Objective: To compare the response of four groups of vocal fold paralysis with different etiologies to percutaneous electrical stimulation and at reanalyzing the outcome according to duration of the condition.
Methods: Medical files of 60 patients referred to the Speech Clinic, Royal Rehabilitation Center during the last eight years, complaining of weak breathy voice due to vocal fold paralysis, were reviewed and classified according to etiology, gender, and duration of onset. Patients received daily sessions of electrical stimulation, applied percutaneously, for 2-7 weeks. The initial and follow-up phonation times and perceptual acoustic analyses were tabulated for each patient. A separate 10-point rating scale on the clarity and loudness of the patient’s voice was given by the patient, the otorhinolaryngologist, and the speech pathologist, before and after the administration of electrical stimulation. The responses to therapy were statistically analyzed and compared according to etiology and duration of onset.
Results: A paired T-test for both the phonation time and the rating of voice quality, before and after electrical stimulation, showed significant differences (p< 0.001) in all four etiologies. Analysis of variance showed that there was no statistical difference according to etiology and, with certain limitation, according to duration of onset of the paralysis.
Conclusion: The outcome and time course of recovery of vocal fold paralysis by implementing electrical stimulation are similar in different etiologies of the paralysis regardless of the duration of the condition.
Key words: Vocal fold paralysis, Electrical stimulation, Loudness, Noise, Phonation time.
JRMS Dec 2005; 12(2): 25-32
Introduction
Vocal fold paralysis (VFP) is a probable complication following thyroidectomy, neck or chest surgery intended to remove a tumor, penetrating trauma, viral infections, or due to idiopathic etiologies, as well as due to central causes (1). Symptoms range from transient aphonia to breathiness and hoarseness of voice with occasional diplophonia, along with aspiration of liquids. Acoustic signs include a periodicity, limited pitch range, increased noise levels, and limited intensity range (2,3).
These symptoms may resolve gradually in 40% (4) to 50% (5) patients within six months following thyroidectomy. Surgical procedures to improve vocal fold valving include, among other techniques, nerve anastomosis (6), Teflon injection (7), fat injection (8), and medialization (9-11). These techniques remain an option if symptoms persist and if traditional voice therapy fails to satisfy the patient’s needs.
Percutaneous neuromuscular electrical stimulation (ES) was effectively used and became a common practice in the conservative management of VFP in Germany and Russia (4,12-22). Also, it was used following surgical management of the glottis in patients with bilateral adductor VFP (18,22) and in the management of functional aphonias and dysphonias (18), and hypokinetic dysphonias, including myasthenia’s (13,18-21). Comparative studies (20-23) showed that combined ES with voice therapy gave superior results when compared to traditional voice therapy.
Electrical stimulation aid in managing VFP as it promotes nervous recovery, counteracts muscular atrophy, and induces desirable hyperemia. It also stimulates adjacent healthy muscles, including the external strap muscles, and the bilaterally innervated interarytenoid and the cricothyroid muscles to an increased compensatory activity (12,13,16).
The responses of the vocal folds to direct or percutaneous ES can be evaluated via a balloon inserted in the larynx (24-28), by direct visual inspection of a gauge needle inserted through the epiglottis (29,30) or through the vocal fold. (30), by direct laryngoscopy (31) or stroboscopy (13,14,19), using spectrographic analysis (20), using magnifying mirror (13), or by videotaping (32). The technique of ES as a diagnostic and therapeutic tool in VFP was found to be safe (18, 29).
The aim of this study was to compare the course of recovery after vocal fold paralysis according to different etiologies and duration of the condition. Recovery was assessed by recording changes in phonation time and vocal quality ratings.
Methods
The medical records of a convenient sample of 60 patients (Appendices 1-4) with dysphonias following vocal fold paralysis and received electrical stimulation at the speech clinic in the Royal Rehabilitation Center during the period 1996 – 2004. Cases of VFP due to central etiologies were excluded from the total pool. The subjects were 33 males (age range 19-69 year; mean 41.4 ± 14.5 years) and 27 females (age range 16-66 years; mean 39.6 ± 13.8 years). The etiology of the unilateral vocal fold paralysis were 21 cases following partial or total thyroidectomy, 16 cases following neck or chest surgery*, 11 cases post viral infections, and 12 cases with idiopathic VFP. The affected side was the right vocal fold in 20 cases, the left vocal fold in 38 cases, and bilateral in two cases. The duration of the paralysis was one month or less in 14 (23.3%) patients, from five weeks to five months in 29 (48.3%) patients, from six to eleven months in 10 (16.7%) patients, and one year or more in 7 (11.7%) patients.
The treatment technique included percutaneous application of triangular faradic modulated current, with around 12 to 24 slow rising surges per minute (13) at 100Hz, with current intensity slightly above the sensation level by the individual patient range (2.6-6.0 milli Amperes (mA); mean (3.8 ± 0.8) and was then increased gradually from session to session according to the patient’s adaptation range (4.0-9.0 mA); mean=(5.7 ± 1.1 mA). Neuroton 726s {Siemens} muscle stimulating unit was used in all patients. Depending on the case, a total of 14-52 sessions were given, initially on daily basis and followed by differently spaced sessions according to the individual need but with a minimum of 3 sessions per week.
Inpatients and some outpatients received ES twice per day. In each session, three 50 trains of pulses applied, timed with prolonged phonations, alternating from the effected side to the intact side and back to the effected side. The maximum duration of each session was 15 minutes. ES was interrupted whenever the signs of discomfort appeared on the patient or when his voice became weaker. Relatively severe cases received a warming stage at the beginning of initial sessions by applying a 5 minute of ‘rectangular’ current aiming at increasing the blood flow due to its warming effect (13) and they were asked to tilt their heads downward a little during the ES sessions.
Before the application of ES, each patient received full explanation about the technique that included demonstration of the technique in front of the patient. Some patients and few normal subjects were hooked to a pulse meter and their pulse rates were recorded before and during ES. None of these showed remarkable increases in the pulse rate, and only one case showed negligible decrease.
Voice Therapy
When patients achieved reasonable improvement in vocal quality, they were instructed to do phonation exercises (15) at home, five sessions per day, around one to three minutes each according to the individual’s capacity. They were asked to keep daily records of their phonation time in seconds. Every patient was counseled to avoid vocal strain or abuse in order to prevent unnecessary muscular tension. Voice therapy was initiated at the appropriate time in order to increase the pitch and the respiratory support. This was timed with instructing the patients to raise the pitch of their voice during ES application, and then, to fluctuate their pitch up and down. Furthermore, the patients were instructed to prolong and inflect voiced words, such as ‘ema’ and ‘deema’, at rising and then falling intonation.
Measurement
Two types of measurements** were used to record improvement following ES, phonation time and rating scales. The latter is composed of a 10-point scale; with ′1′ refers to complete aphonia, and ′10′ refers to normal quality. Ratings were collected from the client or a family member, the referring otorhinolaryngologist (ENT), and the speech pathologist. As a result six ratings were gathered for each client, three before the application of ES and three after. For the sake of the present analysis, each of the accumulated three ratings given before and after ES were averaged into one rating and then this figure was approximated to the nearest ‘full digit’. The ratings given by the patients or their family members correlated relatively higher (0.81) with the ratings given by the speech pathologist than with those given by the ENT (0.77). The results of s/z ratio*** were not included in the present study due to the fact that most clients who suffer from vocal fold paralysis tend to devoice the /z/ sound after the first few seconds of phonation. The phonation time was the average of three consecutive prolongations of the vowel /i/ on deep breath, with enough period of rest in between.
The reliability of both the phonation time and the ratings done by the speech pathologist were measured by having another qualified speech pathologist measure the phonation time and rate the vocal quality of at least 25% of the cases. In order to find inter-rater reliability, the number of agreements between the researchers and the second speech pathologist was calculated. These figures were divided by the sum of both agreements and disagreements (35). The reliability measures for both the phonation time and the ratings of vocal quality were 0.93 and 0.90, respectively.
Results
As shown in Table I and Appendices 1-4, there was a remarkable increase in both phonation time and the average rating following voice therapy combined with percutaneous neuro-muscular electrical stimulation.
The mean of the initial phonation times for the total sample was (3.85 ± 2.81 seconds) range (0.0 – 13 seconds), while the final mean phonation times was (12.27 ± 5.76 seconds) range (3.0 – 32 seconds). The mean difference in the phonation time was significant at p≤ 0.001 for the total sample and for each of the four groups (Table II). The mean of the initial ratings for the total sample was (4.32 ± 1.32 second) range (2 – 7 seconds), while the mean of the final ratings was (8.23 ± 1.41 seconds) range (5 – 10 seconds). This difference in the rating was significant at p≤ 0.001 for the total sample and for each the four groups (Table II). Analysis of variance (Table III) shows that there was no statistical significant difference in the gains achieved between the four different etiologies of vocal fold paralysis.
Reanalyzing the data according the duration of onset (Table IV) shows that the gain in both parameters of the study was statistically significant for each duration of onset subgroup. Analysis of variance (Table V) shows that there was no statistical significant difference between the four different duration of onset of the vocal fold paralysis.
Multiple Tukey’s HSD Post Hoc comparisons showed that the only statistical significant difference was between the first ‘duration of onset’ subgroup (i.e. less than one month) and the forth ‘duration of onset’ subgroup (i.e. more than one year) in both the gain in the ‘duration of phonation’ (p=0.023) and the gain in the ‘averaged rating’ (p=0.012), where the first group benefited the most from electrical stimulation.
Figures 1- 4 below show graphic presentations for both the ‘phonation time’ and the ‘averaged rating’ for selected subjects from the four ‘etiology subgroups’. It is obvious from the graphs that the improvement in both parameters of the study is coincided with the initiation of ES and the slope of the spontaneous recovery, if in process, became steeper after the application of ES.
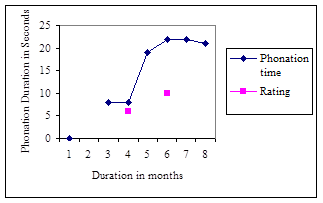
Fig. 1:A graphic presentation of the gain in phonation time by subject OZ. Therapy started on week 17 and extended over 5 weeks. Follow up was done on months 7 & 8.
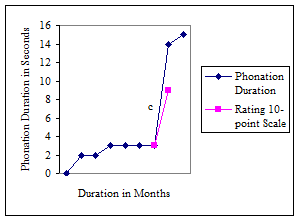
Fig. 2: A graphic presentation of the gain in phonation time by subject AG. Therapy started on week 30 and extended over 4 weeks. Follow up was done on month 9.
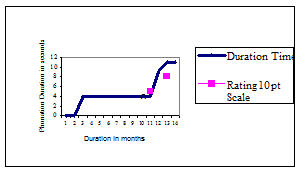
Fig. 3: A graphic presentation of the gain in phonation time by subject YY. Therapy started on week 47 and extended over 6 weeks. Follow up was done on months 13 & 14.
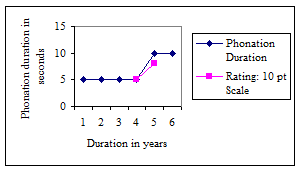
Fig. 4: A graphic presentation of the gain in phonation time by subject AZ. Therapy started on the end of year 4 and extended for 4 weeks. Follow up was made six months later.
Discussion
The results of the present study are in concordance with the published European studies (4,12-22), which implemented neuromuscular electrical stimulation, in conjunction with traditional voice therapy, for both unilateral and bilateral adductor vocal fold paralysis. However, this study is different in sample size and by including clients with various etiology and duration. The vast majority of the subjects benefited to varying degree from ES. One of the subjects, who recovered only partially over four years after hemithyroidectomy, improved remarkably with ES. Previous studies targeted on subjects immediately after the onset of the illness.
Additional notes can be driven. First, the gain in phonation time does not seem comparable to the increase
in the rating scales or vice versa for many patients, which can render for many explanations. Some patients, mainly younger subjects and those with heavy job speaking demands, are seeking full recovery of premorbid voice. They, and even the otolaryngologists, seem to be influenced by the presence of mild hoarseness of voice. Twelve of the subjects of the present study were experiencing premorbid voice abuse and/or excessive muscular tension as documented by their case histories. Endolaryngoscopies for two of them showed hypertrophied false folds. Second, the improvement in phonation time, loudness, and vocal clarity that exceeds endolaryngoscopic findings might be due to ES that enhanced compensatory behavior in addition to its influence on the effected VF.
Limitations of the present study are: 1. Choosing subjective rating and mean phonation time as outcome indicators, 2. Matching groups according to age and gender was not done, and 3. A control group was not included, to enable relevant comparisons.
Several conclusions are inherited in the present study. First, ES is an efficient technique to improve vocal loudness and quality following VFP. Second, the described technique helps to prevent the unnecessary muscle tension that develops when using some traditional approaches. Finally, this study clearly documents that certain laryngeal neuropathologies, such as vocal fold adduction and tension problems, can be dealt with using this technique regardless of the etiology and duration.
Voice therapists are urged to implement this procedure without waiting for the possible spontaneous recovery. It is also recommended to replicate this study with a larger sample and to compare with the outcomes and course of recovery of using traditional approaches.
Acknowledgments
We would like to acknowledge Gayle Woodson, MD, Shelley von Berg, PhD, and Linda Carroll, PhD, for their enthusiasm, support and reviewing the technique. Many thanks are due to Adrianne Perlmann, PhD, for her encouragement and support to conduct a pilot study on a canine and to proceed on with human subjects. Our deep appreciation for the present and former otolaryngologists of the ENT Department, King Hussein Medical Center, for their faithful confidence in referring cases and help in providing the rating of vocal behavior and repeated endolaryngoscopy reports.
Table I:Descriptive statistics for both pre-post phonation time and ratings for the total sample.
References
1. Terris DJ, Arnstein DP, Nguyen, HH. Contemporary evaluation of unilateral vocal cord paralysis [review]. Otolaryngology- Head and Neck Surgery 1992; 107: 84-90.
2. Colton RH, Casper, JK. Understanding voice disorders: A physiology perspective for diagnosis and treatment. 2nd ed. Baltimore, Williams & Wilkins 1996; 155, 259-258.
3. Aronson AE. Clinical voice disorders: An interdisciplinary approach. 3rd Ed. New York. Thieme Medical Publishers. 1990; 58-86.
4. Blomstedt B, Rydmark KE. Paralysis of the recurrent laryngeal nerve following thyroidectomy. Acta Otolaryngology 1960; 52: 150-156.
5. Casper JK, Colton RH, Brewer, DW. Selected therapy techniques and laryngeal physiological changes in patients with vocal fold immobility. In V. Lawrence editors. Transcripts of the 14th symposium: care of the professional voice. New York: Voice Foundation. 1986; 122-124.
6. Crumley RL. Phrenic nerve graft for bilateral vocal cord paralysis. Laryngoscope 1983; 93: 425-8.
7. Lewy RB. Teflon injection: Pointers and pitfalls. Annals of Otology, Rhinology, and Laryngology 1993; 102: 283-284.
8. Jiang JJ, Titze IR, Wexler DB, Gray SD. Fundamental frequency, and amplitude perturbation in reconstructed canine vocal folds. Annals of Otology, Rhinology, and Laryngology 1994; 103: 143-148.
9. Koufman JA. Laryngoplasty for vocal cord medialization: An alternative to Teflon. Laryngoscope 1986; 96: 726-731.
10. Isshiki N. Functional Surgery of the Larynx with Special Reference to Percutaneous Tension of the Vocal Cords. Kyoto: Media Press 1977; 300-310.
11. Sawashima M, Totsuka G, Kobayashi T, Hirose M. Reconstructive surgery for hoarseness due to unilateral vocal cord paralysis. Archives of Otolaryngology 1968; 87: 289-291.
12. Luchsinger R, Arnold GE. Voice- Speech- Language - Clinical Communicology: Its Physiology and Pathology. Belmont, CA: Wadsworth Publishing Co., Inc 1965; 144-147.
13. Boehme G. The effectiveness of electrotherapy in laryngeal diseases as shown in the stroboscopic picture. Z Larryngology Rhino Otology 1965; 44(7): 481-488.
14. Iakovlva I, Iliutovich, GH, Iuvalova ND. On the use of sinusoidal low frequency modulated currents in vocal disorders in patients with paralysis and paresis of the laryngeal muscles. Vestnik Oto-Rino- Laryngologie 1965; 27(5): 93-98.
15. Pozsgay J, Heckenast O, Vincze L. Conservative management of recurrent nerve paralysis. HNO 1967; 15: 273-276.
16. Full-Scharrer G. Phoniatric possibilities in vocal cord paralysis. Laryngologie, Rhinologie, & Otologie 1974; 53: 585-590.
17. Plath P, Philips H. Post influenza vocal cord paralysis in a child. HNO 1974; 22(2): 59-60.
18. Kruse E. Phoniatric therapeutical possibilities for the parlysis of the vocal lips in paramedian position following strumectomy. Laryngologie, Rhinologie, Otologie 1978; 57(1): 26-31.
19. Martin, F. Peripheral Neurogenic paralysis of the vocal cord: Diagnosis and therapy. Muenchener Medizinische Wochenschrift (MMW) 1982; 124(45): 998-1002
.
20. Schleier E. Streubel HG. Relation between diagnostic prognosis and therapeutic results in recurrent laryngeal nerve paralysis. Folia- Phoniatrics (Basel) 1980a; 32(4): 323-333.
21. Schleier E, Streubel HG. Results of the treatment of hyperfunctional dysphonia and atony of the thyroarytenoid muscles by a combined voice stimulation therapy with a synchronic exponential current. Folia Phoniatrica 1980b; 32(1): 70-7.
22. Miehlke A, Arnold R, Kleinsasser O, et al. Reconstruction of function in vocal cord paralysis. Round table discussion]. Laryngologie, Rhinologie, Otologie 1986; 65(1): 1-4.
23. McFarlane SC, Holt-Romeo TL, Lavorato AS, Warner L. Unilateral vocal fold paralysis: Perceived vocal quality following three methods of treatment. Asha 1991; 27: 114-115
24. Attieh A, Perlmann A. Pneumatic Recording of Vocal Fold Adduction by Direct Electrical Stimulation. Unpublished Pilot Study, University of Iowa, Iowa City, Iowa, 1986.
25. Hvidegaard T, Vase P, Jorgensen K, Blichert M. Identification, and functional recording of the recurrent laryngeal nerve by electrical stimulation during neck surgery. Laryngoscope 1983; 93(3): 370-373.
26. Riddell V. Thyroidectomy: Prevention of bilateral recurrent nerve palsy. British Journal of Surgery 1970; 57: 1-11.
27. Shedd DP, Durhan C. Electrical identification of the recurrent laryngeal nerve: I. Responses of the canine larynx to electrical stimulation of the recurrent laryngeal nerve. Annals of Surgery 1966; 163 (1): 47-50.
28. Shedd DP, Burget GC. Identification of the recurrent laryngeal nerve: Electrical method for evaluation in the human. Archives of Surgery 1966; 92: 861-864.
29. Sanders I, Jonathan, A, Biller, HF. Transcutaneous electrical stimulation of the recurrent laryngeal nerve: A method of controlling vocal cord position. Otolaryngology- Head and Neck Surgery 1986; 95(2): 152-157.
30. Spahn JG, Bizal J, Ferguson S, Lingeman RE. Identification of the motor laryngeal nerves: A new electrical stimulation technique. The Laryngoscope 1981; 91(11): 1865-1868.
31. Miehike A. Reconstruction of function in vocal cord paralysis. Laryngologie, Rhinologie, and Otologie 1986; 65(1): 1-4.
32. Broniatowski M, Kaneko S, Jacobs G, et al. Laryngeal pacemaker. II Electronic pacing of reinnervated posterior cricoarytenoid muscles in the canine. Laryngoscope 1985; 95: 1194-1198.
33. Boone DR, McFarlane SC. The Voice and Voice Therapy. 6th Ed. Boston. Allyn & Bacon. 2000; 5: 148-149.
34. Eckel FC, Boone DR. The S/Z ratio as an indicator of laryngeal pathology. JSHD 1981; 46: 147-49.
35. Neale JM, Liebert RM. Science and Behavior: An Introduction to Methods of Research, 2nd Ed. Englewood Cliffs, NJ: Prentice-Hall, Inc. 1980; 155-156.
Appendix 1
Group I: Unilateral vocal fold paralysis following total or partial unilateral Thyroidectomy
|
Case
|
Name
|
Age/Sex
|
Side
|
Duration
|
No. of Sessions
|
Pre-post Phonation
|
Pre-post
Ratings
|
|
1
|
NZ
|
50 F*
|
Rt^
|
1 week
|
52
|
3-22 Secoo
|
3 – 10
|
|
2
|
RW
|
44F
|
Rt
|
9 mo.o
|
30
|
2 - 5 Sec
|
2 – 6
|
|
3
|
HQ
|
27 F
|
Lt^^
|
2.5 mo.
|
23
|
4 – 15 Sec
|
4 – 9
|
|
4
|
YY
|
59 F
|
Rt
|
11 mo.
|
29
|
4 – 11 Sec
|
4 – 8
|
|
5
|
AH
|
40 F
|
Lt
|
2 mo.
|
14
|
5 – 9 Sec
|
3 – 6
|
|
6
|
BH
|
42 F
|
Rt
|
3 mo.
|
17
|
6 – 19 Sec
|
6 – 10
|
|
7
|
AN
|
50 F
|
Lt
|
3 mo.
|
30
|
0 – 14 Sec
|
2 – 9
|
|
8
|
ND
|
38 F
|
Bil.‡
|
2 weeks
|
49
|
0 – 13 Sec
|
2 – 10
|
|
9
|
ZH
|
21 F
|
Lt
|
2 mo.
|
20
|
2 – 20 Sec
|
4 – 10
|
|
10
|
MS
|
42 M**
|
Rt
|
3 mo
|
19
|
4 – 8 Sec
|
4 – 7
|
|
11
|
BI
|
37 M
|
Lt
|
4.5 mo.
|
29
|
7 – 15 Sec
|
7 – 9
|
|
12
|
OL
|
35 M
|
Rt
|
3 week
|
26
|
3 – 6 Sec
|
4 – 8
|
|
13
|
OH
|
44 M
|
Lt
|
15 mo.
|
35
|
4 – 7 Sec
|
3 – 6
|
|
14
|
IB
|
19 M
|
Rt
|
2 mo.
|
15
|
0 – 12 Sec
|
2 – 9
|
|
15
|
AZ
|
25 M
|
Rt
|
4 yrs
|
17
|
5 – 10 Sec
|
5 – 8
|
|
16
|
MJ
|
30 F
|
Rt
|
2 mo.
|
22
|
5 – 11 Sec
|
4 – 8
|
|
17
|
WE
|
41 F
|
Lt
|
3 mo.
|
21
|
7 – 14 Sec
|
6 – 8
|
|
18
|
ZR
|
58 F
|
Rt
|
1 week
|
35
|
0 – 17 Sec
|
3 – 10
|
|
19
|
DN
|
34 F
|
Rt
|
3 week
|
21
|
4 – 17 Sec
|
4 – 10
|
|
20
|
MM
|
62 M
|
Lt
|
1 mo.
|
19
|
8 – 17 Sec
|
7 – 10
|
|
21
|
NN
|
16 F
|
Rt
|
1 mo.
|
33
|
6 – 15 Sec
|
5 – 9
|
*F: Female **M: Male ^Rt: Right ^^ Lt: Lift ‡Bil: omo: month ooSec: Second
Appendix 2
Group II: Unilateral vocal fold paralysis following neck and thoracic surgery (Bullet injury, tumor removal, etc.)
|
Case
|
Name
|
Age/Sex
|
Side
|
Duration
|
No. of Session
|
Pre-post Phonation
|
Pre-post
Ratings
|
|
1
|
MF
|
52M*
|
Lt^^
|
1 year
|
12
|
3 – 3 Secoo
|
4 – 5
|
|
2
|
MS
|
65M
|
Lt
|
5 mo. o
|
20
|
5 – 6 Sec
|
4 – 6
|
|
3
|
AG
|
69M
|
Lt
|
7 mo.
|
20
|
2 – 13 Sec
|
3 – 9
|
|
4
|
AR
|
44 M
|
Lt
|
6 mo.
|
18
|
8 – 13 Sec
|
5 – 8
|
|
5
|
JW
|
49 M
|
Lt
|
5 mo.
|
21
|
1 – 7 Sec
|
3 – 7
|
|
6
|
OL
|
30 M
|
Rt^
|
2 week
|
30
|
0 – 8 Sec
|
3 – 9
|
|
7
|
SL
|
52M
|
Lt
|
6 mo.
|
17
|
4 – 11 Sec
|
3 – 7
|
|
8
|
FA
|
25 M
|
Lt
|
7 mo.
|
15
|
4 – 5 Sec
|
6 – 8
|
|
9
|
SF
|
27 F**
|
Lt
|
2.5 mo.
|
29
|
2 – 10 Sec
|
5 – 8
|
|
10
|
KB
|
28 F
|
Lt
|
2 mo.
|
36
|
0 – 8 Sec
|
2 – 7
|
|
11
|
HS
|
40M
|
Lt
|
4 mo.
|
19
|
2 – 11 Sec
|
4 – 7
|
|
12
|
IZ
|
34M
|
Lt
|
4 mo.
|
19
|
4 – 12 Sec
|
5 – 10
|
|
13
|
LY
|
29F
|
Lt >Rt
|
2 mo.
|
19
|
0 – 9 Sec
|
2 – 6
|
|
14
|
RT
|
59M
|
Lt
|
8 mo.
|
19
|
3 – 8 Sec
|
5 – 8
|
|
15
|
JH
|
66M
|
Lt
|
1.5 mo
|
31
|
1 – 10 Sec
|
5 – 8
|
|
16
|
OD
|
53 M
|
Lt
|
1.2 year
|
20
|
3 – 8 Sec
|
4 – 8
|
*F: Female **M: Male ^Rt: Right ^^ Lt: Lift omo: month ooSec: Second
Appendix 3
Group III:Unilateral vocal fold paralysis following viral infection
|
Case
|
Name
|
Age/Sex
|
Side
|
Duration
|
No. of Sessions
|
Pre-post Phonation
|
Pre-post
Rating
|
|
1
|
IN
|
30 F*
|
Lt^^
|
6 years
|
28
|
4 – 6 Secoo
|
5 – 7
|
|
2
|
ZS
|
57 F
|
Lt
|
7 moo
|
29
|
4 – 14 Sec
|
6 – 10
|
|
3
|
OR
|
27 M**
|
Lt
|
3 weeks
|
17
|
5 – 9 Sec
|
6 – 9
|
|
4
|
GF
|
66 F
|
Rt^
|
3 mo
|
23
|
0 – 17 Sec
|
4 – 10
|
|
5
|
FR
|
45 M
|
Lt
|
8 mo
|
20
|
3 – 12 Sec
|
4 – 8
|
|
6
|
FZ
|
40 M
|
Lt
|
1 mo
|
18
|
1 – 9 Sec
|
3 – 8
|
|
7
|
SH
|
38 F
|
Lt
|
7 mo
|
17
|
4 – 8 Sec
|
5 – 9
|
|
8
|
AW
|
63 M
|
Lt
|
3 weeks
|
29
|
4 – 18 Sec
|
5 – 10
|
|
9
|
KF
|
20 M
|
Lt
|
1 mo
|
16
|
3 – 12 Sec
|
4 – 8
|
|
10
|
YR
|
38 M
|
Lt
|
1 mo.
|
22
|
10 – 32 Sec
|
6 – 10
|
|
11
|
KZ
|
24 M
|
Rt
|
3 mo
|
19
|
4 – 8 Sec
|
4 – 6
|
*F: Female **M: Male ^Rt: Right ^^ Lt: Lift omo: month ooSec: Second
Appendix 4
Group IV: Idiopathic unilateral vocal fold paralysis
|
Case
|
Name
|
Age/Sex
|
Side
|
Duration
|
No. of Sessions
|
Pre-post Phonation
|
Pre-post
Rating
|
|
1
|
AK
|
40 M**
|
Lt^^
|
2 moo
|
15
|
8 – 24 Secoo
|
4 – 9
|
|
2
|
HM
|
34 M
|
Lt
|
5 mo
|
14
|
2 – 7 Sec
|
4 – 7
|
|
3
|
AL
|
59 F*
|
Rt^
|
3.5 mo
|
25
|
6 – 19 Sec
|
6 – 10
|
|
4
|
IB
|
24 F
|
Lt
|
2 year
|
22
|
3 – 6 Sec
|
4 – 6
|
|
5
|
NS
|
22 M
|
Rt
|
2 mo.
|
21
|
13 – 20 Sec
|
5 – 9
|
|
6
|
OZ
|
23 F
|
Rt
|
4 mo.
|
24
|
8 – 22 Sec
|
6 – 10
|
|
7
|
NH
|
25 M
|
Rt.
|
2 mo.
|
30
|
8 – 20 Sec
|
7 – 9
|
|
8
|
RS
|
35 F
|
Lt
|
2 mo
|
21
|
2 – 13 Sec
|
4 – 8
|
|
9
|
HL
|
49 F
|
Lt
|
5 mo
|
15
|
4 – 6 Sec
|
5 – 7
|
|
10
|
MR
|
33 M
|
Lt
|
1 mo
|
16
|
2 – 6 Sec
|
5 – 7
|
|
11
|
NW
|
60 F
|
Lt.
|
2 mo.
|
27
|
2 – 11 Sec
|
4 – 8
|
|
12
|
TS
|
50 M
|
Rt.
|
18 mo.
|
32
|
10 – 22 Sec
|
6 – 10
|
*F: Female **M: Male ^Rt: Right ^^ Lt: Lift omo: month ooSec: Second