Objective: To investigate the distribution of granulomas of the jaws and the oral cavity and to evaluate the clinical and radiological data contained in the submitted histopathology request forms in a peripheral hospital in the North of Jordan.
Methods: All the patients who had been treated surgically for oral granulomas at Prince Rashid Bin Al-Hassan hospital during the period 1984-2002 were included in this study. Histopathology records for those patients were retrospectively analyzed for the following data: Age, gender, presentation of the lesion, site distribution, and adequacy of the clinical data provided in the histopathology records.
Results: During the study period, 62 patients received surgical treatment by excision and / or curettage for oral granulomas. The majority of granulomas were found in females 34 (54.8%) compared to males 28 (45.2 %). Twenty-four cases (38.7%) were in the mandible and 23 cases (37.1%) in the maxilla. The highest percentage of granulomas (38.7%) was found in the young patients within the age group of 10-20 years. Pyogenic granulomas were the most encountered type in 29 cases (46.8 %), followed by peripheral giant cell granulomas, 22 (35.5 %). The chief complaint at presentation was friable mass in 38.7 % of the patients, followed by swelling and firm mass in 33.9% and 27.4% of the patients respectively.
Conclusion: Oral granulomas are more common in the jawbones than other sites of the oral cavity. These lesions are benign and rarely recur if properly treated. Pyogenic granuloma is the most encountered type, and central giant cell granuloma showed the highest recurrence. All the possible personal, clinical, and radiological data should be provided in the histopathology request forms, to provide better categorization of these lesions and to help better follow up.
Key words: Granuloma, Reparative, Giant Cells, Pyogenic.
JRMS Dec 2006; 13(2):41-45 Introduction Pyogenic granuloma is a non neoplastic tumor-like growth of the oral cavity which was originally thought to be caused by pyogenic organisms, it is now believed to be unrelated to infections but represent an exuberant tissue response to local irritation or trauma, in spite of its name it is not a true granuloma (1).
Giant cell granulomas are either central or peripheral. Central giant cell granulomas occur within jaw bones and may initially present as a solitary cyst like radiolucency but as it grows larger it frequently develops an architecture that causes a soap bubble appearance radiolucency, it tends to occur more in females than in males. Peripheral giant cell granuloma occurs as an exophytic lesion exclusively on the gingival and alveolar mucosa, it also affects females more than males. The exact etiology of oral granulomas is not well identified and trauma plays an important role.
Oral granulomas are treated surgically by excision and curettage (2); their recurrence should alert the clinician to the possibility of parathyroid disease. The aim of this study was to investigate the distribution of the different types of oral granulomas and to evaluate the clinical and radiological data contained in the submitted histopathology request forms.
MethodsAll patients who had been treated surgically for oral granulomas at Prince Rashid Bin Al-Hassan Hospital over a period of 18 years (1984-2002) were included in this study. The excised specimens were sent to the histopathology laboratory with written histopathology request forms containing demographic, clinical, and radiological data. Histopathology records of the patients were retrospectively analyzed for the following data, age, gender, and presentation of the lesion in addition to site distribution and adequacy of the clinical data provided in the histopathology records.
These data were tabulated and statistically analyzed using the SPSS program standard version release 9.0 using the chi square test.
Results
A total of 62 granulomas were surgically treated during the study period. The majority of the granulomas occurred in females 34 (54.8 %) compared to males 28 (45.2%).
The age of the patients ranged from 6-70 years (mean 38 years). Most of the granulomas 46.8% occurred in the young age group (10-20 years) followed by the age group (41-60 years) in 24.2 % of the cases; the distribution of the cases among the different age groups is presented in (Fig 1). In 16 cases (25.8%) the duration of the lesion is not mentioned in the histopathology request forms, and in 54 cases (87.1%) no description of the radiological appearance of the lesion was provided in the histopathology request forms.
The number of granulomas found in the mandible was 24 (38.7%), nearly equal to those in the maxilla 23 (37.1%), the remaining granulomas were found in the lower lip, cheek, upper lip, and the tongue respectively (Fig 2). In 24 of the cases (38.7%), the exact location of the granuloma in the upper or lower jaw was not mentioned.
The results of histopathology revealed that pyogenic granulomas accounted for 46.8% of the cases, followed the peripheral giant cell granulomas (35.5%), while central giant cell granulomas was found only in 8% of the cases, The group of the granulomas designated as giant cell granulomas was found in 9.7% of the cases (Fig 3).
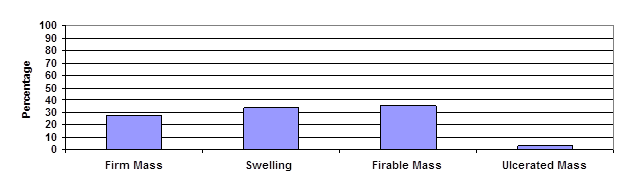
The highest percentage of the granulomas (35.5%) presented clinically as a friable mass, followed by swelling (33.9%), and the least clinical presentation was an ulcerated mass in (3.2%) of the case as demonstrated in (Fig 4).
Sixty of the granulomas (96.8%) were sent for histopathology as excisional biopsies and only two specimens were sent as incisional biopsies. Six specimens (9.7%) were containing bone or teeth, the remaining specimens were only soft tissues.
Among the 62 cases, the ability of the clinician to diagnose or expect the lesion as granuloma depending only on clinical and/or radiological features was correct in 40 cases (64.5%), while the ability of the clinician to expect the exact kind of granuloma clinically was correct in 19 cases (30.6%). The highest precision of expectation was with pyogenic granulomas 15 (24.2%). The overall ability of the clinician to predict or exclude the exact diagnosis of granuloma clinically was significant (P < 0.03).
In 16 cases (25.8%) the duration of the lesion is not mentioned in the histopathology request forms, and in 54 cases (87.1%) no description of the radiological appearance of the lesion was provided in the histopathology request forms.
The histopathologist commented on 11 cases as incompletely excised and asked for evaluation of the parathyroid diseases in three cases, two of them turned to have parathyroid adenomas (hyperparathyroidism). In 4 cases, the final histopathology diagnosis referred to the reparative nature of the granuloma and no reference was mentioned regarding giant cell tumors.
Discussion
This study showed that oral granulomas occur in females more than males, in a ratio of 1.2:1, this corroborates with other studies (3,4). The age group less than 20 years was the most affected, where 38.7% of the granulomas occurred in this age group. Mandible was affected more than the maxilla, however, both jaws hosted 65.8% of the cases, the second site most affected was the lower lip, and the least affected site was the tongue.
Pyogenic granulomas constituted 46.8% of the oral granulomas and again females slightly outnumbered males, the pyogenic granuloma is a relatively common, tumor like, exuberant tissue response to localized irritation or trauma. The name pyogenic granuloma is a misnomer since the condition is not associated with pus and does not represent a granuloma histologically.
It is a reactive inflammatory process filled with proliferating vascular channels, immature fibroblastic connective tissue, and scattered inflammatory cells. The surface is usually ulcerated, and the lesion exhibits a lobular architecture (4).
Two lesions, peripheral ossifying fibroma and peripheral giant cell granuloma, are clinically identical to the pyogenic granuloma when they occur on the gingiva. If 100 biopsies of pyogenic granuloma appearing lesions of the gingiva are submitted for histopathological examination, approximately 85% will be pyogenic granulomas, 10% will be peripheral ossifying fibromas, and 5% will be peripheral giant cell granulomas. The clinical appearance, treatment, and prognosis are the same for all three entities (5).
In this study there were no exact descriptions in histopathology request forms of the color of the lesions who turned to be pyogenic or peripheral giant cell granulomas, the clinician either did not think that was necessary and it would not have changed the microscopic appearance or just overlooked that important differentiating feature of granulomas.
Peripheral giant cell granulomas also known as giant-cell epulis, osteoclastoma, giant-cell reparative granuloma, or giant-cell hyperplasia (6) occur exclusively on the gingiva or edentulous alveolar ridges, its clinical appearance is similar to pyogenic granuloma but its color is bluish purple compared to the bright red color of atypical pyogenic granuloma.
Central giant cell granuloma appears to be a unique lesion of the jaws, although the so-called giant cell reaction of the hands and feet shares many features (7). The radiographic features of central giant cell granuloma vary; early lesions are usually small, unilocular areas of lucency that can mimic an odontogenic cyst. As it develops, the lesion may appear multilocular with wispy internal septa and osseous expansion (8). The main histologic differential diagnosis includes the brown tumor of hyperparathyroidism and the giant-cell tumor of bone.
The brown tumor of hyperparathyroidism has histological features identical to those of giant-cell reparative granuloma. The giant-cell tumor of bone is distinguished from this lesion by having a more diffuse and homogeneous distribution of giant cells and by subtle morphologic differences in the stromal cells (9).
In spite of these similarities, jaw lesions appear to have different biological behavior like high recurrence rates and up to 10% show malignant changes; Whitaker (10) reported an over all recurrence rate of 16% of the 147 studied cases of central giant cell granulomas. Surgery is the treatment currently recommended for oral granulomas, Alternative treatment of giant cell granulomas involve steroid injection in cases of progressive and recurrent lesions, calcification and shrinkage of these lesions occurred following intralesional steroid injections (11,12).
In this study, no periapical granulomas were reported, probably due to the fact that small granulomas attached to the apex of extracted teeth or teeth roots are not usually submitted to histopathology examination and considered innocent, and these granulomas removed during apical surgery are fragmented and usually discarded, however periapical granulomas provided to the histopathologist without the teeth or teeth roots or without mentioning their relationship to the teeth in the histology request could have been diagnosed as pyogenic granulomas.
Another group of granulomas were designated as giant cell granulomas without mentioning whether they were central or peripheral due to the lack of detailed clinical and radiological data provided in the histopathology request forms. Essential clinical data related to the duration of illness, relationship of the lesion to dental structures, radiological appearance, and the operative findings are overlooked and not provided in the histopathology request forms, this could be explained but not justified by the fact of relative easiness of diagnosing a granuloma clinically and the clinician was interested mainly in excluding malignant changes in these lesions rather than sub-classifying every granuloma into a certain group.
Colleagues at histopathology departments still referring to the reparative nature of some granulomas although the reparative process of oral granulomas is doubtful, better communication with the histopathologist is usually achieved through the provision of all the relevant clinical and radiological data with the submitted specimens.
Conclusion
Oral granulomas are benign tumors that rarely recur if properly treated, these tumors are more common in the jawbones than other sites of the oral cavity. All the possible personal, clinical, and radiological data should be provided in the histopathology request forms, this will help the histopathologist to better diagnose and classify granulomas and this will help the clinician to schedule treatment and follow up.
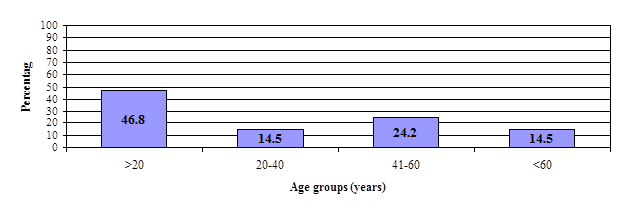 Fig. 1:
Fig. 1: Distribution of granulomas among age groups.
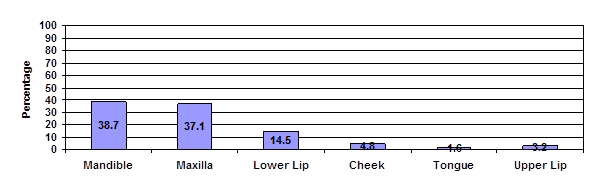 Fig. 2:
Fig. 2: Site distribution of granulomas
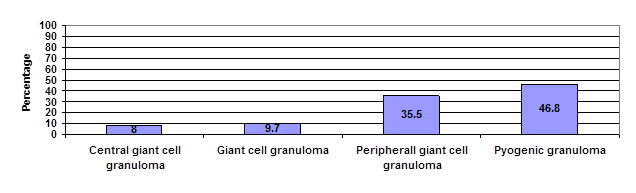
Fig. 3: Types of granulomas among study groups as appeared in the request forms