ABSTRACT
Objective: To determine the frequency of pseudoexfoliation syndrome at Prince Ali Hospital Karak-Jordan.
Methods:
This study was conducted by the ophthalmology clinic at Prince Ali
Hospital in Karak province, between November 2003 to February 2004. A
total of 400 consecutive patients aged 40 years or above attending the
eye clinic were included in the study.
Results: The
frequency of pseudoexfoliation syndrome in Karak was found to be 21.3%
in subjects 40 years of age and above, 27.4% for patients 50 years of
age or above.
Conclusion: Further studies in other parts
of Jordan are needed to determine the incidence and prevalence of
Pseudoexfoliation syndrome in Jordan.
Key words: Pseudoexfoliation, Glaucoma, Prevalence.
JRMS June 2005; 12(1): 15-17IntroductionPseudoexfoliation syndrome (XFS) was first described in 1917 by Lindberg (1) in Finnish population. It is the most common identifiable cause of open angle glaucoma worldwide (2). The clinical diagnosis is made by the presence of typical pseudoexfoliation material (PXM) on the anterior lens capsule surface and at the pupillary margin. In addition to PXM, other features include endothelial pigmentation, loss of pupillary ruff, iris transillumination, Sampaolesi’s line, and pigment deposition in the trabecular meshwork (3).
PXS is associated with various ocular complications. Elevated intraocular pressure (IOP) and glaucomatous nerve damage had been demonstrated in patients with PXS (4-6). Cataracts were reported to be more common in patients with XFS (7). Unfavorable factors such as poor mydriasis (6,8-10), higher rate of vitreous loss (9,10), zonular weakness (9-12), corneal endotheliopathy (13), capsular phimosis, and opacification (14) have all been reported in relation to cataract surgery in these patients. PXM has been identified in various tissues in patients with ocular XFS (15). Systemic associations reported include angina, hypertension, myocardial infarction, stroke, and abdominal aortic aneurysm (16). The exact etiology and pathogenesis remain largely unknown (17). Hypothesis of an accumulation of basement membrane components such as fibrillin has been proposed (18).
It is a generalized disorder of the extracellular matrix characterized by the production of abnormal basement membrane-like material in several intraocular and extraocular tissues. The trigger for the production of PXM remains to be identified. Clinically, the PXM can be seen deposited in the anterior segment on the pupillary ruff, the anterior lens capsule, and other anterior segment structures. On the anterior capsule, it has a characteristic distribution of a central disc surrounded by a clear zone, surrounded by a peripheral ring-like deposit of granular material (19).
It has also been reported to be a risk factor for narrow angles and angle closure glaucoma (ACG) (6,20,22).
The prevalence of XFS in various populations has varied from 0% to 38% (22-31), and were reported to be: England 4% (22), Germany 4.7% (22), Norway 6.3% (22), Eskimos 0% (23), Russia 12% (23), Finland 22% (23), Iceland 29% (23) and 30% (24), Iran 9.6% (25), South Eastern United States 6% (26), Navajo Indians 38% (27), China 0.4% above 60 years of age (28), South India 3.8% (29), Black south Africans 7.7% in Hlabisa and 6.0% in Temba (30), and in France 5.5% (31).
MethodsA total of 400 consecutive patients attending the eye clinic at Prince Ali Hospital between November 2003 to February 2004, and aged 40 years or above, were examined for the presence of pseudoexfoliation. The relevant medical and ocular history was recorded. Eye evaluation included the visual acuity, slit lamp examination of the anterior segment with special attention to the endothelium, pupillary margin, anterior capsule with/without dilatation, and I.O.P. XFS was diagnosed clinically by the presence of typical PXM on the anterior capsule or at the pupil border, with or without pigment deposition on the corneal endothelium.
Glaucoma was diagnosed by the presence of characteristic glaucomatous nerve damage and/or field loss associated with raised IOP.
The collected data was analyzed according to age, gender, and laterality.
ResultsThe total number of patients included in this study was 400 [800 eyes], 169 (42.3%) males and 231 (57.7%) females, with age range from 40 to 85 years (Fig. 1). XFS was found in 85 (21.3%) patients [115 eyes (14.3%)], 35 (20.7%) males and 50 (21.7%) females. The youngest age found to have XFS was 50 years. No subjects under this age were found to have PXS. The ocular involvement was bilateral in 30 subjects (7.5% of all subjects and 35.3% among those with pseudoexfoliation (PXF); 12 (40%) females and 18 (60%) males, and it was unilateral in 55 subjects (13.8% among all subjects and 32.5% among those with PXF); 38 (69.1%) females and 17 (30.9%) males, and involving right eye in 35 (63.6%) subjects and left eye in 20 (36.4%) subjects.
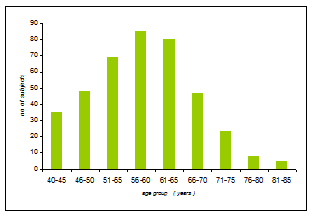
Fig. 1: Age distribution of the study population
The mean age of the study population was 58.9 years.
The mean age of subjects found to have PXS was 63 years, while the mean age of subjects without XFS was 57.8 years.
The mean age of females and males with XFS was 58.3 and 69.7 years respectively, however, the mean age of females and males included in the study was 52.03 and 64.62 years respectively.
Among the 115 eyes with PXF, 27 eyes (23.5%) were already diagnosed to have pseudoexfoliation glaucoma, while 6 more eyes (5.2%) were discovered to have it. So a total number of 33 eyes (28.7%) were found to have glaucoma.
DiscussionThe prevalence rate of XFS in different populations shows extensive variations – from 0% in Eskimos (23) to 38% in Navajo Indians (27). These variations arise from racial, genetic, and /or geographical differences.
Unfortunately, no reports are available in the literature on the prevalence of PXF from Arab nations. In our study, the frequency was found to be 21.3% in Karak, in patients 40 years of age and older, and 27.4% in patients 50 years and older. No significant sex predeliction was found, and this agrees with the results of other international studies (3,29). This implies a high prevalence of pseudoexfoliative glaucoma in this part of Jordan (27.8%), and this needs to be confirmed and more elaborated on in another study.
The mean age of subjects with XFS was found to be 63.0 years, and, considering age specific prevalence rates, there was a significant linear increase in prevalence with age (as shown in Table I). It is well known that the prevalence of XFS increases with age (5,26,29).
Table I: Age groups, frequency and percentage XFS.
|
Age group (years)
|
Population
|
No. of patients with XFS
|
%
|
|
40-45
|
35
|
0
|
0
|
|
46-50
|
48
|
1
|
2.1
|
|
51-55
|
69
|
9
|
13
|
|
56-60
|
85
|
22
|
25.9
|
|
61-65
|
80
|
24
|
30.0
|
|
66-70
|
47
|
16
|
34
|
|
71-75
|
23
|
8
|
34.8
|
|
76-80
|
8
|
3
|
37.5
|
|
81-85
|
5
|
2
|
40.0
|
|
Total
|
400
|
85
|
21.3
|
No significant age difference was found between bilateral and unilateral cases, and this is similar to those of other studies (29).
Further studies in other parts of Jordan are needed to determine the incidence and prevalence XFS in Jordan.
References
1. Lindberg JG. Kliniska undersokningar over depigmenteringen av pupillarranden och genomlysbarheten av iris vid fall av aldersstarrr samt i normala ogon hos gamla personer. Helsinki, Finland: Helsinki University, 1917; [Thesis]
2. Ritch R, Schlotzer-Schrehardt U. Exfoliation (Pseudoexfoliation) syndrome: Toward a new understanding. Acta Ophthalmol Scand 2001; 79: 213-217.
3. Prince AM, Ritch R. Clinical signs of the pseudoexfoliation syndrome. Ophthalmology 1986; 93: 803-807.
4. Davanger M, Ringvold A, Bilka S. Pseudo-exfoliation, IOP and glaucoma. Acta Ophthalmol 1991; 69: 569-573.
5. Mitchell P, Wang JJ, Hourihan F. The relationship between glaucoma and Pseudoexfoliation. The Blue Mountains Eye Study. Arch Ophthalmol 1999; 117: 1319-1324.
6. Layden WE, Shaffer RN. Exfoliation syndrome. Am J Ophthalmol 1974; 78: 835-841.
7. Hirvela H, Luukinen H,Laatikainen L. Prevalence and risk factors of lens opacities in the elderly in Finland. Ophthtalmology 1995; 102: 108-117.
8. Carpel EF. Pupillary dilatation in eyes with pseudoexfoliation syndrome. Am J Ophthalmol 1988; 105: 692-694.
9. Avramides A. Cataract surgery and lens implantation in eyes with exfoliation syndrome. J Cat Ref surg 1997; 23: 583-587.
10. Lumme P, Laatikainen L. Exfoliation syndrome and cataract extraction. Am J Ophthalmol 1993; 116: 51-55.
11. Allen JS. Zonular dialysis in pseudoexfoliation syndrome. Arch Ophthalmol 1987; 105: 1318-1319.
12. Shlotzer-Shrehardt U, Naumann GOH. A histopathologic study of zonular instability in pseudoexfoliation syndrome. Am J Ophthalmol 1994; 118: 730-743.
13. Wang L,Yamasita R, Hommura S. Corneal endothelial changes and aqueous flare intensity in pseudoexfoliation syndrome. Ophthalmologica 1999; 213: 387-91 (Med).
14. Kuchle M, Amberg A, Martus P, et al. Pseudoexfoliation syndrome, and secondary cataract. Br J Ophthalmol 1997; 81: 862-866
15. Shlotzer-Schrehardt U, Kocar MR, Naumann GOH, et al. Pseudoexfoliation syndrome: Ocular manifestation of a systemic disorder? Arch of Ophthalmol 1992; 110: 1752-1756.
16. Schumacher S, Schlotzer-Schrehardt U, Martus P, et al.Pseudoexfoliation syndrome and aneurysms of the abdominal aorta. Lancet 2001; 357: 359-360.
17. Damji KF, Bains HS, Stefansson E, et al. Is pseudoexfoliation syndrome inherited? A review of genetic and nongenetic factors and a new observation. Ophthalmic Genetics 1998; 19: 175-185.
18. Schlotzer-schrehardt U, von der Mark K, Sakai LY, et al. Increased extracellular deposition of fibrillin-containing fibrils in pseudoexfoliation syndrome. Invest Ophthalmol Vis Sci 1997; 38: 970-984.
19. Ritch R. Exfoliation Syndrome. In: Ritch R, Shields MB, Kruoin T, editors. The glaucomas, 2nd ed. St Louis: Mosby, 1996; 993-1022.
20. Wishart PK, Spaeth GL, Poryzees EM. Anterior chamber angle in pseudexfoloiation syndrome. Br J Ophthalmol 1985; 69: 103-107.
21. Gohdo T, Takahashi H, Ijima H, et al. Ultrasound biomicroscopy of angle closure glaucoma with pseudoexfoliation syndrome. Br J Ophthalmol 1997; 81: 705.
22. Aasved H. The geographical distribution of fibrillopathia epitheliocapsularis, so- called senile exfoliation or pseudoexfoliation of the anterior capsule. Acta Ophthalmol 1969; 47: 792-810.
23. Forsius H. Prevalence of pseudoexfoliation of the lens in Finns Lapps, Icelanders, Eskimos and Russians. Trans Ophthalmol Soc 1979; 99: 296.
24. Allingham RR, Loftsdottir M, Gottfredsdottir MS, et al. Pseudoexfoliation syndrome in Icelandic families. Br J Ophthalmol 2001; 85: 702-707.
25. Nouri-Mahdavi K, Nosrat N, Sahebghalam R, et al. Pseudoexfoliation syndrome in central Iran: a population-based survey. Acta Ophthalmol Scand 1999; 77: 581-584.
26. Cashwell LF, Shields MB. Exfoliation syndrome; prevalence in a southeastern United States population. Arch Ophthalmol 1988; 106: 335-336.
27. Faulkener HW. Pseudoexfoliation of the lens among Navajo Indians. AM J Ophthalmol 1971; 72: 206.
28. Young AL, Tang WW, Lam DSC. The prevalence of pseudoexfoliation in Chinese people. Br J Ophthalmol 2004; 88: 193-195.
29. Arvind H, Raju P, Paul PG, et al. Pseudoexfoliation in south India. Br J Ophthalmol 2003; 87: 1321-1323.
30. Rotchford AP, Kirwan JF, Johnson GJ, Roux P. Exfoliation syndrome in black South Africans. Arch Ophthalml 2003; 121(6): 863-870.
31. Ritch R. Exfoliation syndrome: Clinical findings and occurrence in patients with occludable angles. Trans Am Ophthalmol Soc 1994; 92: 845-944.