Introduction
Congenital left atrial appendage (LAA) aneurysm is a very rare condition, with only about 50 cases reported in the literature worldwide. As it has the potential for serious sequelae that include various arrhythmias and systemic emboli (1,2), surgical removal is indicated even in asymptomatic cases (3).
Case Report
A 21-year-old male was referred to our outpatient cardiology clinic at Queen Alia Heart Institute (QAHI)/ King Hussein Medical Center (KHMC) for further evaluation upon the incidental finding of atrial fibrillation and an abnormal chest X-ray on a routine pre-recruitment medical screening for the Jordan Armed Forces. Upon further inquiry he admitted a history of paroxysmal palpitations and shortness of breath on moderate exertion. Clinical examination was unremarkable except for an irregularly irregular pulse.
His ECG showed atrial fibrillation with controlled ventricular rate and narrow QRS complex (Fig. 1). The chest X-ray revealed an increased cardiothoracic ratio of 70% (Fig. 2) with an abnormally prominent left upper cardiac border. Trans-thoracic echocardiography showed distortion of the left ventricle by an intra-pericardial cystic mass. Transesophageal echocardiography (TEE) showed LAA aneurysm with spontaneous contrast and a distorted left ventricle (Fig. 3 and Fig. 4). The aneurysm measured a 16 x 10 x 11 cm, and there was no evidence of a thrombus.
He subsequently underwent right and left heart catheterization that showed normal hemodynamic parameters. Left ventriculography and coronary angiography showed distortion of the left ventricular free wall and cavity (Fig. 5) and a distorted left anterior descending artery course (Fig. 7).
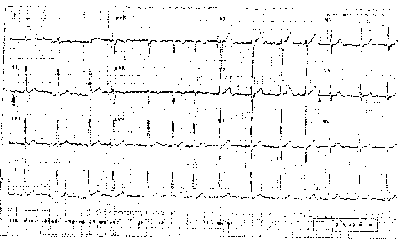 Fig.1:
Fig.1:Pre-operative ECG, showing atrial fibrillation with controlled ventricular rate and narrow QRS complex.
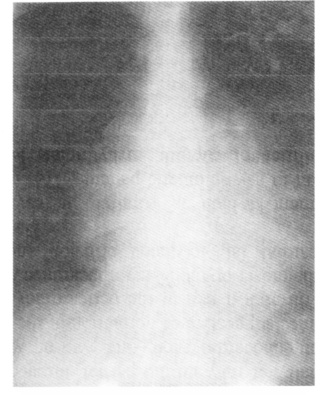 Fig. 2:
Fig. 2:Pre-operative CXR, showing an increased cardiothoracic ratio of 70% with an abnormally prominent left upper cardiac border.
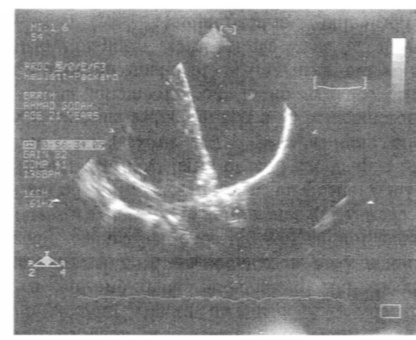 Fig.3:
Fig.3:Left Ventricle during diastole.Transesophageal Doppler echocardiography showing a left atrial appendage aneurysm with spontaneous contrast and a distorted left ventricle.
 Fig. 4:
Fig. 4:Left Ventricle during systole. Transesophageal echocardiography showing a left atrial appendage aneurysm with spontaneous contrast and a distorted left ventricle.
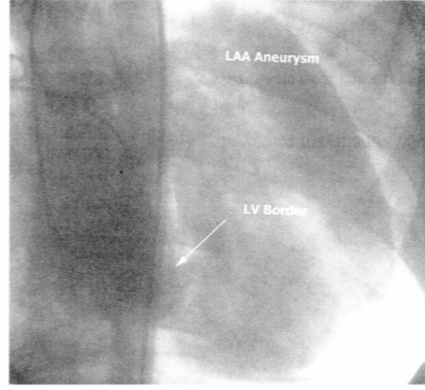
Fig. 5:Postero-anterior view of left atrial contrast injection showing distortion of the left ventricular free wall and cavity by the large left atrial appendage aneurysm.
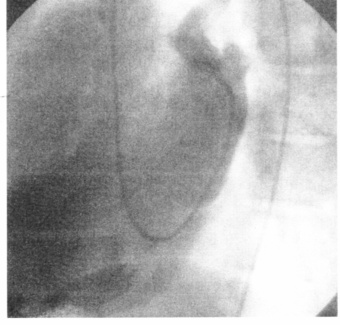 Fig. 6:
Fig. 6: Lateral view of left atrial contrast injection.
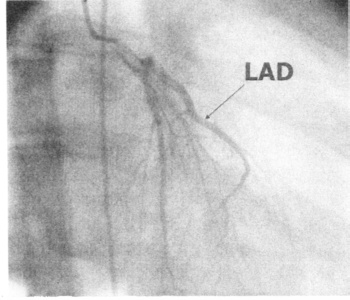 Fig. 7:
Fig. 7: Postero-anterior view of left coronary angiogram showing a displaced left anterior descending artery course.
A 6F pigtail catheter was passed retrograde through the mitral valve into the left atrium. Left atrial contrast injection showed a huge left atrial appendage aneurysm measuring 16.5 x 10.5 x 11.8 cm. Figures 5 and 6 show antero-posterior and left lateral views. Left atrial aneurysm contrast injection was avoided because of the risk of rupture. Under partial cardiopulmonary bypass, he underwent surgical excision of the LAA (Fig 8 and Fig 9). The pericardium was found to be intact. Histopathology showed a sac-like structure measuring 17 x 12 cm that was composed of three myocardial layers of different thickness. They included epicardial, myocardial and endocardial layers. His post-operative course was uneventful, and was discharged home 6 days later. After surgical excision his cardiac rhythm spontaneously reverted to sinus rhythm, which was maintained upon at follow-up twelve months later. Figure 10 shows his post-operative chest X-ray with a cardiothoracic ratio of 55%.
 Fig. 8:
Fig. 8:Aneurysm in-situ.
 Fig. 9:
Fig. 9: Aneurysm removed.
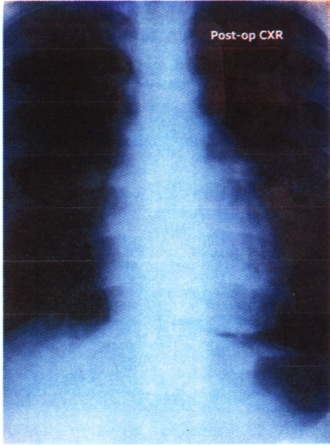
Fig. 10:Postoperative CXR, showing a normal cardiothoracic ratio.
Discussion
LAA aneurysm is an extremely rare cardiac anomaly in which the pericardium is intact and there is no primary disease causing dilatation of the atrium. The aneurysm is attributed to congenital dysplasia of the musculi pectinati in the left atrial appendage and of the bands of the atrial muscle from which they arise (4).
Around fifty cases have been reported so far worldwide. LAA aneurysm usually presents during childhood, but presentation later on life is not uncommon. Late presentation has been described as an incidental finding (e.g. an abnormal cardiac silhouette on a chest X-ray done during pre-operative assessment) (5). LAA aneurysm may present with shortness of breath, palpitations (due to atrial tachyarrhythmias) (6), embolic complications (1,4,7) (e.g. strokes) and even chest pain accompanied by a rise in cardiac enzymes (due to extrinsic compression of the left anterior descending artery by the aneurysm) (8). In infants or children, the aneurysm can cause cardiac arrest, respiratory distress, atrial fibrillation (9), or heart failure (6,10).
In the past, chest X-ray, transthoracic echocardiography, cardiac catheterization and even exploratory thoracotomy have been used to confirm the diagnosis. In recent years, TEE and chest MRI proved to be useful for the detection and diagnosis of this anomaly (2,11,12). Occasionally, it may mimic partial absence of the pericardium on echocardiography and even on MRI, giving an appearance suggestive of herniation of the left atrial appendage through a gap in the pericardium (13). The differential diagnosis of the X-ray appearance also includes an epicardial fat, loculated effusion and a mediastinal mass.
Surgical treatment, which is curative, is usually recommended even in asymptomatic patients. This is to avoid the possibilities of rupture, arrhythmias, heart failure, or thromboembolism. Surgical resection with or without cardiopulmonary bypass (2,6,14) has been reported, with no reports of recurrence. On the other hand, the prognosis of asymptomatic congenital absence of the pericardium is thought to be good and some patients have been followed up without needing any surgical treatment. However, congenital absence of the pericardium can rarely cause cardiac incarceration, that can cause acute myocardial infarction, sudden death, cerebral thrombosis or multiple thrombosis (15,16).
We believe that the size of the LAA aneurysm in our case is the largest ever been reported in the literature. It was picked up on a routine pre-recruitment medical screening and had classical findings. Our patient had mild clinical symptoms and atrial fibrillation for which he did not seek medical advice. The surgical treatment was curative and the cardiac rhythm returned to normal sinus rhythm.
Conclusion
Left atrial appendage aneurysms are rare congenital cardiac anomalies that may be asymptomatic or present with shortness of breath, palpitations and embolic complications. Surgical excision even in asymptomatic is recommended and is curative.
References
1.
Gold JP, Afifi HY, Ko W, et al. Congenital giant aneurysms of the left atrial appendage: Diagnosis and management. J Card Surg 1996; 11: 147-150. (Abstract)
2.
Burke RP, Mark JB, Collins JJ Jr, Cohn LH. Improved surgical approach to left atrial appendage aneurysm. J Card Surg 1992; 7: 104-107. (Abstract)
3.
Moralis JM, Patel SG, Jackson JH, et al. Left atrial aneurysm. Ann Thorac Surg 2001; 71: 719-722.
4.
Victor S, Nayak VM. Aneurysm of the left atrial appendage. Tex Heart Inst J 2001; 28(2): 111-118.
5.
Park JS, Lee DH, Han SS, et al. Incidentally found, growing congenital aneurysm of the left atrium. J Korean Med Sci 2003; 18(2): 262-266.
6.
Pomerantzeff PM, Freyre HM, de Almeida Brandao CM, et al. Aneurysm of the left atrial appendage. Ann Thorac Surg 2002; 73(6): 1981-1983.
7.
Wagshal AB, Applebaum A, Crystal P, et al. Atrial tachycardia as the presenting sign of left atrial appendage aneurysm. Pacing Clin Electrophysiol 2000; 23: 283-285. (Abstract)
8.
Frambach PJ, Geskes GG, Cheriex EC, et al. Giant intrapericardial aneurysm of the left atrial appendage. Eur Heart J 1990; 11(9): 848-853. (Abstract)
9.
Brigui M, Ennabli K, Remadi F, et al. Severe aneurysmal dilatation of the left atrium. Apropos of a case. Arch Mal Coeur Vaiss (Article in French) 1994; 87(12): 1749-1753. (Abstract)
10.
Stone KS, Brown JW, Canal D, et al. Congenital aneurysm of the left atrial wall in infancy. Ann Thorac Surg 1990: 49: 476-478.
11.
Hoffmann U, Hamed N, Herold C, Globits S. Radiological signs of a left atrial aneurysm. Eur Radiol 2000; 10(8): 1332-1334. (Abstract)
12.
Cujec B, Bharadwaj B, Orchard RC, Lopez JF. Transesophageal echocardiography in the diagnosis of left atrial appendage aneurysm. J Am Soc Echocardiogr 1990; 3(5): 408-411. (Abstract)
13.
Kunishima T, Musha H, Yamamoto T, et al. Congenital giant aneurysm of the left atrial appendage mimicking pericardial absence. Case report. Jpn Circ J 2001; 65(1): 56-59.
14.
Zhao J, Ge Y, Yan H, et al. Treatment of congenital aneurysms of the left atrium and left atrial appendage. Tex Heart Inst J 1999; 26(2): 136-139. (Abstract)
15.
Saito R, Hotta F. Congenital pericardial defects associated with cardiac incarceration. Am Heart J 1980; 100: 866-870.
16.
Williams WG. Dilatation of the atrial appendage. Br Heart J 1963; 25: 637-643.