ABSTRACT
In this case report, we describe a case of large
omphalocele in which spleen was one of the contents in addition to the
liver and bowel.
Key words: Omphalocele, Gastroschisis, Karyotype, Spleen.
JRMS June 2005; 12(1): 35-37
A 34-year-old woman, gravida 3 para 2, presented for fetal scanning at 24 weeks of gestation. The fetus was noted to have ascites and omphalocele containing liver, bowel, and suspicious spleen, because it was difficult to visualize the spleen in the fetal abdomen (Fig. 1) Skeletal and cardiac abnormalities were noted including: spine and lower limbs deformity, and ventricular septal defect (VSD). Amniocentesis yielded trisomy 18. Repeated ultrasonography at 28 and 32 weeks of gestation confirmed the presence of the omphalocele and normal fetal growth. The choice of termination was discussed with the parents, but they elected continuation of pregnancy. The patient presented with premature rupture of membranes at 33 weeks gestation and vaginal delivery of a 2350-gm baby took place. The baby died 15 minutes after delivery. The omphalocele contained bowel, liver, and spleen (Fig. 2). Skeletal abnormalities were obvious in the chest and lower limbs.
Discussion
Omphalocele is a common group of birth defect that is related to the anterior abdominal wall, with a reported incidence of nearly 2.5 cases per 10.000 live births (1). This defect is associated with a high rate of concurrent malformations, chromosomal anomalies, and fetal mortality (2-9).
Abnormalities of the cardiovascular, skeletal, gastrointestinal, genitourinary tract, and central nervous system are seen in more than 50% of cases, and the associated chromosomal abnormalities are typically present in more than one-third of omphalocele cases (2,3). Contents of this abnormality are usually bowel, liver, or both (1-9), but spleen may be rarely contained (10,11).
During the 6th week of embryonic development, rapid growth of the bowel causes the intestinal loops to enter the extraembryonic coelom. By the next few weeks, further elongation of the intestinal loops occurs along with a 270-degree rotation. The herniated loops of the intestines usually return to the abdominal cavity by the end of the third month, and the failure of this to occur, will result in an omphalocele (4). At birth, the herniated loops of intestine with the possible accompanying large bowel and liver are covered with amnion, parietal peritoneum and a thin connective tissue.
Omphalocele is associated with high rate of concurrent malformations, chromosomal anomalies and fetal mortality. The rate of concurrent anomalies was reported to range between 67% to 88% (5-7). In these studies, concurrent malformations were the most significant predictor of subsequent death, and this statistical significance was unchanged whether or not chromosomal anomalies were considered. Many investigators suggested that the size or contents of the omphalocele may be of important prognostic value; also, a strong association between omphalocele contents and chromosomal abnormality was reported (5,7). Getachew et al (8) reported that 87% of fetuses with omphalocele containing only bowel had an abnormal karyotype, which is significantly higher rate than in those fetuses whose omphalocele contained liver (9%). Same findings were reported by Hughes et al (6).
Fetuses with trisomy 18 are associated with high mortality rate that related to the higher incidence of concurrent abnormalities associated with this syndrome (12). The most frequent abnormalities reported by these investigators include: Intrauterine growth retardation, cardiac defects, digestive abnormalities, limb abnormalities, cystic hygroma, omphalocele, diaphragmatic hernia, and facial dysmorphism. Our case represents an omphalocele that contained bowel, liver and spleen with skeletal and cardiovascular abnormalities, and abnormal karyotype. Because there was no sufficient data about cases of omphalocele that contain spleen, further reports are needed to determine the incidence of chromosomal anomalies associated with abdominal wall defect. Omphalocele should be distinguished from gastroschisis, another fetal abdominal wall abnormality that consists of a full-thickened abdominal wall defect with subsequent herniation of small bowel and occasionally large bowel.
Liver rarely if ever protrudes through the defect; if it is seen, one can usually exclude the diagnosis of gastroschisis (4). Furthermore, associated chromosomal abnormalities are unusual in gastroschisis, and concurrent anomalies are seen in approximately 13% of cases. Most of these abnormalities are gastrointestinal, where the majority in omphalocele is extraintestinal including: cardiovascular, skeletal, genitourinary, and central nervous system anomalies (9). Ultrasonographically, omphalocele can be distinguished from gastroschisis. The imaging in the transverse view can diagnose most omphaloceles by noting tissue protruding into the base of the umbilical cord or by visualizing bowel or liver within a sac, while in gastroschisis the herniated loops of bowel are freely visualized in the amniotic cavity, to the right of the umbilical cord insertion site (4).
The optimal mode of delivery for fetuses with antenatally diagnosed abdominal wall defects has been the subject of intense controversy. In a recent study, How et al (13) reported that these fetuses may safely be delivered by the vaginal route, and cesarean delivery should be performed for obstetric indications only. In their study, they found no statistically significant difference in the rates of neonatal death and neonatal sepsis for cesarean versus vaginal delivery. On the other hand, other investigators emphasized that elective cesarean section improves the outcome of neonates with abdominal wall defect (14). In our case, because of the gestational age, abnormal karyotype, and the concurrent malformations, the vaginal route for delivery was chosen following discussion with the parents.
In conclusion, omphalocele containing liver and spleen is most likely to be associated with abnormal karyotype with subsequent poor fetal or neonatal outcome. Pregnancy termination options should be discussed with the family depending upon the gestational age of the fetus and local legal limits for such procedure. For families that elect pregnancy continuation, serial sonography is recommended to detect any alteration in fetal growth as well as other sonographic evidence of fetal compromise. In the former situation, careful consideration should be given to a planned delivery usually undertaken abdominally at a time when not only is neonatal expertise available, but also surgical facilities for highly complex neonatal surgery with the support of neonatal intensive care unit postoperatively.
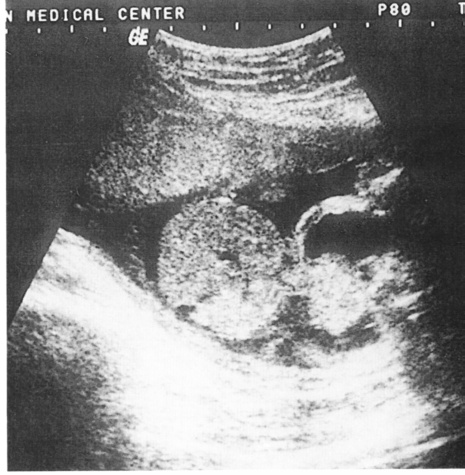 Fig. 1:
Fig. 1:Fetal ultrasound at 24 weeks of gestation shows fetal ascites and large omphalocele containing bowel, liver and suspicious spleen.
 Fig. 2:
Fig. 2: Ruptured omphalocele containing bowel, liver and spleen.
References
1.
Calzolari E, Bianchi F, Dolk H, et al. Omphalocele and gastroschisis in Europe: A survey of 3 million births, 1980-1990. Am J Med Genet 1995; 58: 187.
2.
De Veciana M, Mijor CA, Porto M. Prediction of an abnormal karyotype in fetuses with omphalocele. Prenat Diagn 1994; 14: 487.
3.
Tucci M, Bard H. The associated anomalies that determine prognosis in congenital omphalocles. Am J Obstet Gynecol 1990; 163: 1646.
4.
Martin RW. Screening for fetal abdominal wall defects. Obst Gyn North America 1998; 25: 517.
5.
Nyberg DA, Fitzsimmons J, Mack LA, et al. Chromosomal abnormalities in fetuses with omphalocele: The significance of omphalocele contents. J Ultrasound Med 1989; 8: 299-308.
6.
Hughes MD, Nuberg DA, Mack LA, Pretorius DH. Fetal omphalocele: Prenatal US detection of concurrent anomalies and other predictors of outcome. Radiology 1989; 173: 371.
7.
AXT R, Quijano F, Hendrik HJ, et al. Omphalocele and gastroschisis: Prenatal diagnosis and peripartum management. A case analysis of the years 1989-1997 at the Department of Obstetrics and Gynecology, University of Homborg/Saar. Eur J Obstet Gynecol Reprod Biol 1999; 87: 47-54.
8.
Getachew MM, Goldstein RB, Edge V, et al. Correlation between omphalocele contents and karyotypic abnormalities: Sonographic study in 37 cases. AJR Roentgenol 1992; 158: 133.
9.
Fisher R, Attah A, Partington A, et al. Impact of antenatal diagnosis on incidence and prognosis in abdominal wall defects. J Pediatr Surg 1996; 31: 538.
10.
Williams JL, Bush D, Wright PG. Omphalocele and ectopic spleen. J Clin Ultrasound 1987; 15: 409-411.
11.
Delarue A, Camboulives J, Bollini G, et al. Delayed cure of an omphalocele requiring abdominosternoplasty, right hepatectomy and partial splenectomy. Eur J Pediatr Surg 2000; 10: 58-61.
12.
Brun L, Dufour P, Savary JB, et al. Trisomy 18: Ultrasound aspects. Report of 40 cases. Presse Med 2000; 29: 2082-2086.
13.
How HY, Harris BJ, Pietrantoni M, et al. Is vaginal delivery preferable to elective cesarean delivery in fetuses with a known ventral wall defect. Am J Obstet Gynecol 2000; 182: 1527-1534.
14.
Sakala EP, Erhard LN, White JJ. Elective cesarean section for improving outcome of neonates with gastroschisis. Am J Obstet Gynecol 1993; 169: 1050.