Objective: To evaluate the efficacy of non-enhanced helical computed tomography scan in patients with acute right lower quadrant pain and diagnosing acute appendicitis.
Method: A total number of 70 patients presented with right lower quadrant pain, suspected to have appendicitis were referred by emergency and surgical departments for a non-enhanced helical computed tomography scan. The primary computed tomography criteria for diagnosing acute appendicitis were a distended appendix greater than 6 mm in maximal diameter, appendiceal wall thickening, and free peritoneal fluid. Prospective diagnoses based on computed tomography findings were compared with surgical results and clinical follow-up.
Results: Acute appendicitis was diagnosed in 30 of the 70 patients (43%). Of the 30 patients with a computed tomography diagnosis of acute appendicitis, 27 (39%) had acute appendicitis proven by surgery and pathology. Twenty-two (31%) patients had a normal computed tomography study and 18 (26%) patients had non-appendiceal pathologies. There were 27 true-positives, 38 true negatives, 3 false positives, and 2 false negatives. Non-contrast helical computed tomography had a sensitivity of 90%, specificity of 95%, and accuracy of 95%.
Conclusion: This study shows that non-enhanced Computed tomography is a useful test to diagnose appendicitis in patients with acute abdominal pain in the right lower quadrant.
Key words: Right lower quadrant pain, Computed tomography scan, Appendicitis.
JRMS Dec 2006; 13(2):20-23
IntroductionComputed tomography (CT) scan has emerged as a powerful diagnostic tool in the evaluation of suspected appendicitis, and its routine use has been advocated. A landmark study revealed that CT scan was far more sensitive and specific than the pre-CT linical diagnosis (1). Accuracy rates with a variety of CT techniques that used different combinations of oral, rectal, and intravenous contrast agents have ranged form 93% to 98% for patients suspected to have acute appendicitis (2).
In 20% of patients with appendicitis, the diagnosis is missed initially, and in 15 to 40% of those undergoing emergency operations for suspected appendicitis, the appendix is normal (3,4). Clearly, more precision in the diagnosis is essential. Such precision can be achieved with laparoscopy, but it has the disadvantage of being invasive and not entirely free of risks. Of the noninvasive diagnostic aids, ultrasonography was for some time the most promising, but CT san has proved to be more precise (3).
Elimination of the delay and risk of administering contrast material allows thin-section helical CT performed without oral, rectal, or intravenous administration of contrast material to be ideally suited for the evaluation of patients with suspected acute appendicitis. Also, the ability to accurately diagnose acute appendicitis and the myriad of disorders that clinically mimic it should reduce the number of unnecessary appendectomies (2). Our study aimed to establish non-enhanced helical CT technique to diagnose accurately acute appendicitis and that condition that can mimic it.
Methods
Seventy consecutive patients were examined prospectively by using transverse non-enhanced thin section helical CT for the detection of suspected acute appendicitis. The patients included 33 males (47%) and 37 females (53%) who were referred from surgical and emergency departments at Prince Ali and Prince Hashem hospitals between August 2003 and August 2004. Age range was 14-76 years. Inclusion criteria were based on the clinical judgment of the referring physicians.
All CT scans were obtained with a Hi Speed dual helical CT scanner from GE. A single breath-hold helical scans from the top of the T12 vertebral body to the pubic symphysis was obtained by using 5mm beam collimation and 8mm/sec table speed (pitch 1.6; 120kVp; 240-270mAs). No oral, rectal, or intravenous contrast material was administered. Images were reconstructed and photographed at 5mm intervals by using standard soft tissue windows (width 400 HU; level, 40 HU). Patients were instructed to hold their breath on inspiration for 45 seconds. Total examination time was approximately 10 minutes.
The primary CT criteria for diagnosing acute appendicitis were a distended appendix greater than 6 mm in maximal diameter, appendiceal wall thickening, and free peritoneal fluid. The presence of periappendicular stranding, focal thickening of the apex of the cecum, and visualization of appendicoliths were also noted prospectively. Following completion of the examination, the CT images were immediately reviewed by a specialist radiologist. The CT findings were compared with the surgical and pathologic findings. If surgery was not performed, then clinical follow-up was conducted in all patients. Appendectomy was not performed at a later date in any of the patients who had CT scans that were interpreted as negative.
Results
The prospective interpretations of the non-enhanced helical CT scans in the 70 patients yielded 27 (39%) true-positive and 38(54%) true-negative diagnoses. For 18 (47%) of the 38 true-negative CT interpretations, an alternative diagnosis was correctly established prospectively.
There were three false-positive interpretations and two false-negative interpretations. In the first and second false-positive examinations, the appendix measured greater than 6 mm in transverse diameter: 7 and 10 mm. Within the 10-mm appendix, an appendicolith was also clearly evident. However, on retrospective review, periappendiceal inflammation was not present on either of the two CT scans. In the third false-positive case, the base of the appendix measured 7 mm on CT scans, with minimal periappendiceal inflammation. However, it was histologically normal. The two patients with false-negative interpretations were encountered very early in our study protocol and, in retrospect, had obviously positive diagnosis of acute appendicitis.
In 18 (26%) of the 70 patients imaged prospectively for acute appendicitis, an alternative diagnosis was correctly established on the basis of surgical or clinical follow-up, or the additional imaging findings. Disease entities in these 18 patients included renal or ureteral calculi in 6, gynecologic disorders in 4, small-bowel disease in two, mesenteric adenitis in three, and neoplasms in one. Miscellaneous disorders included cholelithiasis and bladder inguinal hernia. This analysis corresponds to an overall sensitivity of 90%, a specificity of 95%, and an accuracy of 95%. The positive predictive value was 93%, and the negative predictive value was 93%.
DiscussionAppendicitis is an acute inflammation of the appendix. The appendix is a blind-ending diverticular structure arising from the cecum. Acute appendicitis is a common cause of abdominal pain and the most frequent condition leading to emergent abdominal surgery in children (5).
Despite the familiarity of signs and symptoms of disease, 20% of patients present atypically (6). Atypical clinical presentations can occur in patients with a retrocecal appendix, with flank or right upper quadrant pain, or in patients with bowel malrotation or elongated appendix within the pelvis or inguinal canal. Clinical diagnosis is more problematic in infants and young children; ovulating women aged 20-40 years, and elderly patients. Controversy exists as to whether imaging is required in patients with the classic history and physical findings of acute appendicitis. Opinions vary as to whether these modalities should be performed in all patients with suggested appendicitis or if radiology should be reserved for selected patients with atypical or confusing clinical presentations (6,7).
Several authors have emphasized the value of focused appendiceal imaging. The use of contiguous thin-section helical scanning limited to the right lower quadrant (RLQ), with or without rectal contrast material, is used in a selected population reportedly results in an extremely high rate (up to 100%) of visualization of the appendix and is 98% accurate for the diagnosis of acute appendicitis, which is little higher than accuracy rate in our study (95%), but still somewhat better than the accuracy rates of nonfocused appendiceal imaging techniques reported in the literature (93%) (8,9).
Nevertheless, limitation of the diagnostic study to the RLQ and visualization of the appendix may not always facilitate a diagnosis, moreover the ability to scan the abdomen and pelvis rapidly without any bowel preparation or contrast medium has made non-enhanced helical CT the study of choice for the evaluation of patients suspected to have acute appendicitis. Furthermore, since rectal, oral, and intravenous contrast materials are not used, other imaging studies are not precluded if no abnormality is detected on the non-enhanced CT scan. The examination is not operator-dependent and may be performed in very ill patients (2,9).
In our study the primary imaging findings of acute appendicitis at non-enhanced CT include an appendix that measures greater than 6 mm in transverse diameter and periappendiceal inflammation (2,4,10) (Fig. 1).
Additional findings on CT scans in acute appendicitis include cecal or appendiceal wall thickening, appendicoliths, and periappendiceal fluid collections. Visualization of an appendicolith may aid in identifying the appendix, although this finding is not specific for acute appendicitis (4,10) (Fig. 2 & 3). Intraperitoneal fat is the intrinsic contrast medium of a non-enhanced CT examination. Identifying inflammatory changes in thin pediatric patients with little intraperitoneal fat may therefore be difficult (2).
In our study the two false-negative interpretations that occurred were in thin, young women with little intraperitoneal fat, the lack of intraperitoneal fat in these two patients resulted in obscuration of the inflammatory process in the periappendiceal fat, even though the appendix was visualized prospectively.
We consider non-enhanced helical CT to be the initial study of choice for confirmation of suspected appendicitis in adult patients with normal or obese body habitus. Ultrasound (US) remains the primary imaging modality for pediatric patients, pregnant patients, and very thin patients of either sex with suspected acute appendicitis (11). Use of this rapid, non–operator-dependent and, in our experience, highly accurate examination may decrease delays in appropriate medical or surgical therapy.
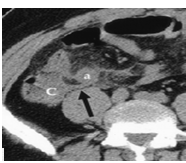
Fig. 1: Non-enhanced transverse helical CT scan in a 38-year-old woman with right lower quadrant pain and fever shows a dilated appendix (a) in the transverse orientation, with associated periappendiceal inflammation adjacent to the cecum (c). Note the thickened appendiceal mesocolon (arrow).
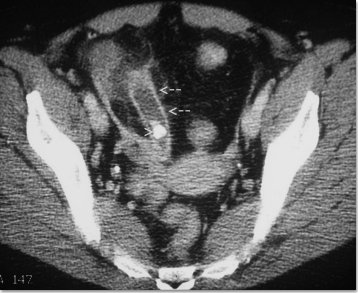 Fig. 2:
Fig. 2: Appendicitis (inflamed distended pus-filled appendix, arrows) with calcified appendicolith (arrowhead) on CT in an adult.
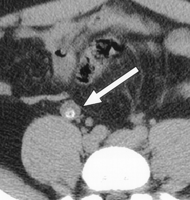 Fig. 3:
Fig. 3: Non-enhanced transverse helical CT scan in a 31-year-old man with pelvic pain radiating to the umbilicus shows a dilated appendix (arrow) containing an appendicolith. There is no periappendiceal inflammation.
This result was prospectively interpreted as acute appendicitis; however, no evidence for acute appendicitis was identified at histologic examination
Conclusion Non-enhanced CT is a useful test to diagnose appendicitis in patients with acute abdominal pain in the right lower quadrant however; the interpreter must be aware of the broad range of abnormalities that may mimic a very common disorder. In our study, the appendix was visualized by non-enhanced CT scan in all patients, the test was considered negative when the criteria did not meet the diagnosis of acute appendicitis including appendix diameter of less than 6 mm, normal appendiceal wall thickening and normal periappendicular fat planes.
Currently we recommend non-enhanced spiral CT scan for all candidate patents with acute right iliac fossa pain and no laparatomies should be done without performing the test. Moreover, accurately diagnosing those conditions that can mimic acute appendicitis, a very common disorder, may help reduce the number of unnecessary appendectomies.
References1.
Murray S. CT for Acute Abdomen Pain (Appendicitis and Kidney Stone) (Serial online) 2003. Available from: URL:
http://www.rasloimaging.com.Newsletter/Oct2003.pdf
2.
Lane M, Liu D, Huynh M, et al. Suspected Acute Appendicitis: Nonenhanced Helical CT in 300 Consecutive Patients. Radiology 1999; 213: 341-346.
3.
McColl I. More precision in diagnosing appendicitis. N Engl J Med 1998; 338(3): 190-191.
4.
Mann J. The rational use of a CT scan in the diagnosis of appendicitis (Serial online) 2003. Available from: URL: http:// www.homestead.com/emguidemaps/files/ctscaninappendicitis-two.htm
5.
Tucker J. Appendicitis (Serial online) 2004. Available from: URL: http://www.emedicine.com/pedtopic127.htm
6.
Incesu L. Appendicitis (Serial online) 2004. Available online: URL:
http://www.emedicine.com/radiotopic47.htm
7.
Ng C, Watson C, Palmer C, et al. Evaluation of early abdominopelvic computed tomography in patients with acute abdominal pain of unknown cause: Prospective randomised study. BMJ 2002; 325:1387.
8.
Barbara M, Pena G, Taylor G, et al. Effect of computed tomography on patient management and costs in children with suspected appendicitis. Pediatrics 1999; 104: 440-446.
9.
Kemel I, Goldberg N, Keogan M, et al. Right lower quadrant pain and suspected appendicitis: Nonfocused appendiceal review of 100 cases. Radiology 2000; 217:159-163.
10.
Rosen M. CT exerts influence on patient management, from surgical decisions to hospital stays (Serial online) 2003. Available from: URL:
http://www.dimag.com/advancedct2003.htm
11.
Douglas C, Macpherson N, Davidson P, et al. Randomised controlled trial of ultrasonography in diagnosis of acute appendicitis, incorporating the Alvarado score. BMJ 2000; 321: 919-920.