Objective: To evaluate the long-term outcome after endonasal, endoscopic resection of juvenile nasopharyngeal angiofibromas.
Study design: Retrospective study of a series of ten consecutive patients undergoing endoscopic tumor resection at a University Hospital Center. All patients were male caucasians between 13 and 24 years of age.
Methods: Ten nasopharyngeal angiofibromas type II – IIIa according to Fisch, were diagnosed via computerized tomography scan or magnetic resonance imaging. All juvenile nasopharyngeal angiofibromas were resected via a combined endonasal peroral endoscopic approach. In three cases of type IIIa tumors a computer assisted intraoperative guiding system was applied (ENTrak, GE Medical, Lawrence, USA). Follow up checks included routine nasal endoscopy and regular magnetic resonance imaging.
Results: Ten consecutive patients underwent endonasal endoscopic juvenile nasopharyngeal angiofibromas resection. In two patients (20 %) an unmistakable recurrence with the need for further treatment was detected at 14 and 23 months after surgery respectively. One of the two recurrent tumors was successfully resected endoscopically. The second recurrence with infiltration of the skull base was treated with gamma knife. Eight patients (80%) were free of symptoms and showed a tumor free operation cavity with nasal endoscopy. In two of these patients and the patient, who underwent revision surgery postoperative magnetic resonance imaging showed localized enhanced signal, supposedly minimal residual tumor tissue. Magnetic resonance imaging follows up showed no growth and all three patients were free of symptoms over three, five, or nine years respectively and no further treatment was required.
Extension to the medial aspect of infratemporal fossa and retromaxillary space was not a contraindication against an endonasal endoscopic approach. Feeders from the internal carotid artery could effectively be dealt with endoscopically. The mean follow up was 39.1 months (range 5 months to 9 years) and the mean postoperative hospitalization was 6.2 days, with minimal postoperative morbidity. There was no surgical complications observed. The overall success rate in this case series was 90%, including one patient undergoing a second endoscopic resection and three symptom free patients with non growing minimal residual tumor tissue.
Conclusion: Resection of nasopharyngeal angiofibromas type II-IIIa can be safely achieved endoscopically. The advantage of this minimally invasive technique is the avoidance of external scars, shorter hospitalization, and low morbidity. The intraoperative computer assisted guiding system ENTrak was highly accurate and provided substantial help.
Key words: Juvenile nasopharyngeal angiofibroma, endoscopic sinus surgery, Computer assisted surgery
JRMS Dec 2005; 12(2): 18-24
Introduction
Juvenile nasopharyngeal angiofibromas (JNA) are highly vascular tumors of the nasopharynx originating from the area of the sphenopalatine foramen (1).
The morphology is characterized by architecturally irregular vessels ranging from capillary and sinusoidal-type vessels to muscular vessels set in a fibrous stroma (2,3). Beham et al (2) describe JNA as a tumor like vascular malformation. Schick et al (4) explain the vascular component of JNA embryologically due to incomplete regression of the first branchial artery. This vessel arises between embryological days 22 and 24 and recedes completely during normal development. It temporarily connects the internal carotid artery and the vessels from the maxillary artery.
Incomplete regression of the vascular plexus of this first branchial artery may form the vascular component of an angiofibroma arising due to growth stimulation at the time of adolescence. This rare entity occurs typically in male adolescents and is characterized by slow but locally destructive growth. Therapy is often challenging due to tumor spreading into critical areas such as pterygopalatine and infratemporal fossa, skull base, orbit or even intracranially. Cranial nerves, carotid arteries, cavernous sinus, and dura can be infiltrated. Although spontaneous regression of the tumor has been reported (5,6). Surgical resection is considered as therapy of choice. Surgical procedures include transpalatal techniques, lateral rhinotomy, midfacial degloving, infratemporal approaches, and combined infratemporal and frontotempral techniques (7-12).
The first reports about minimal invasive endoscopic resections were published during recent years (13-20). In our department, we started endoscopic resection of JNA as early as 1994. Since then experience with this minimally, invasive surgical technique has been gained over a period of nine years. This study presents a case series of 10 consecutive patients, who underwent endonasal endoscopic resection of JNA. A computer assisted intraoperative guiding system was applied in selected cases.
Methods
We present a retrospective study of the charts of ten patients undergoing endoscopic surgery for JNA between 1994 and 2002. Setting was the Department of ORL, University Medical School of Graz, Austria. All patients were males, between 13 and 24 years of age. According to Andrews/Fisch (21) the tumors of this series were classified from II to IIIa (Table I).
All patients underwent angiography and embolization of the tumor feeding vessels 1 to 20 days preoperatively. Two tumors with feeding branches from the internal carotid artery could not be fully embolized.
In all patients a combined endonasal and transoral endoscopic tumor resection was performed by the same experienced surgeon. For three resections of type IIIa angiofibromas an intraoperative computer assisted guiding system was applied (ENTrak, GE Medical, Lawrence, USA). Postoperative follow up including nasal endoscopy and magnetic resonance Imaging (MRI) ranged from 5 months to nine years, mean follow up was39.1 months (Table I)
Endoscopic surgical technique (according to Stammberger):
All patients were operated using the same endoscopic principles with modifications adapted to the individual case. A combined transnasal and transoral endoscopic approach was used:
Patients were positioned on their back, intubated transorally and the upper body and head elevated 10 degrees. A tongue depressor (standard tonsil spatulum) was inserted and a velotractor was applied transnasally and the soft palate thus elevated. This allowed for alternating or even simultaneous transnasal and transoral endoscopic approaches. For maximum vasoconstriction, pledgets (Sugomed®, Kettenbach, Germany) soaked in Adrenalin 1:1.000 and well squeezed out, were applied to the mucosa of the nose and the epipharynx. In special cases an intraoperative guiding system (ENTrak, GE Medical, Laurence, USA) was used. The headgear with electromagnetic feducials was placed on the external auditory canals.
One straight and one-bent suction devices were calibrated at the beginning of the procedure. The tip of these suction devices was visualized on frontal, sagittal and axial computerized tomography (CT) scans throughout the procedure (Fig. 1). After 10 minutes, the surgical procedure would start. 0o, 30o, 45o and 70o 4 mm telescopes (Karl Storz® Endoscopes, Tuttlingen, Germany) were used together with standard FESS-instrumentation. Bipolar suction-cautery forceps proved essential for the technique, the straight one being used transorally and the curved one transanally.
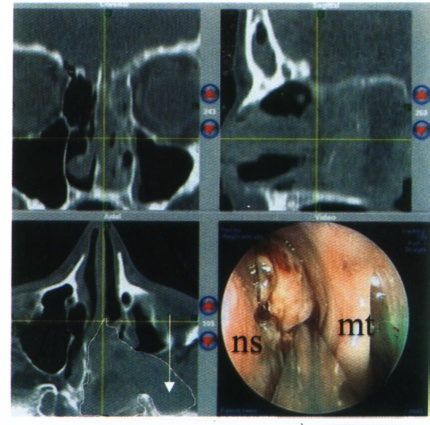 Fig. 1:
Fig. 1: Intraoperative Computer assisted navigation CT of IIIa nasopharyngeal angiofibroma. In the axial CT scan the white line shows the tumor extension with infiltration in the left infratemporal fossa (white arrow). The grey cross indicates the tip of the suction device while using computer assisted navigation. (Patient number 7). nS = nasal septum, mT = middle turbinate.
The first step in most cases was aimed at the sphenopalatine foramen and/or the sphenopalatine artery respectively, usually the area and source of origin of the lesion. To achieve this, depending on the extend of the angiofibroma in the individual case, anterior and posterior ethmoid sinuses were opened and depending on the degree of infiltration, the middle and/or inferior turbinates partially resected. In the vicinity of the sphenopalatine foramen a subperiostal plane was identified and if possible, the stem of the artery identified and resected as far laterally as possible (Fig. 2).
In cases of considerable lateral extension of the lesions, the internal maxillary artery was exposed and clipped in four patients (one Fisch type II and three Fisch type IIIa lesions).
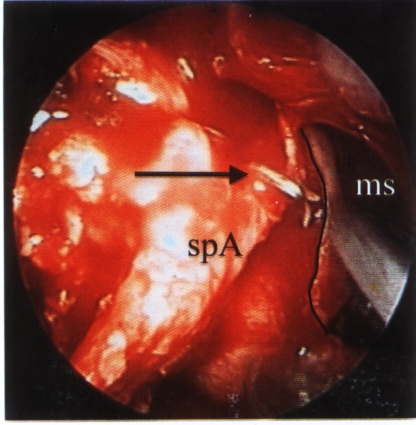 Fig. 2:
Fig. 2: The left sphenopalatine artery was clipped (black arrow) on the edge to the pterygopalatine fossa. The black line indicates the posterior wall of the left maxillary sinus. spA = sphenopalatine artery, mS = maxillary sinus.
When infiltration of posterior segments of the septum were present, the latter was transacted anterior to the infiltration and the lesion from there depressed down into the nasopharynx, as even with piece-meal resection technique, portions of the angiofibroma would usually be too large to allow for transnasal removal.
In cases of sphenoid sinus involvement, a cleavage plane was identified between the tumour and the sinus walls and feeders from the internal carotid artery thus identified, cauterised and transacted. In all cases optic nerve and carotid artery could easily be identified and damage avoided despite bony walls being frequently deficient (Fig. 3,4).
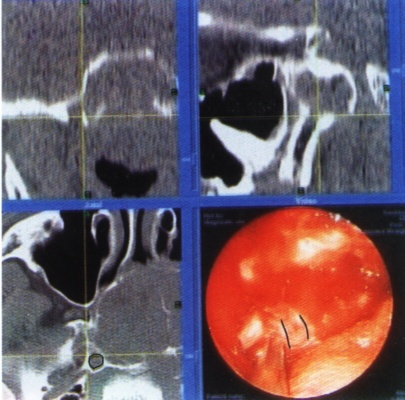 Fig. 3:
Fig. 3:The tip of the suction device is positioned towards the right infratemporal fossa. The black line indicates the right internal carotid artery. (Patient number 10).
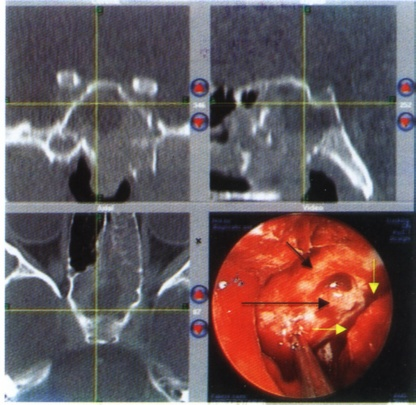 Fig. 4:
Fig. 4:The tumor was resected from the sphenoidal sinus and is pulled downwards into the nasopharynx (white arrows). The bulges of optic nerve (short black arrow) and internal carotid artery (long black arrow) are clearly visible. (Patient number 10).
When the tumour had infiltrated and/or penetrated the floor of the sphenoid sinus, the angiofibroma components were followed from superiorly to inferiorly and “pushed” to the nasopharynx. We have not encountered a true infiltration of the cavernous sinus in our series, but frequently saw compression of the sinus by the angiofibroma.
Extensions to the infratemporal fossa were dealt with after partial or subtotal resection (including drilling) of the pterygoid, usually the medial plate but in two cases as the lateral plate as well. For retromaxillary extension, the posterior wall of the maxillary sinus was removed and the lesions thus exposed. External pressure with a finger behind the tuber maxillae in those cases helped to displace the lesions medially and thus make it accessible for endoscopic techniques (Fig. 5). In all cases with retromaxillary lateral extension, the internal maxillary artery was identified and clipped as safety precaution.
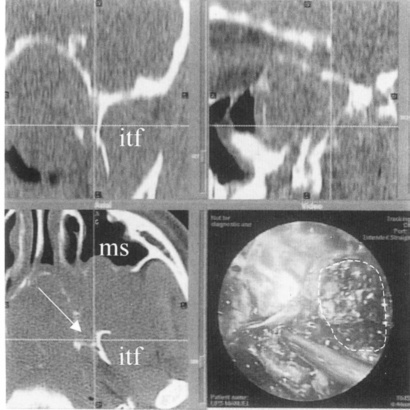 Fig. 5.
Fig. 5. The white line shows the area where tumor was resected from the medial aspect of the left infratemporal fossa. The grey cross indicates the tip of the suction device placed to the bony wall of the internal carotid artery. (Patient number 7). itF = infratemporal fossa, mS = maxillary sinus
The simultaneous inspection through the mouth with 30°, 45° or 70° lens telescopes allowed for control of the surgical field, removal of the dissected angiofibroma components and good access for hemostasis.
Though technically, the endoscopic approach to the infratemporal fossa and to the clivus was sometimes challenging, it was the nasopharynx extension that proved most time consuming to remove in those cases where there was a diffuse infiltration of this region by the JNA. A clean cleavage plane sometimes was difficult to achieve here, as visual distinction between lesion and the soft prevertebral tissue was very difficult. In some situations therefore, the deep fascia had to be identified for a safe cleavage plane.
Hemostasis was achieved with bipolar suction cautery and the surgical cavity covered with Resorbable Oxicell pieces at the end of the procedure. It may be indicative of a learning curve, that in the last four cases, including three IIIa angiofibromas, no packing was used at all. So far only one of the ten patients (the first one) required revision surgery. There were no complications associated with any of the procedures; especially no bleeding that required the operation to be abandoned.
Endovascular embolization:Angiography and embolization were preceded by tumour evaluation by means of CT and/or MRI scans. In all patients angiography and embolization were performed during the same session. In all cases, a coaxial catheter system (Seldinger) was introduced via a transfemoral approach. A superselective catheterization of the supplying external carotid artery and internal carotid artery branches was performed in order to devascularize the tumor. For embolization, either polyvinyl alcohol particles in solution of non-heparinized saline or isobutyl-cyanoacrylate mixed with non-ionic contrast medium were used. Time interval was between 1 and 3 days with one exception of 20 days prior to surgery.
One patient (case 3) suffered from temporary motor aphasia after embolization due to connecting branches to the internal carotid artery. An MRI scan showed signs of ischemia of the region of the medial meningeal artery. Neurological signs vanished after 72 hours but surgery was postponed. Eight months later a second embolization was performed. Again the patient suffered from short time slowing of speech, but no ischemia of cerebral structures was detected on MRI. Endoscopic tumor resection without complication was performed 20 days later.
In one patient (case 4) with a recurrence invading the skull base (patient 4) embolization of the maxillary artery was followed by temporary partial motor aphasia. An MRI scan showed ischemia of the thalami area. No further surgical resection was attempted and the patient underwent gamma knife treatment.
Results
Two of 10 patients (20%) had recurrences requiring further treatment. One of these could be managed successfully with a second endoscopic resection 23 months after first surgery. The other due to embolisation complications was not operated upon, but underwent gamma knife therapy. Eight patients (80%) at follow up were free of symptoms and showed a normal postoperative cavity with nasal endoscopy. Two of these patients and the patient, who underwent revision surgery demonstrated minor signal enhancement on postoperative MRI, which we classified as supposedly minimal residual disease (Table 1). MRI follow up showed no growth and patients were free of symptoms without further treatment at 108, 61 and 38 months postoperatively.
The overall cure rate including one patient undergoing a second endoscopic resection and three patients with non growing minimal residual tumor tissue was 90%. The mean follow up was 39.1 months (range 5 months to 9 years). In eleven endoscopic tumor resections with prior embolization the blood loss ranged from 100ml to 1500ml mean blood loss was 500 ml. Three patients with blood losses of 1000-1500 ml received peroperative hemodilution. No patient was given units of donor blood. In four cases posterior packing was necessary for 24 hours postoperatively. Since 1998 no posterior packing was applied in four consecutive cases including three IIIa JNAs.
The mean surgical time for ten approaches (for case 1 data was not available) was three hours and 38 minutes (range from 1 hour thirty minutes to 6 hours). For the last three consecutive cases, including two IIIa JNAs the mean operating time was 2 hours and fifteen minutes, indicating a “learning curve”. In two of these cases a computer assisted guiding system was used. The short operating time using this system suggests that this technique helps to save time in the operating theater despite the increased technical effort.
Discussion
Transfacial approaches like midfacial degloving or lateral antrotomy are standard techniques for resection of juvenile angiofibromas with tumor extension to the nasopharynx, pterygopalatine fossa, sphenoid, and skull base. The infratemporal fossa approach enables optimal exposure of tumors with more lateral extension behind the pterygoid plates. Fisch (10) recommends his type C infratemporal approach for type III and IV juvenile angiofibromas. These techniques enable optimal tumor exposure, but the side effects cannot be excluded in any case. Hypoesthesia of V2 and V3, serous otitis media and transient trismus were described after infratemporal approaches (11,22). Herman (23) reviewed 44 cases operated via lateral rhinotomy, midfacial degloving or Lefort I osteotomy and found late complications such as infraorbital nerve dysesthesia (5 cases), lacrimal duct stenosis (4 cases) and secretory otitis media (2 cases). Herman (23) states that a transfacial approach helps to avoid neuralgia of the V nerve or trismus related to sectioning the pterygoid muscles during an infratemporal approach. External scars and interference with facial bone still in growth should be avoided if possible.
The evolution of endoscopes, special instruments, and experience in sinus surgery enables minimal invasive endonasal resection of tumors in the skull base area today (24). First reports about successful endoscopic resections of JNAs have been published since 1998 (13-20). The only complication reported in the literature was one case of optic nerve neuropathy, which was successfully managed with endoscopic decompression (16). Draf et al (25) successfully resected JNAs type I-II with an endonasal microendoscopic approach.
Endonasal endoscopic resections of JNA have been performed in our department since 1994. Therefore we are now able to present long-term results of a case series of ten consecutive patients for nine years. Patients were operated by the same experienced surgeon and followed up endoscopically and via MRI. The present series includes four type IIIa tumors with involvement of the infratemporal fossa. In all cases exclusively endoscopic tumor removal via a combined endonasal and enoral approach was possible. Extension to the medial aspect of the infratemporal fossa and retromaxillary space was not a contraindication for an endoscopic approach. Feeders from the internal carotid artery could well be dealt with endoscopically. No perioper- or postoperative complication was observed.
In three cases a computer assisted guiding system (ENTrak, GE Medical, Lawrence, USA) was applied, providing better orientation in critical areas, such as pterygopalatine fossa, infratemporal fossa or close to the internal carotid arteries (Fig. 3-5). The technical system helps to orientate, but will never replace the surgeon’s exceptional knowledge of this complicated anatomical area.
By far the most feared complication in JNAs is intraoperative bleeding. To prevent excessive intraoperative blood loss, embolization of tumour feeding vessels was advocated by Robertson et al in 1972. All authors cited recommend embolization before endonasal endoscopic tumour resection. Nevertheless embolization bears a risk if tumour-feeding trunks originate from the internal carotid artery. Two patients of the presented study suffered from intracerebral ischemia after embolization, but without sequales were observed. In our opinion preoperative embolization of the tumour is advisable because blood loss is reduced and long time complications are remote.
Long term studies on recurrence rates include tumors of different extensions and resection techniques and are therefore difficult to compare: Paris (8) reports a recurrence rate of 21% (43 cases, different non- endoscopic approaches), McCombe (9) of 34% (33 cases, lateral rhinotomy), Lloyd (1) of 39.5% (72 cases, non- endoscopic techniques) and Fagan (7) of 37% (16 cases of advanced tumor stage, 3 endonasal endoscopic approaches, 13 non-endoscopic approaches). The risk for recurrence is higher if tumor involvement of the base of pterygoids, deep invasion of the sphenoid, cavernous sinus or infratemporal fossa is present (1,12,23). Herman (23) states that the use of endoscopes in combination with a transfacial approach resulted in a decrease of recurrences in his study.
When discussing recurrences one has to differentiate true new tumor growth from asymptomatic, non growing residual tumor tissue (26). Minimal tumor remnants detected on MRI in asymptomatic patients may undergo involution later on (7,9,23,26). Therefore, extensive surgery to completely remove minimal residual tumor tissue is not mandatory. Close follow up including nasal endoscopy and regular MRI or CT scans is an alternative to early revision surgery. In case of tumor, regrowth further treatment is indicated.
Type IV JNA however, pose a clear limitation to exclusively endoscopic approaches, as do some forms of orbital fissure involvement. The low morbidity, short hospitalization and minimal invasive character of the endoscopic approach have clear advantages. It is a safe procedure in the hands of an experienced endoscopic surgeon, especially when an intraoperative guiding system is used.
Conclusion
Endoscopic resection of nasopharyngeal angiofibroma up to stage IIIa according to Fisch can be recommended for surgeons experienced in endoscopic sinus surgery. Advantages of the endoscopic technique are the minimal invasive character and low morbidity.
Table I: Different characteristics, follow-up and outcome for the study group.
|
No
|
Age
|
Fisch type
|
Tumor involvement
|
Approach
|
Duration
|
Blood loss
|
Packing
|
Follow-up months
|
MRI (postop)
|
Outcome
|
|
1
|
13
|
II
|
NPH*, ppH
|
ESS
|
No data
|
100 ml
|
None
|
23
|
Recurrence
|
Recurrence
|
|
|
|
|
NPH
|
ESS (revision 23 moths after first ESS)
|
3 hr
|
450 ml
|
24 hr
|
108
|
Regredient tissue
|
FOS
|
|
2
|
24
|
II
|
NPH, bil, ppF, max+ethm.sin
|
ESS
|
2 hr 43 min
|
100 ml
|
None
|
22
|
NAD
|
FOD
|
|
3
|
22
|
II
|
NPH, ppF, max. sin, cheek
|
ESS, clipping of max.art
|
4 hr 30 min
|
1500 ml
|
24 hr
|
84
|
Not available
|
FOD
|
|
4
|
14
|
III a
|
NPH, ppF, max+ethm+sphen sin ,sphenoid
|
ESS, clipping of max, art
|
6 hr
|
300 ml
|
24 hr
|
14
|
Recurrence invading skull base
|
Recurrence (gamma knife therapy)
|
|
5
|
13
|
II
|
NPH, ethm+sphen sin floor of sphenoid
|
ESS
|
4 hr
|
400 ml
|
None
|
61
|
Residual tissue
|
FOS
|
|
6
|
15
|
III a
|
NPH, ppF, itF
|
ESS
|
3 hr 30 min
|
1000 ml
|
24 hr
|
31
|
NAD
|
FOD
|
|
7
|
15
|
III a
|
NPH, ppF, sphenoid, itF, orbit
|
ESS+intraop guiding system
|
5 hr 30 min
|
1000 ml
|
None
|
38
|
Residual tissue
|
FOS
|
|
8
|
11
|
III a
|
NPH, ppF, itF
|
ESS+intraop guiding system, clipping of max. art
|
2 hr 16 min
|
250 ml
|
None
|
16
|
NAD
|
FOD
|
|
9
|
15
|
II
|
NPH, ppF, sphenoid clivus
|
ESS
|
1 hr 30 min
|
30 ml
|
None
|
12
|
Not available
|
FOD
|
|
10
|
15
|
III a
|
NPH, ppF, sphen sin, itF, orbit
|
ESS + intraop guiding system, clipping of max. art
|
3 hr
|
400 ml
|
None
|
5
|
NAD
|
FOD
|
NPH: Nasopharynx ppF: pterygopalatine fossa itF: infratemporal fossa ESS: endosopic sinus surgery NAD: no abnormality dedected
FOS: free of symptoms FOD: free of disease
Table II:Classification of Nasopharyngeal Angiofibromas according to Andrews / Fisch (21)
|
Type I
|
Tumor limited to the nasopharynx and nasal
cavity. Bone destruction negligible or
limited to the sphenopalatine foramen
|
|
Type II
|
Tumor invading the pterygopalatine fossa or the
maxillary, ethmoid, or sphenoid or sinus with bone destruction
|
|
Type III a
|
Tumor involving the infratemporal fossa or orbital
region without intracranial involvement.
|
|
Type III b
|
Tumor invading the infratemporal fossa or orbit with
intracranial extradural (parasellar) involvement
|
|
Type IV
|
Intracranial intradural tumor with infiltration of
the cavernous sinus, pituitary fossa or optic chiasm
|
References
1.
Lloyd G, Howard D, Phleps P, Chessman A. Juvenile angiofibroma: The lessons of 20 years of modern imaging. J Laryngol Otol 1999; 113(2): 127-134.
2.
Beham A, Beham-Schmid C, Regauer S, et al. Nasopharyngeal angiofibroma: True Neoplasm or vascular malformation? Adv Anat Pathol 2000; 7: 36-46.
3.
Beham A, Regauer S, Beham-Schmid C, et al. Expression of CD34-antigen in nasopharyngeal angiofibroma. Int J Pediatr Otorhinolaryngol 1998; 44: 245-250.
4.
Schick B, Plinkert P, Prescher A. Etiology of angiofibromas: Reflection on their specific vascular component. Laryngo-Rhino 2002; 81: 280-284.
5.
Stansbie JM, Phelps PD. Involution of residual juvenile nasopharyngeal angiofibroma. J Laryngol Otol 1986; 100: 599-603.
6.
Weprin LS, Siemens PT. Spontaneous regression of juvenile nasopharyngeal angiofibroma. Archive of Otolryngology Head and Neck Surgery 1991; 117: 796-799.
7.
Fagan JJ, Snyderman CH, Carrau RL, Janecka IP. Nasopharyngeal angiofibromas: Selecting a surgical approach. Head Neck 1997; 19: 391-399.
8.
Paris J, Guelfucci B, Moulin G, et al. Diagnosis and treatment of juvenile nasopharyngeal angiofibroma. Eur Arch Otorhinolaryngol 2001; 258(3): 120-124.
9.
McCombe A, Lund V, Howard D. Recurrence in juvenile angiofibroma. Rhinology 1990; 28: 97-102.
10.
Fisch U, Mattox D. Microsurgery of the skull base. Stuttgart: Thieme 1988; 350-389.
11.
Close LG, Schaefer ST, Mickey B, Manning S. Surgical management of nasopharyngeal angiofibroma involving the cavernous sinus. Arch Otolaryngol Head Neck Surg 1989; 115: 1091-1096.
12.
Howard DJ, Lloyd G, Lund V. Recurrence and its avoidance in juvenile angiofibroma. Laryngoscope 2001; 111(9): 1509-1511.
13.
Bernal-Sprekelsen M, Vazquez A, Pueyo J, Casasus C. Die endoskopische Resektion juveniler Nasenrachenfibrome. HNO 1998; 46: 172-174.
14.
Jorissen M, Eloy P, Rombaux P, et al. Endoscopic sinus surgery for juvenile nasopharyngeal angiofibroma. Acta Otolaryngol Bel 2000; 54(2): 201-219.
15.
Newlands SD, Weymuller EA Jr. Endoscopic treatment of juvenile nasopharyngeal angiofibroma. Am J Rhinol 1999;13(3): 213-219.
16.
Carrau RL, Snyderman CH, Kassam AB, Jungreis CA. Endoscopic and endoscopic-assisted surgery for juvenile angiofibroma. Laryngoscope 2001; 111: 483-487.
17.
Scholtz AW, Appenroth E, Kammen-Jolly K, et al. Juvenile nasopharyngeal angiofibroma: Management and therapy. Laryngoscope 2001;111: 681-687.
18.
Roger G, huy T, Froehlich P, et al. Exclusively endoscopic removal of juvenile nasopharyngeal angiofibroma: trends and limits. Arch Otolaryngol Head Neck Surg 2002; 128: 928-935.
19.
Mair EA, Battiata A, Casler JD. Endoscopic laser-assisted excision of juvenile nasopharyngeal angiofibromas. Arch Otolaryngol Head Neck Surg 2003; 129: 454-459.
20.
Anderhuber W, Stammberger H, Walch CH, et al. Rigid endoscopy in minimally invasive therapy of tumors of the paranasal sinuses and skull base. Min Invas Ther & Allied Technol 1999; 8: 25-32.
21.
Andrews JC, Fisch U, Valavanis A, et al. The surgical management of extensive nasopharyngeal angiofibromas with the infratemporal fossa approach. Laryngoscope 1989; 99: 429-437.
22.
Brown JD, Jacob SL. Temporal approach for resection of juvenile nasopharyngeal angiofibromas. Laryngoscope 2000; 110(8): 1287-1293.
23.
Hermann P, Lot G, Chapot R, et al. Long-term follow-up of juvenile nasopharyngeal angiofibromas: analysis of recurrences. Laryngoscope 1999; 109(1): 140-147.
24.
Walch CH, Stammberger H, Anderhuber W, et al. The minimally invasive approach to olfactory neuroblastoma: combined endoscopic and stereotactic treatment. Laryngoscope 2000;110: 635-640.
25.
Schick B, Tahan A, Brors D, et al. Experiences with endonasal surgery in angiofibroma. Rhinology 1999; 37: 80-85.
26.
Jones GC, DeSanto LW, Bremer JW, Neel HB. Juvenile angiofibromas. Behavior and treatment of extensive and residual tumors. Arch Otolaryngol Head Neck Surg 1986; 1191-1193.