months). The VSD size ranged from 0.1-0.5 cm at the time of first diagnosis. The types of VSDs were: Perimembraneous 79 (71.2%), outlet 3 (2.7%), inlet 2 (1.8%) and muscular type in 27 (24.3%). Left ventricle end -diastolic diameter (LVEDD) was measured and indexed for body surface area (BSA). Shortening fraction was measured. The mean (LVEDD) and LVEDDi (LVEDD/BSA) at last follow up visit were 2.80.6 and 8.51.7 cm respectively and the shortening fraction mean was 0.310.07. Considering both LVEDD and LVEDDi, the LV size was normal in 101 patients (91.0%), borderline in 10 patients (9.0%) but without deterioration during follow up and none had definitely enlarged LV. Estimated right ventricle systolic pressure was normal or slightly raised.
Spontaneous closure was observed in 12 (15%) of perimembranous, and 10 (37%) of muscular VSDs (overall rate of spontaneous closure 19.8 % by the end of the study). The age range at the time of closure was 6 months-10 years.
Exercise testing was feasible to perform in 25 patients. Of those 84% of patients had achieved a target heart rate more than 80% of age- predicted maximum heart rate for age (MHR). None had a target heart rate less than 70% of age predicted maximum heart rate (MHR) or developed any serious arrhythmias during the exercise testing. Twenty-four hour Holter monitoring optionally performed, for the purpose of the study, in 57 patients (51%). Of these none had pathological arrhythmias (i.e., multiform premature ventricular contraction, ventricular couplets, ventricular tachycardia).
At the end of the study, infective bacterial endocarditis was observed in two patients, one of them was strictly compliant to prophylaxis. On the other hand at the time of the last visit, only two patients were having mild aortic insufficiency (AI). These four patients were sent for surgical closure of their VSDs.
A total of 52 patients who had: Evidence of large shunt and/or raised estimated right ventricle pressure underwent cardiac catheterization. Many of these patients were selected for nonsurgical device closure of their VSDs. Mean pulmonary artery pressure was 226, and pulmonary to systemic flow ratio less than 1.5:1 in all of them.
Discussion
The management of isolated small VSDs remains controversial. Clinician assessment must be made of the size of the defect, the magnitude of hemodynamic overload, and the status of pulmonary vascular resistance (1).
Although our patients were asymptomatic, they were referred for cardiac evaluation, because of accidental finding of heart murmur, during evaluation for VSD misrelated symptoms or during routine check-up. All remained free of cardiac symptoms during the follow-up period. Our findings match those reported by Freedom et al (6), and Gabriel et al (10), where vast majority of patients remained asymptomatic.
The results of exercise testing were encouraging: 84% of patients who underwent exercise treadmill testing achieved a target heart rate >80% of age predicted maximum heart rate (MHR), none had a target less than 70% of predicted maximum heart rate (MHR) and none developed serious arrhythmias during exercise. On the other side with regard to left ventricle function, none of the patients had definite increasing dimensions or functional deterioration of the left ventricle. In two previous studies, 94% of patients with small VSDs were in New York Heart association functional class 1 (10,11). Since small VSDs are hemodynamically insignificant lesions and none developed serious arrhythmias during exercise, these children may be allowed to participate freely in physical exercise, and engage in competitive sports.
Detection of few types of benign arrhythmias by ECG, the 24-hour ECG monitoring, or during the exercise testing was observed in 21% of our patients while no serious arrhythmias have been detected. In small VSD the ECG is usually normal. However, a few demonstrated an rsr in lead v1 (1).
Freedom et al (6) reported only one patient in his series to have a chronic supraventricular tachycardia. In NHS-2 (11), a disconcertingly high percentage of all deaths were sudden and unexpected, which was attributed to the higher-than-normal prevalence of serious arrhythmias recorded during 24-hours ECG monitoring. Absence of serious arrhythmias may be responsible for no reported death in our study.
Regarding AI, outcome in our study group is excellent, since mild AI developed in only two patients (1.8%) during the period of follow-up. Our findings are consistent with those reported in NHS-2 where only four patients (0.7%) spontaneously developed AI after admission in the study (11) and the findings of Freedom et al (3.5%). The outcome is remarkably better than that reported by Backer et al (12) as aortic valve prolapse was observed in 45% of his group of patients and aortic insufficiency in 18%.
This is a 63% combined incidence, thus it is likely that the spectrum of disease severity differed from that in our population. Mehta et al confirmed that clinical or echocardiography aortic regurgitation is uncommon in the first five years of life (13). In contrast, frequency of AI associated with perimembranous VSD is approximately 10% in adolescents, and need long-term follow-up (14).
Endocarditis is still a major morbid event in patients with small VSDs.In our study (1.8%), one of the two patients who developed infective bacterial endocarditis was noncompliant to prophylaxis and our results are in agreement with previous reports (8-10,13). On the other hand Gresony et al (16) reported that the incidence of endocarditis was significantly less after VSD closure but not eliminated, whereas Kidd and associates reported from the NHS-2 (11) an endocarditis rate of 1.4 versus 1.6 per 1,000 patient-year for nonoperated and postoperative follow-up, respectively.
In the last thirty years, several authors have reported spontaneous closure of VSDs by various methods in children. Doppler color flow mapping has made the diagnosis, localization, and follow-up of VSD easy and more accurate (13). Reported closure rates vary with size and location of VSD, age at presentation and patients’ population. In NHS-2 spontaneous closure was reported in 15% of patients, which approaches our results (19.8%), whereas Mehta et al reported that overall spontaneous closure of VSD was 34% at one year (13). The higher rate in the last study could be explained by the fact that patients population were all infants, most of our patients were studied after infancy, and thus during a time in which spontaneous closure is less common. On the other hand our study has also showed that spontaneous closure of muscular VSDs is more frequent than that of perimembranous VSD (39% vs. 15%).
Shirali et al studied 156 cases and found a significantly higher spontaneous closure rate for muscular defects (17) and Du et al reported a higher rate (84.4%) of spontaneous closure of muscular VSDs in neonates (18).
The higher frequency and closure rate in muscular VSDs suggest that this is probably caused by improved diagnostic methods for finding these defects. With regard to type of VSD, Tomita et al came out with a conclusion that outlet VSDs close spontaneously in small percentage of patients (3.8%-4.3%) (19).
Surgical closure is recommended for only small defects with significant associated lesions such as aortic regurgitation, aortic valve prolapse, or recurrent endocarditis. Enlarging left ventricular size or deteriorating left ventricular function would also be an indication for surgical repair (5).
In our group, surgery is withheld in carefully selected patients; they have no symptoms, no signs of LV volume overload (on 2-DE), normal or slightly raised RV pressure, and small shunts (pulmonary : systemic flow <1.5:1.0). It has been previously reported that patients with small VSDs are unlikely to develop pulmonary hypertension and shunt flow is unlikely to increase with advancinage(16,18).
Conclusion
The overall clinical outcome of asymptomatic children with isolated small VSD is excellent. Spontaneous closure may occur and these children may be allowed to participate freely in physical exercise, and engage in competitive sports.
Clinical and 2-D echo follow up are indicated indefinitely, to emphasize the importance of prophylactic antibiotics for endocarditis, and to observe for occasional patients who develop aortic insufficiency, as both remain an indication for surgical closure of VSD.
References
1. Graham TP, Bender HW, Spach MS. Ventricular septal defect. In: Adams FW, Emmanouilides GC, ed. Moss” Heart disease in infant children and adolescents, including fetus and young adult. Baltimore: The William and Wilkins Co, 1995; 724-744.
2. Kimball TR, Daniels SR, Meyer RA, et al. Relation of symptoms to contractility and defect size in infants with ventricular septal defect. Am J Cariol 1991; 67: 1097-1102.
3. Roger H. Recherché cliniques sur la communication congenital des duex coeurs, par innoclusion du septum interventriculaire. Bull Acat Nat Med (Paris) 1879; 8: 1074.
4. Ramaciotti C, Keren A, Silverman NH. Importance of (Perimembraeous) ventricular septal aneurysm in the natural history of isolated perimembraneous ventricular septal defect. Am J Cardiol 1986; 57: 268-272.
5. King ME, de Moor M. Ventricular Septal Defect. Curr Treat Options Cardiovasc Med 1999; 1(4): 311-322.
6. Freedom RM, White RD, Pieroni DR, et al. The natural history of the so-called Aneurysm of the membranous ventricular septum in children. Circulation 1974; XLIX: 375-384.
7. Williams RG. Doppler color flow mapping and prediction of ventricular septal defect outcome. JACC 1989; 13(5): 1119-1121.
8. Ito T, Okudo T, Kimura M, et al. Increase in diameter of ventricular septal defect and membranous septal aneurysm formation during the infantile period. Pediatr Cardiol 2001; 22(6): 491-493.
9. Liberman L, Kaufman S, Alfayyadh M, et al. Noninvasive prediction of pulmonary artery pressure in patients with isolated ventricular septal defect. Pediatr Cardiol 2000; 21(3): 197-201.
10. Gabriel HM, Heger M, Innerhofer P, et al. Long-term outcome of patients with small ventricular septal defect considered not to require surgical closure during childhood. Am Coll Cardiol 2002; 39:1066-1071.
11. Kidd L, Driscoll DJ, Gersony WM, et al. Second Natural History Study of Congenital Heart Defects. Circulation 1993; 87:138-151.
12. Backer CL, Winters RC, Zales Vt R, et al. Restrictive ventricular septal defect: How small is too small to close. Ann Thorac Surg 1993; 56: 1014-1019.
13. Mehta AV, Guenca S, Chidambaram B, et al. Natural history of ventricular septal defect in the first five years of life. Tenn Med 2000; 93(4): 136-138.
14. Onat T, Ahunby G, Blamaz G, et al. The natural coarse of isolated ventricular septal defects in asdolescence. Pediatr Cardiol 1998; 19: 230-234.
15. Keith JD, Rose V, Collins G, Kidd BS. Ventricular septal defect. Incidence, morbidity, and mortality in various age groups. Br Heart J 1971; 33: 246-257.
16. Gersony WM, Hayes CJ, Driscoll DJ, et al. Bacterial endocaritis in patients with aortic stenosis, pulmonary stenosis, or ventricular septal defects. Circulation 1993; 87: 1121-1126.
17. Shirali GS, Smith EO, Geva T. Quantitation of echocardiographic predictors of outcome in infants with isolated perimembranous ventricular septal defects. Am Heart J 1995; 130: 1228-1235.
18. Du ZD, Roguin N, Wu XJ. Spontaneous closure of muscular ventricular septal defect identified by echocardiography in neonates. Cardiol Young 1998; 8(4): 423-424.
19. Tomita H, Arakaki Y, Yagihara T, Echigo S. Incidence of spontaneous closure of outlet ventricular septal defect. Jpn Circ J 2001; 65(5): 364-366.