A 15-year-old male patient with a history of nasal obstruction, recurrent epistaxis, proptosis and loss of vision in his right eye. The diagnostic workup (clinical, endoscopic, radiological and histopathological) confirms the diagnosis of nasal olfactory neuroblastoma.
Key word: Olfactory, neuroblastoma, Nose.
JRMS Dec 2005; 12(2): 48-50 Introduction
Olfactory neuroblastoma (ON) or esthesioneuroblastoma (ENB) is an uncommon malignant neoplasm of neural origin arising from the olfactory sensory epithelium in the nasal cavity (1,2). It was first described by Berger et al in 1924 (3). It is now accepted that the tumor is neuroectodermal in origin and in most patients arises high (in the roof or lateral wall of the nose) close to the ethmoidal labyrinth, the area of olfactory epithelium. This tumor has a broad histological spectrum and it can be confused histologically with peripheral neuroectodermal tumors (4).
The common clinical symptoms include nasal obstruction, recurrent epistaxis, hyposmia, rhinorrhea, headaches, and visual disturbances (1,5). As the tumor grows, it tends to spread submucosally in all directions to involve the paranasal sinuses, nasal cavity, and the surrounding structures (the oral cavity, the orbits, and the brain) (5-7). The tumor is locally invasive, and local recurrence strikes in up to 68% of cases regardless of initial treatment protocol (8,9). We describe a patient with olfactory neuroblastoma who presented with symptoms similar to those mentioned above.
Case Report
A 15-year-old male patient came to our clinic with right nasal obstruction, recurrent epistaxis and proptosis, loss of vision in the right eye, and headache of three weeks duration. Diagnostic endoscopy revealed an irregular large mass in the right nasal cavity occupying the upper 2/3 of the nose. The mass was bluish in color, partially necrotic and insensitive to touch. Ophthalmic examination revealed proptosis of the right eye with total loss of vision.
Coronal and axial CT scan of the nose and sinuses were performed and showed a large soft tissue mass in the right superior nasal cavity that extended into the ethmoid, sphenoid sinuses and skull base with extension into both orbits more to the right side (Fig. 1, 2).
The patient subsequently underwent magnetic resonance imaging, which showed cribriform plate involvement without intracranial extension, no cervical or distance metastasis has been detected. Angiography showed a mass with moderate contrast enhancement.
An endoscopically- guided biopsy from the mass was performed under general anesthesia. A histopathological diagnosis of olfactory neuroblastoma was made based on immunohistochemistry. Hormonal assay: adrenocortico-tropic (ACTH) and antidiuretic hormone level, were normal.
The surgical plan was to excise the tumor through a right external ethmoidectomy with partial medial maxillectomy and sphenoidectomy; in case the histopathology revealed residual tumor in the ethmoid specimen, we arranged to give him postoperative radiotherapy. But according to his family wish the patient was sent abroad to a cancer center in which he was treated with chemotherapy alone.
Discussion
Olfactory neuroblastoma, also called esthesio-neuroblastoma is a relatively uncommon intranasal tumor that originates from olfactory epithelium in the upper nasal cavity in the region of the cribriform plate. Berger and Richard first described it in 1924. Only 250 cases have been recorded since (1).
It occurs in all age groups with a peak incidence in the age groups of 11 to 20 years and 51 to 60 years (Elkon et al) (2).
The tumor shows a relatively homogeneous population of small round cells set in a variable fibrillary stroma and forms part of the differential diagnosis of round cell lesions of the head and neck region (10).
The presence of a fibrillary intercellular background in conjunction with the presence of Homer - Wright rosettes in an upper nasal neoplasm is considered to be diagnostic of olfactory neuroblastoma (5).
It accounts 1 to 5% of malignant neurological neoplasms (11). There is no true sex predominance, but some authors report a male-female ratio of 2:1 (11,12).
The tumor is not usually associated with hormone secretion, but in some cases it has been found to be an arginine vasopressin producer causing inappropriate antidiuretic hormone secretion syndrome. In one case olfactory neuroblastoma was found to produce adrenocorticotropic hormone, causing Cushing syndrome. (10)
Classification is based on the extent of tumor invasion; the staging system proposed by Kadish et al in 1976 (8,9) provides a reference point for therapy and prognosis. (Table I, II)
Table I: Kadish classification
|
Stage
|
Location
|
5 year survival
|
|
A
|
Disease confined to the nasal
cavity
|
75%
|
|
B
|
Disease confined to the nasal
cavity and paranasal sinuses
|
68%
|
|
C
|
Local or distant spread
beyond the nasal cavity or sinuses
|
41%
|
Our patient was in stage C, based on Kadish classification as the tumor had spread beyond the nasal cavity and the sinuses to the orbit.
The tumor metastasizes widely by both hematogenous and lymphatic routes (Table II). The cervical lymph nodes are the most common site of metastases followed by the lungs, abdominal organs, long bones, and pelvis (8,9).
Table II: Disease distribution
|
Local disease
|
68%
|
|
Nodal involvement
|
22%
|
|
Distal spread
|
16%
|
Regardless of the grade or stage (with the possible exception of distant metastasis), surgery is the recommended therapy in patients harboring these tumors (15,16). Surgical treatment alone is effective in cases of low-grade tumor if tumor-free margins can be obtained. The use of adjuvant radiotherapy is supportive for low-grade tumors when the margins are close, for residual or recurrent disease and for all high-grade tumors (12).
Some authors argue that radiation is best administered preoperatively (13), where others prefer to administer it postoperatively (14,17-19), and yet others recommend postoperative radiotherapy for stage A tumors and preoperative radiotherapy for higher-stage lesions (stages B and C) (15).
More recently, chemotherapy combined with resection and radiotherapy, have been used to treat advanced stage, high-grade, and recurrent ONS with durable remission periods (13,20). Long time follow-up is necessary.
Fig 1 and 2 CT scan shows a large soft tissue mass in the right superior nasal cavity that extends into the ethmoid, sphenoid sinuses and skull base with extension into both orbits more in the right side
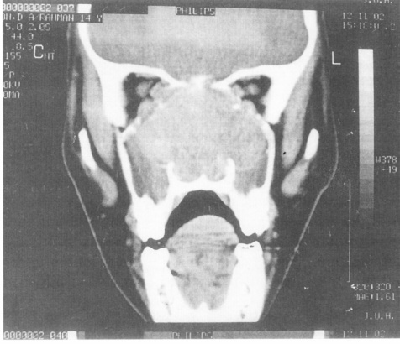 Fig. 1:
Fig. 1: A coronal CT of the nose and sinuses.
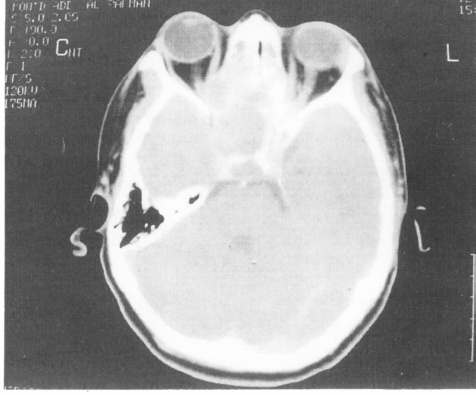 Fig. 2:
Fig. 2: Axial CT of the nose and sinuses.
References
1.
Lund VJ, Milroy C. Olfactory neuroblastoma: Clinical and pathological aspects. Rhinology 1993; 31:1-6.
2.
Elkon D, Hightower SI. Esthnesioneuroblastoma. Cancer 1979; 44: 1087-94.
3.
Berger L, Luc G, Richard D. L’esthesioneuro-epitheliome olfactif. Bull Assoc Franc Etude Cancer 1924; 13: 410.
4.
Nelson RS, Perlman EJ, Askin FB. Is esthesioneurablastoma a peripheral neuroectodermal tumor? Hum Pathol 1995; 26: 639-641.
5.
Mills SE, Frierson HF Jr. Olfactory neuroblastoma: A clinicopathologic study of 21 cases. Am J Surg Pathol 1985; 9: 317-327.
6.
Myers SL, Hardy DA, Wiebe CB, Shiffman J. Olfactory neuroblastoma invading the oral cavity in a patient with inappropriate antidiuretic hormone secretion. Oral Surg Oral Med Oral Pathol 1994; 77: 645-650.
7.
Batsakis JG. Tumors of the head and neck. 2nd. Baltimore: Williams and Wilkins, 1979: 338-349.
8.
Kadish S, Goodman M, Wang CC. Olfactory neuroblastoma. A clinical analysis of 17 cases. Cancer 1976; 23: 1571-1676.
9.
Anavi Y, Bahar M, Ben Bassat M. Olfactory neuroblastoma: Report of a case and review of the literature. J Oral Maxillofac Surgery 1989; 47: 514
10.
Chaudhry MR, Akhtar S, Kim DS. Neuroendocrine carcinoma of the ethmoid sinus. Eur Arch Otorhinolaryngol 1994; 251: 461-463.
11.
O’Connor TA, Mclean P, Juillard GJ, et al. Olfactory neuroblastoma. Cancer 1989; 63: 2426-2428.
12.
Morita A, Ebersold MJ, Olsen KD, et al. Esthesioneuroblastoma: prognosis and management. Neurosurgery 1993; 32: 706- 715.
13.
Eden BV, Debo RF, Larner JM, et al. Esthesioneuroblastoma long- term outcome and patterns of failure-the University of Virginia Experience. Cancer 1994; 73: 2556-2562.
14.
Dulguerov P, Calcaterra T. Esthesioneuroblastoma: The UCLA experience 1970-1990. Laryngoscope 1992; 102: 843-849.
15.
Eriksen JG, Bastholt L, Krogdahl AS, et al. Estnesioneuroblastoma - what is the optimal treatment? Acta Oncol 2000; 39: 231-235.
16.
Hwang SK, Paek SH, Kim DG, et al. Olfactory neuroblastomas. Neurooncol 2002; 59(3): 217-226.
17.
Iliades T, Printza A, Eleftheriades N, et al. Olfactory Neuroblastomas. A Report of 3 Cases. ORL J Otorhinolaryngol Relat Spec 2002; 64(6): 454-456.
18.
Kenmochi M, Ohashi T, Ochi K, et al. A rare case of Olfactory Neuroblastoma with intracranial extension. Auris Nasus Larynx 2003; 30: 111-114.
19.
Lund VJ, Howard D, Wei W. Olfactory Neuroblastoma: Past, Present, and Future? Laryngoscope 2003; 113(3): 502-507.
20.
Zou L, Cheng Q. The Experience of treatment of 7 cases of Olfactory Neuroblastoma. Lin Chuang Er Bi Yan Hou Ke Za Zhi 1999; 13(2): 60-61.