Objective: To investigate the relationship between maternal chronic periodontal disease and preterm low birth weight.
Methods: A case-control study was performed on 103 pregnant or post partum women seen at Prenatal Care Clinic in Prince Hashem Hospital in Zarqa- Jordan. The study group preterm low birth weight cases were defined as a mother with a birth of < 2500g and with preterm labor (gestational age < 37 weeks), while control group cases were mothers with new born of > 2500g and born after 38 weeks. Assessment for the known risk factors for preterm low birth weight, such as age, prenatal care, smoking, etc. was achieved by filling a data questionnaire. Each subject also received a periodontal examination to determine clinical attachment loss, probing pocket depth and gingival bleeding on probing.
Results: The study group preterm low birth weight consisted of 54 cases of which 19 were primiparous, while the control group consisted of 49 cases of which 18 were primiparous. A statistically significant relationship was found between preterm low birth weight and clinical attachment loss, bleeding on probing and probing pocket depth for primiparous and all mothers (p < 0.05). Also, in spite of adequate prenatal care, mothers tended to have preterm low birth weight. However, no significant correlation could be drawn with other risk factors.
Conclusion: Periodontal disease represents a statistically significant risk factor for preterm low birth weight. However, further studies are required to demonstrate a causal relationship between maternal periodontal disease and preterm low birth weight and to detect whether prevention and treatment of periodontal disease can reduce the incidence of preterm low birth weight.
Key words: Preterm low birth weight, Periodontal disease, Risk factors.
JRMS Dec 2005: 12(2): 36-41Introduction
While infant mortality rate has declined in past years, low birth weight (< 2,500g) in pre-term infants (< 37 weeks) remains a significant cause of perinatal mortality. Recognized risk factors for preterm low birth weight (PLBW) include: Older (>34 years) or younger (<17 years) maternal age; low socio-economic status; inadequate prenatal care; drug abuse; alcohol and tobacco use; hypertension; genitourinary tract infections, diabetes, and multiple pregnancies (1).
Several studies have demonstrated an association between infection, especially lower genitourinary tract infection and PLBW (2-4). PLBW, which occurs as a result of infection, is mediated indirectly, principally by the translocation of bacterial products such as endotoxins (lipopolysaccharides) (LPS), and by the action of maternally produced inflammatory mediators (5).
However, the observation of elevated inflammatory mediators, prostaglandin E2 (PGE2) and tumor necrosis factor-α (TNF-α) even in the absence of any genitourinary tract infection, has led to the conclusion that most PLBW cases are “ probably caused by an infection of unknown origin” (6).
Periodontal disease is a group of inflammatory conditions affecting the supporting structures of teeth. They are associated with chronic gram-negative infections that provide bacterial components such as LPS, which trigger release of PGE2 and TNF-α that, in turn, may influence the course or outcome of pregnancy. Evidence to support this model has been obtained from animals, where fetal growth was retarded when pregnant golden hamsters were exposed to periodontal infection (7).
Microbiologically, however, periodontal pathogens and / or their inflammatory products may have a role in prematurity via a hematogenous route (8).
Maternal serum immunoglobulin levels against various periodontal pathogens were found to be higher in PLBW group of mothers compared to mothers delivering infants with normal birth weight (NBW) (9-11). Moreover, a significant association between microbial DNA in amniotic fluid of mothers and previous pregnancy complications such as spontaneous abortions, preterm delivery, etc. was detected (12).
Investigating periodontal health with PLBW, Offenbacher et al (13) determined that mothers with periodontal infection had more than seven times the risk of delivering a PLBW infant. The extent and severity/ incidence and progression of periodontal disease were shown to be higher in women delivering an infant with PLBW than in mothers delivering one with normal birth weight (14-17).
Furthermore, periodontal therapy was found to reduce the incidence of PLBW in pregnant women (18). In the contrary, Davenport et al (19), found no evidence for the association between PLBW and maternal periodontal disease.
Collectively, the animal, microbial and clinical studies clearly indicate a possible association between periodontal infection and adverse pregnancy outcomes. This background had led us to undertake the present investigation to estimate the association between maternal chronic periodontal disease and PLBW.
MethodsStudy design and populationA case-control study design was chosen as most appropriate because PLBW is comparatively rare. The participants were women being seen for routine care in the Prenatal Care Clinic - Prince Hashem Ben Al-Hussein Hospital (PHHH) in Zarqa - Jordan, or in-patients at the Obstetrics and Gynecology ward in the same hospital during the period of study (6 months). The controls were selected randomly (using random number tables) from eligible mothers either seen for routine care in the Prenatal Care Clinic or present on the ward on a particular weekday.
A total of 103 volunteer Jordanian women 17-40 years old were included in this study. No volunteer had exhibited risk factors for bacterial endocarditis, which would have required antibiotic prophylaxis preceding a periodontal examination. Each participant received an appropriate description of the study and signed a consent form.
Pregnancy outcomes and risk factorsUsing a computer based questionnaire, mothers were asked a series of questions to ascertain the following details related to the previous pregnancy history and the current pregnancy. These questions included terms and birth weights of all previous births. In addition, a detailed profile of all risk factors for PLBW was assessed for each patient, including: Age, parity, medications, smoking habit, alcohol use, maternal general health during pregnancy, especially genitourinary tract infections and treatment, prenatal care and socio-economic status (Table I). Socio-economic status was assessed by dividing the women into three groups according to the family monthly income. Families in the lowest income group earn 135 Jordanian Dinars (JDs) or less, which is the poverty line in Zarqa Goverernorate (Ministry of Social Development) (20), while families in the highest income group earn 500 JDs or more. Group of families in the middle earn monthly income in between.
Periodontal measurementsA complete periodontal examination was performed on all 103 mothers either during the time of volunteering at the Prenatal Care Clinic or within 3 days of their delivering at PHHH. Full-mouth data were recorded on probing pocket depth (PPD) and clinical attachment loss (CAL) on six sites per tooth using a disposable pressure-sensitive probe (Vivacare TPS, Vivadent, Schaan, Liechtenstein, Germany). The examiner (periodontist, DMD) measured CAL, with the cemento-enamel junction (CEJ) serving as the reference point. Bleeding on probing (BOP) was measured and expressed as a percentage of sites that bled upon probing. The examiner was masked from obstetric data.
Case definitionAlthough clinical attachment loss (CAL) is the most commonly used measure of periodontal disease, it is an accumulative measure and can include both active and inactive sites. Once attachment loss occurs, the evidence of disease remains in the mouth and that site may or may not be currently active. This means that our measure of CAL also may have occurred with a previous PLBW infant, but that the current birth was NBW. Thus, two definitions for the case were adopted. In the first definition, study group cases were defined as mothers delivering an infant weighing less than 2,500g and born before 37 weeks gestation at this pregnancy, or who had a history of PLBW in the past. The control group cases were women delivering an infant weighing more than 2,500g and born after 38 weeks gestation, and who had no prior abnormal pregnancy outcome history. The second definition of a case was the same as for case and control, except that the group was restricted to mothers having their first baby (primiparous).
Data management and statistical analysisPregnancy outcomes were categorized into cases and controls for two groups of mothers; all mothers and primiparous mothers. For each group, periodontal disease status was first defined using full-mouth, mean CAL (mean CAL mm/site) for each patient, pooling to form group means. Probing pocket depth (PPD) was calculated as for CAL. A second case-control definition was used for modeling to limit the data to primiparous women to remove any effect of previous births or any potential error on previous births reporting.
This additional model was developed using a case definition of primiPLBW, with primiNBW mothers serving as controls. All collected data were coded, computerized, and analyzed using the Statistics Program for Social Sciences Version 11 (SPSS ©) software. Frequency distributions were compared between the cases (Any PLBW and primiPLBW) and controls (All NBW and PrimiNBW) using Chi-square analysis and the significance level was set at 5%.
Results
During the study period (6-months), we examined 54 PLBW (52.4%) cases of which 19 (35.2%) were primarous and 49 (47.6%) NBW or control case of which 18 (36.7%) were primiparous (Fig. 1).
The mean age was 27.2 years (SD, 4.6) for the PLBW group and 27.0 (SD, 4.1) for the NBW group indicating no significant difference (p> 0.05) between the two groups. The age distribution of study and control group cases is presented in (Fig. 2). The primiparous mothers tended to be younger in comparison to the group of multiparous mothers with mean ages of 24.54 (SD, 3.0) and 28.56 (SD, 4.3) respectively. However, age distribution was not significantly different comparing cases to controls for all the mothers or the primiparous ones (p > 0.05).
Socio-economically, mothers living in lowest income group formed 4.0% of the PLBW cases, compared to 0.0% in the control group. Most of the subjects under study were in the middle group that formed 74% of the PLBW cases and 69% of the controls, while 22% of the cases located in the highest income group compared to 31% of the controls. However, socio-economic status showed no significant correlation with PLBW either for all the mothers or for the primiparous ones, (p > 0.05).
Parity as a possible risk factor for PLBW showed no significant correlation with PLBW (p > 0.05). Data showed that mothers with previous live births were comparable in the study and control group cases as follows: For 1 live birth 17.1% compared to 19.4% while 28.7% of the cases had 2 live births compared to 25.8% of the controls. For 3 live births, the figure was 17.1% compared to 38.7%, while for 4 live births it was 17.1% compared to 6.4%. Mothers in the case group with 5 or more live births formed 20% compared to 9.7% in the controls.
Of the studied population, data revealed that 41 (75.9%) of the PLBW cases attended the Prenatal Care Clinic adequately (i.e.
6 visits), whereas 13 subjects (24.1%) did not. Similarly, most of the subjects in the control group (98%) received adequate prenatal care. In the primiparous group, 78.9% of PLBW cases attended the clinic adequately compared to 21.1% who failed to attend. For the control group, the figures are similar where all the mothers received adequate care. However, there was a statistically significant relationship between PLBW and mother attendance to the Prenatal Care Clinic (p < 0.05).
A genitourinary tract infection, as an obstetric history variable, was a marginally statistically significant factor (p = 0.05), associated with any PLBW cases but not primiPLBW. Neither tobacco or alcohol use, nor medications differed among the groups as none of the subjects under study consumed alcohol, tobacco or had taken any medication other than tonics. Moreover, none of the cases or controls was diabetic or hypertensive or had hemoglobin levels less than 28mg/ dl during this pregnancy.
Relation between PLBW and periodontal diseaseComparison of the mean CAL between PLBW case and control mothers demonstrated significant differences. Fig. 3 illustrates that the 54 PLBW cases has a mean CAL of 4.24± 0.69 mm/ site. By comparison, the 49 NBW controls have a mean CAL of 2.05 ± 0.31 mm/ sites, which was significantly less than the cases at p < 0.05.
Table II shows the case-control comparisons using PPD, % of sites that bled upon probing, in addition to CAL as periodontal disease indicators. PPD and BOP have shown a statistically significant association with PLBW (p < 0.05).
All cases and control subjects exhibited BOP, with a range of 4 - 50% for the cases and 15 - 30% for the controls. The primiparous cases had significantly more severe periodontal disease than primiparous controls, based upon mean CAL, PPD, and % of sites exhibited BOP (p < 0.05). Thus, the periodontal condition of the primiparous cases was significantly worse than primiparous controls.
Discussion
The major issues in designing a case - control study are ensuring firstly that controls are representative (by avoiding selection bias) and secondly that all potential confounding factors are measured. On recruitment of the subjects, cases and controls were selected at random from the same pool – mothers seen at Prenatal Care Clinic at PHHH who later delivered on the ward, and the clinician (Periodontist) was blinded to the selection process. Moreover, the community from which most of the subjects were drawn is a specific inner - Governorate population, and therefore, the study outcome should not necessarily be considered representative of other child – bearing women in Jordan, except in other areas with similar population profile.
One of the important variables in this study that had a significant correlation with PLBW was the level of prenatal care. In spite of adequate prenatal care (³ 6 visits), mothers tended to have PLBW. This implies the presence of another risk factor that might induces PLBW, which is potentially the maternal periodontal disease. This finding again enhances the relationship between periodontal status and PLBW.
Preterm infants who are born with low birth weight represent a major social and economic public health problem. The significance of the association between periodontal disease and PLBW re-opens new possibilities for an old concept, the focal infection. Galloway 1931 (21) first suggested that periodontal disease may “ provide sufficient infectious microbial challenge” to have “potentially harmful effects on the pregnant mother and developing fetus”. Periodontal disease, as remote gram-negative infections may have the potential to affect pregnancy outcome. Lipopolysaccharides (LPS), which are major components of the bacterial cell wall of gram-negative bacteria, can target the placental membrane via the blood stream. A series of experiments had clearly demonstrated that infections in pregnant animals could elicit many pregnancy complications including spontaneous abortion, preterm labor, low birth weight, fetal growth restriction and skeletal anomalies (15).
Standard clinical parameters for evaluation of the periodontal status have been well established in dentistry. At present, bleeding on probing, probing pocket depth and clinical attachment loss constitute the primary clinical measures, which are utilized by many practicing dentists to measure the periodontal condition of patients. In the present study, PLBW cases have shown more CAL, PPD and BOP in comparison to the control group. Periodontal status of primiparous cases was also worse than that for control group. Similar to these results, Offenbacher et al (13) have found that the mean CAL for PLBW cases was higher than that for controls. Even for primiparous cases, the mean CAL was higher in comparison with the control group; however, pocket depth and severity scores have not shown a statistically significant difference between cases and controls.
Therefore, they concluded that periodontal disease was significantly associated with PLBW and that risk appears to be independent of other known risk factors such as age, alcohol use, smoking, etc. However, another case-control study (15) used extent scores (extent of attachment level), for measurement of periodontal disease among mothers with PLBW. It found that the mean extent score (CAL ³4) for PLBW mothers was higher than that for control group, but this difference was not statistically significant which might be related to the small sample size (n = 44).
Furthermore, Offenbacher et al (16) used maternal periodontal disease status at antepartum, using a 3-level disease classification (health, mild, moderate- severe), and investigated the prevalence of gestational age, and birth weight. The results showed that the prevalence of preterm delivery, low birth weight, and low weight for gestational ages were higher among women with moderate- severe periodontal disease compared with women with mild periodontal disease or periodontally healthy mothers.
Despite these later findings, Davenport et al (19), in their case-control study on 236 cases and 507 controls, found that the risk for PLBW decreased with increasing probing pocket depth. This raises the question whether the relation between periodontal disease and PLBW is association or causation? However, further studies are required to confirm their results, as this is the only study with such results so far.
Assessing periodontal status for 700 mothers attending the Royal London Hospital in East London through Community Periodontal Index of Treatment Need (CPITN) scoring, Davenport et al (14) found a high prevalence of CPITN score 3 (38%) and 4 (49%) of the study population. This may reflect an elevation of gingival inflammation leading to enlargement of the gingiva and hence an increase in pocket depth and not necessarily an actual loss of connective tissue attachment.
Regarding gingival bleeding upon probing, it is likely that our results are significantly influenced by pregnancy. This is in agreement with Löe and Silness (22), who observed that all 121 pregnant women examined showed signs of gingival inflammation. Our results again go with the East London Study (14), where none of the subjects under study was free of gingival inflammation. Although gingival inflammation associated with pregnancy is thought to be reversed postpartum, most of the subjects were examined clinically within 3 days after delivery, at which stage little resolution of the gingival inflammation would be expected.
Although periodontal disease was the strongest factor among other known obstetric risk factors for PLBW, it seems that pregnant women with periodontal disease may benefit from periodontal therapy to reduce the incidence of PLBW (18), however further studies are needed to confirm these results.
In summary, preliminary indications from this case–control study of the relation between PLBW and maternal periodontal disease suggest that there is a statistically significant relationship between PLBW and maternal periodontal disease. Future larger prospective multi-center studies are needed to confirm results obtained from this small case – control study and to determine a causal relationship between periodontal disease and PLBW. Considering the fact that periodontal disease is preventable and treatable, the question that needs to be investigated is whether intervention strategies through periodontal therapy and improving oral health can reduce the incidence of PLBW.
Table I: Data collection form
|
Identification
|
File number, date,
name
|
|
Demographic data
|
Age, parity,
socio-economic status, prenatal care
|
|
Medical information
|
Health status during
pregnancy, genitourinary tract infection, medications
|
|
Habits
|
Alcohol use, smoking
|
|
Obstetric data
|
Previous pregnancy
outcomes, birth weight, length of gestation
|
Table II:Mean and standard deviation for periodontal measurements between the study and control groups
|
Variable
|
Any PLBW
Cases
Mean ±SD
|
All NBW
Controls
Mean ±SD
|
PrimiPLBW
Cases
Mean ±SD
|
PrimiNBW
Controls
Mean ±SD
|
|
PPD (mm/site)
|
5.07 ± 0.67
|
2.95 ± 0.31
|
4.89 ± 0.66
|
2.72 ± 0.31
|
|
CAL (mm/site)
|
4.24 ± 0.69
|
2.05 ± 0.31
|
4.00 ± 0.67
|
1.92 ± 0.35
|
|
BOP %
|
41.85 ± 7.75
|
19.9 ± 4.59
|
43.21 ± 3.75
|
16.94 ± 3.49
|
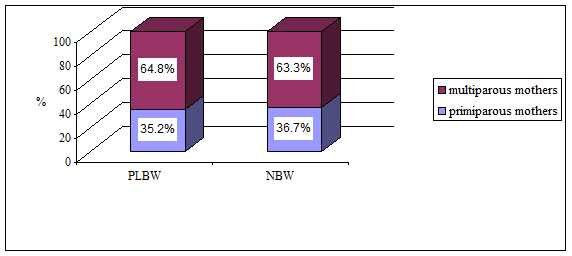 Fig. 1:
Fig. 1: Distribution of the study and control group cases
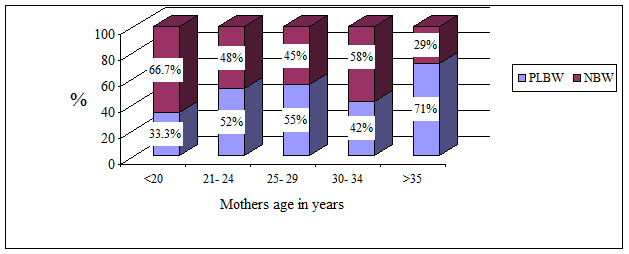 Fig. 2:
Fig. 2:Distribution of the study and control group cases by age.
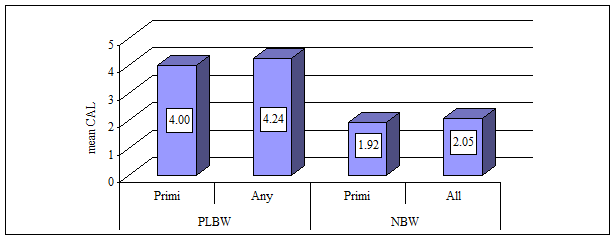
Fig. 3: The mean clinical attachment loss in the study and control groups
References1.
Position paper. Periodontal disease as a potential risk factor for systemic diseases. J Periodontol 1998; 69: 841-850.
2.
Niswander KR, Gordon M. The women and their pregnancies. The collaborative perinatal study of the National Institute of Neurological Diseases and Strokes. Philadelphia: W.B. Saunders 1972; 252- 256.
3.
White CP, Wilkins EGL, Roberts C, Davidson DC. Premature delivery and group B streptococcus bacteriurea. Lancet 1984; II: 69-70.
4.
Muller-Heubach E, Rubenstein DN, Schwarz SS. Histological chorioamnionitis and preterm delivery in different patient populations. Obstet Gynecol 1990; 75: 622- 626.
5.
Gibbs RS, Romero R, Hillier SL, et al. A review of premature birth and subclinical infections. Am J Obstet Gyenecol 1992; 166: 1515 - 1528.
6.
Romero R, Mazor M, Wu YAK, Avila C. Bacterial endotoxin and tumor necrosis factor stimulate prostaglandin production by human decidua. Prostaglandins Leukot Essent Fatty Acids 1989; 37: 183 - 185.
7.
Collins JG, Kirtland BC, Arnold RR, Offenbacher S. Experimental periodontitis retards hamster fetal growth. J Dent Res 1995; 74: 158 - 162.
8.
Hill GB. Preterm birth: Association with genital and possibly oral microflora. Ann Periodontol 1998; 3: 222- 232.
9.
Offenbacher S, Madianos PN, Suttle M, et al. Elevated human IgM suggests in utero exposure to periodontal pathogens. J Dent Res 1999; 78: 2191 - 2193.
10.
Dasanayake AP, Boyd D, Madianos PN, et al. The association between porphyromonas gingivalis- specific maternal serum IgG and low birth weight. J Periodontol 2001; 72: 1491-1497.
11.
Madianos PN, Lieff S, Murtha AP, et al. Maternal periodontitis and prematurity. Part II: Maternal infection and fetal exposure. Ann Periodontol 2001; 6: 175- 182.
12.
Teng A, Taylor G, Scannapieco F, et al. Periodontal health, and systemic disorders. J Can Dent Assoc 2002; 68: 188- 192.
13.
Offenbacher S, Vern K, Fertik G, et al. Periodontal infection as a possible risk factor for preterm low birth weight. J Periodontol 1996; 67: 1103- 1113.
14.
Davenport ES, Williams CE, Sterne JA, et al. The East London study of maternal chronic periodontal disease and preterm low birth weight infants: Study design and prevalence data. Ann Periodontol 1998; 3: 213- 221.
15.
Offenbacher S, Jared HL, O’Reilly SR, et al. Potential pathogenic mechanisms of periodontitis-associated pregnancy complications. Ann Periodontol 1998; 3: 233- 250.
16.
Offenbacher S, Lieff S, Boggess KA, et al. Maternal periodontitis and prematurity. Part I: Obstetric outcome of prematurity and growth restriction. Ann Periodontol 2001; 6: 164-174.
17.
Lopez NJ, Smith PC, Gutierrez J. Higher risk of preterm birth and low birth weight in women with periodontal disease. J Dent Res 2002; 81: 58- 63.
18.
Lopez NJ, Smith PC, Gutierrez J. Periodontal therapy may reduce the risk of preterm low birth weight in women with periodontal disease: A randomized controlled trial. J Periodontol 2002; 73: 911- 924.
19.
Davenport ES, Williams CE, Sterne JA, et al. Maternal periodontal disease and preterm low birth weight: Case-control study. J Dent Res 2002; 81: 313- 318.
20.
Ministry of Social Development. Characterestics of poverty in Jordan, Ministry of social development, Amman, Jordan 1993.
21.
Galloway CF. Focal infection. Am J Surg 1931; 14: 643- 645.
22.
Löe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol Scand 1966; 21: 533- 549.