Objective: To assess the results of minimally invasive cardiac valve surgery at Queen Alia Heart Institute.
Methods: The medical records and operative notes of 60 consecutive patients, who underwent minimally invasive valve surgery with or without other concomitant surgical cardiac procedures at Queen Alia Heart Institute between February 1997 and August 2003, were retrospectively reviewed.
Results: A satisfactory valve repair and/or replacement were performed in 58 cases through a minimally invasive approach. Conversion to classical midsternotmy was done in two cases (3.3%). Mean incision length was 6 cm (range 5-7). Mean duration of operation, cardiopulmonary bypass, and cross clamp time was 150, 70, and 35 minutes respectively. Mean duration of intensive care unit stay was 30 hours (range 24 to 36 hours) and mean duration of hospital stay was 4 days (range 3 to 5 days).
All patients were discharged from hospital. Postoperative wound infection and neurological deficits were not noticed. All patients had a speedy recovery with less pain and trauma. At mean follow-up of 12 months (range 1 month to 6 years) all patients were alive and in NYHA functional class I.
Conclusion: Minimally invasive valve surgery is technically feasible, safe and provides adequate exposure for valve repair and/or replacement in selected cases. It allows rapid recovery and early hospital discharge. Case selection and more technical experience are needed to further evaluate the early and long-term outcome of this procedure.
Key words: Minimally Invasive, Valve Surgery, Assessment of results
JRMS Dec 2005; 12(2): 14-17
Introduction
Cardiac valve surgery is traditionally performed via median sternotomy with direct aortic and right atrial cannulation for cardiopulmonary bypass. An alternative to this is direct-access minimally invasive valve surgery through an upper ministernotomy or right anterolateral minithoracotomy approach which was attempted in selected cases and our objective was to assess the results of this approach at Queen Alia Heart Institute (QAHI).
Patient Selection
Patients of average weight and height, and with non-calcific or mildly calcified valves were selected to be operated upon using minimally invasive techniques. Patients with concomitant coronary artery disease, calcifying pericarditis, morbid obesity, gross thoracic boney deformity, aneurysms of ascending aorta, poor ejection fraction, aortic stenosis that necessitated annular enlargement, and or mitral valve disease requiring chordal reconstruction for anterior mitral leaflet were excluded.
Technique
Two approaches were used in this group of patients: Upper ministernotomy in 57 patients, and right anterolateral minithoracotomy in 3 patients.
Upper Ministernotomy Approach
The patient is anesthetized in the supine position and intubate. The jugular notch and the midpoint of the body of the sternum at fourth interspace are marked as the primary reference points. A 5-7 cm longitudinal skin incision is made at the midpoint between these two reference points. The two flaps are raised above and below to the level of the two primary reference points.
The periosteum over the sternum is incised vertically from the suprasternal notch to the level of the fourth interspace. The sternum is first divided transversely at the level of the fourth interspace and then vertically to the level of the suprasternal notch, i.e. inverted T shape using an oscillating sternal saw. Once the initial separation has been achieved, a small retractor is introduced in the cleft between the two vertical halves of the sternum and retraction is effected. The pericardium is opened vertically and retracted. Cannulation of the ascending aorta and right atrium is achieved easily for establishing cardiopulmonary bypass.
Discontinuation of ventilation during cardiopulmonary bypass allows access to the right superior pulmonary vein for the insertion of a vent. Delivery of cardioplegia is achieved by the antegrade and or retrograde method according to the individual requirement.
Replacement of the aortic valve is performed by a standard operative technique under CO2 hood at 3L/minute through a cannula which is placed at the wound edge to help reduce the potential for air emboli, this displaces oxygen and nitrogen in the operative field and therefore any remained bubbles of CO2 in circulation after efficient deaeration are rapidly absorbed.
After repair of the aortotomy, the heart is allowed to fell with blood with suction in the aortic root and the left ventricular vent, de-airing is accomplished. Pediatric defibrillator pads introduced through the ministernotomy incision, if necessary, can perform defibrillation. After the patient is weaned off cardiopulmonary bypass the cannula are removed and the heparin is reversed.
The mitral valve can be approached through the same ministernotomy incision, through the roof of left atrium where repair or replacement of the mitral valve using either the continuous or interrupted suture technique can be done easily. The ministernotomy is closed with 3 or 4 wires over a single pericardial drain. Figure (1: a-b)
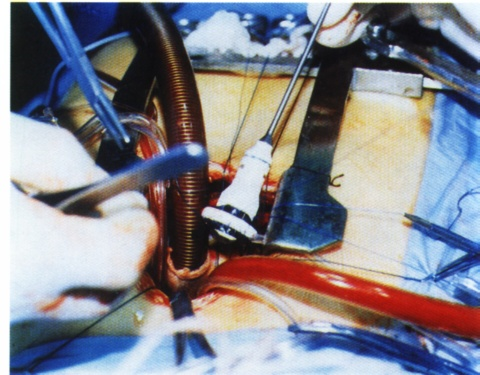 Fig. 1(a):
Fig. 1(a): Minimally invasive AVR through upper ministernotomy incision.
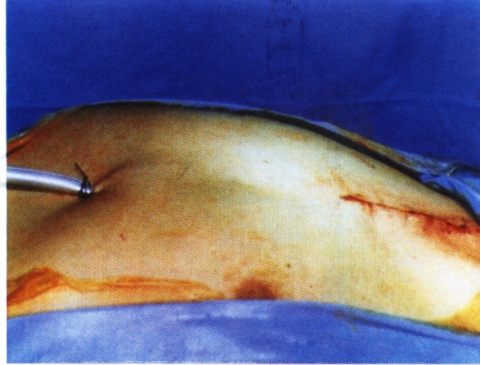
Fig. 1(b):Upper ministernotomy incision is closed, single pericardial drain inserted.
Right Anterolateral Minithoracotomy Approach
The patient is anesthetized in a semilateral position, 40 right up and groins horizontal, and the patient is intubated with a double lumen endotracheal tube to deflate the right lung for better exposure. A sub mammary 6 cm incision is done, pericardial cavity is opened, and edges of pericardium are retracted. This facilitates exposure to the right and left atria.
Femoral cannulation is done in the usual manner, aortic cross clamp applied through the minithoracotomy incision, then the mitral and/or tricuspid valve can be exposed, repaired, or replaced through left and/or right atria under CO2 hood. After the arteriotomy is closed, decannulation is done and closure of minithoracotomy incision is performed in layers over a single chest tube.
Results
Between February 1997 and August 2003 sixty patients underwent minimally invasive valve surgery with or without other concomitant surgical cardiac procedures using one of the above two approaches. Mean patients weight and height were 74 Kg (range 42-86) and 168 cm (range 154 –180), respectively.
Upper ministernotomy approach was used in 57 patients: Thirty nine patients underwent isolated AVR, 4 MVR, 3 mitral valve repair, 4 combined AVR+MVR, 5 AVR+mitral valve repair, 1 AVR plus excision of SAM, and 1 Redo AVR.
Right minithoracotomy approach was used in 3 patients: 2 Redo MVR and 1 for tricuspid valve repair.
A satisfactory valve repair and/or replacement were achieved in 58 cases. Conversion rate to classical midsternotmy was needed in two cases (3.3%), 1 because of uncontrolled bleeding from aortotomy site and the other due to slipping of pacemaker wire needle into the pericardial cavity.
The mean length of incision was 6 cm (range 5 to 7cm). The mean duration of operation, cardiopulmonary bypass, and cross clamp time was 150, 70, and 35 minutes respectively. The aortic cross clamp time was a mean of 30 minutes for isolated AVR and 45 minutes for AVR with concomitant surgical procedures. Mean intubation time was 6 hours (range 4 to 8 hours).
Mean duration of intensive care stay was 30 hours (range 24 to 36 hours) and mean duration of in-hospital stay was 4 days (range 3 to 5 days). All patients had speed recovery and survived hospitalization. No wound infection or postoperative neurological deficit was noticed in any of the patients. One patient needed to be reoperated upon because of prosthetic aortic valve endocarditis two months after his first surgery whereby Re-do AVR was done successfully through the same upper ministernotomy approach.
At mean follow-up of 12 months (range from 1 month to 6 years), 96% were in functional class I, with resumption of normal activity. Postoperative echocardiography showed excellent valve function in all cases except one patient who developed prosthetic endocarditis two months postoperatively.
Discussion
Minimally invasive surgical techniques have proliferated at a staggering rate in the last decade. Cardiac surgery has been a late entrant in this process but is currently experiencing a surge of interest in the techniques for minimally invasive approaches that, it is hoped, will decrease patient discomfort, operative morbidity, length of hospitalization, and cost, improve cosmetic healing and facilitate return to normal function while not comprising short-or-long-term outcomes of the surgical procedure or increased difficulty for the surgeon. Whilst most definitions of less invasive coronary surgery include the phrase without cardiopulmonary bypass, this is clearly not yet possible in valve surgery. In valve surgery, the definition of less invasive relates only to the size of incision and rate of recovery.
The aim of this article is to describe the technique, examine the progress in this field, comment on the potential of this approach, and put into perspective the expected goals of minimally invasive valve surgery and discuss the reasons why minimally invasive valve surgery is emerging as a standard of care worldwide. Furthermore, this article examines the evolution of recent experience with minimally invasive valve surgery and emphasizes the surgical considerations about the choice of incision, access technique for cardiopulmonary bypass (CBS), method of myocardial protection, technique for aortic occlusion, incisions for exposure of the diseased valves, and the use of CO2 hood to reduce the potential for air emboli.
Regarding the selection of suitable patients, it was shown that the new technique suits patients of average weight and height, and with non-calcific or mildly calcified valves. Patients with severely calcified valve lesions, concomitant coronary artery disease, calcifying pericarditis, morbid obesity, gross thoracic boney deformity, aneurysms of ascending aorta, poor ejection fraction, aortic stenosis that necessitated annular enlargement, and or mitral valve disease requiring chordal reconstruction for anterior mitral leaflet were excluded.
Of the two approaches mentioned above, upper ministernotomy approach provides access for the surgeon to perform a procedure from the mid-ascending aorta to the mid-left ventricular cavity. Additional procedures in this area through limited incisions may be possible (1).
The right anterolateral minithoracotomy for minimally invasive mitral valve surgery seems adequate, because this incision provides a direct line view of the left atriotomy with minimal patient discomfort thereafter. As demonstrated by Yugal (2), two-thirds of their patients who came for mitral valve surgery were young women; hence this incision gives better cosmetic results than any other incision because it remains hidden underneath the breast. Their strategy of switching to the transthoracic aortic clamp in place of the endoaortic clamp seems logical, because the transthoracic aortic clamp method appears safe and requires few additional resources or disposable supplies.
As demonstrated in this study and by others transthoracic-clamp occlusion was not difficult and antegrade cardioplegia provided excellent cardiac protection (2-4). Regarding difficulties facing the surgeon during performing such procedures, it is of course related to reduced exposure, which poses difficulties in intraoperative testing of valve prosthesis or assessment of valve repair. Transesophageal echocardiography (TEE) helps in overcoming such problems. It also helps in monitoring the process of de-airing of cardiac chambers, which is not easily accessible as in the classical approach. Otherwise we do not face major difficulties in performing such procedures. Partial upper re-sternotomy approach for AVR and Redo AVR after previous cardiac surgery seems to be a safe and effective alternative to full re-sternotomy and is associated with low morbidity and mortality (3).
In our study, re-operation was done in one case for postoperative prosthetic aortic valve endocarditis at two months through the same previous upper ministernotomy incision and found to be feasible and not difficult because the pericardium below the sternum remains intact with minimal adhesions, protecting the heart during re-entry.
In cardiac operations overall pain levels are relatively low. After minimally invasive procedures earlier mobilization is possible because of a better stability of the bony thorax, resulting in lower pain levels. It accelerates recovery and decreases pain, while maintaining overall surgical efficacy. The decreased pain reported by patients, may, in fact be related to the absence of retraction and stress placed on the ribs with the classical complete midsternotmy incision. A small wound reduces the potential for wound infection and blood loss from the incision (1,5).
Duration of ICU and hospital stay is gaining more and more importance, because they are the most important determinants of costs in cardiac surgery. Therefore, all steps that accelerate a patient's recovery and shorten hospital stay and thus reduce overall costs are appreciated. We confirm the results of Cosgrove (1), who reported a reduction of direct hospital costs of about 19% due to earlier extubation and reduced length of stay in the ICU. In our study, patients have been extubated earlier and discharged from the hospital early; mean hospital stay was 4.5 (range 4-5) days. Meanwhile follow up suggests these simplified approaches reduce patient pain and morbidity without jeopardizing surgical results.
Heinrich E. Machler et al (4) from Austria made a nice and well informative prospective study comparing the results of minimally invasive with conventional aortic valve operations in 120 patients .In there study, four surgeons were randomly assigned to perform the minimally invasive (L-shaped ministernotomy) (group 1) or the conventional (group 2) operation in 120 patients exclusively. In both groups (n = 60) there was no significant difference in the cross-clamping period (group 1, 60 minutes; range, 35 to 116 minutes), in the duration of extracorporeal circulation (group 1, 84 minutes; range, 51 to 179 minutes) or in the time from skin-to-skin (group 1, 195 minutes; range, 145 to 466 minutes). A patient in group 1 was extubated earlier, the postoperative blood loss was less, and the need for analgesics was reduced. In 5 patients in group 1 a redo operation was required for bleeding, 3 patients in group 1 required a redo operation because of paravalvular leakage or endocarditis, the overall 30-day mortality rate in there study was 1.6 %. Overall the survival rate was 95% in group 1 and 97% in group 2 .As mentioned in other studies in the literature they concluded that the advantages of minimally invasive aortic valve operation include reduced trauma from incision and duration of ventilation, decreased blood loss and postoperative pain, the avoidance of groin cannulation, and a cosmetically attractive result. Simple equipment was used with a high degree of effectiveness and with no sacrifice of safety. Their study demonstrated the practicability and reliability of this new method.
In our study analysis of surgery times for the next 25 patients, who underwent minimally invasive AVR in our department, confirmed this supposition: duration of surgery and ECC as well as aortic-cross-clamp-time decreased significantly and is now similar to conventional procedures. Others also made this experience (4), when new operative techniques were introduced they demonstrated that time for surgery may approximate to usual values for conventional AVR with increasing experience.
However, others reported longer ischemic- and CPB-times for minimally invasive aortic valve replacement (6). As mentioned earlier lesser wound complications and blood loss are decreased in minimally invasive access surgery. Our patient cohort is too small to investigate differences in frequency of wound infections or disturbances in wound healing between these minimally invasive approaches and the classical midsternotmy approach. Therefore, studies with greater patient cohorts are necessary to answer this question. With respect to blood loss, our study and the investigation done by others (4,7) demonstrate significant differences between both groups. As reported, blood loss after minimally invasive valve surgery is markedly reduced in comparison to conventional methods. Reasons may be due to: Avoidance of complete sternotomy; avoidance of mediastinal dissection (which leads to diffuse bleedings); and the smaller operative access. A critical consideration is that the main trauma, namely extra corporal circulation, has not been reduced (5).
Conclusion
Minimally invasive valve surgery is technically feasible, safe and provides adequate exposure for valve repair and/or replacement in selected cases. It allows speedy recovery and early hospital discharge as well as reduces complications. It remains a challenge for both the cardiac anesthetist and surgeon. Case selection and more technical experience are needed to further delineate the early and long-term outcome of this procedure.
References
1.
Cosgrove DM, Sabik JF. Minimally invasive approach for aortic valve operations. Ann Thorac Surg 1996; 62: 596-597.
2.
Mishra YK, Malhotra R, Mehta Y, et al. Minimally invasive mitral valve surgery through right anterolateral minithoracotomy. Ann Thorac Surg 1999; 68:1520-1524.
3.
Byrne JG, Karavas AN, Adams DH, et al. Partial upper re-sternotomy for aortic valve replacement or re-replacement after previous cardiac surgery. Eur J Cardiothorac Surg 2000; 18: 282-286.
4.
Machler HE, Bergmann P, Anelli-Monti M, et al. Minimally invasive versus conventional aortic valve operations: A prospective study in 120 patients. Ann Thorac Surg 1999; 67:1001-1005.
5.
Walther T, Falk V, Metz S, et al. Pain and quality life after minimally invasive versus conventional cardiac surgery. Ann Thorac Surg 1999; 67(6): 1643-1647.
6.
Ehrlich W, Skwara W, Klِovekorn W, et al. Do patients want minimally invasive aortic valve replacement? Eur J Cardiothorac Surg 2000; 17: 714-717.
7.
Christiansen S, Stypmann J, Tjan TDT, et al. Minimally invasive versus conventional aortic valve replacement - perioperative course and mid - term results. Eur J Cardiothorac Surg 1999; 16: 647-