ABSTRACT
Objective: To assess the outcome of infragenicular arterial revascularization for lower limb salvage in critical ischemia.
Methods: A retrospective analysis was conducted on 33 patients who underwent infragenicular bypass procedure for critical limb ischemia at Queen Alia Military Hospital / Vascular Unit between the years 2002 and 2004. Twenty seven patients were males and 6 were females with a mean age of 63 years. Rest pain and gangrene were the presentation in most of the patients. Twenty two patients were diabetics. Long saphenous vein was used for the bypass in 28 patients. Analysis of the graft patency, limb salvage and patient survival was considered.
Results: The early patency rate within the first 30 days was 64%. At 12 and 24 months, the patency was 47% and 39% and the limb salvage rate was 51% and 45%, respectively. A total of 14 major limb amputations has been performed, 8 of which were at above knee level. Three cases of death within the first 6 months were reported due to acute myocardial infarction.
Conclusion: Reconstructive procedure should be attempted before considering major limb amputation as long as there is an opportunity of saving a critically ischemic limb.
Infragenicular revascularization to the tibial and pedal arteries is an effective procedure in limb salvage and improving the quality of patient’s life.
Key words: Infragenicular bypass, Limb salvage, Patency, Amputation.
JRMS April 2007; 14(1): 13-16Introduction
The elderly patient with critical limb ischemia remains a challenge to the vascular surgeon(1).
Critical limb ischemia can be defined as the ischemia that endangers the whole or part of a leg and presents clinically by rest pain requiring analgesia for more than two weeks, ulceration or gangrene at the foot(2). It is usually characterized by accelerated and extensive multilevel and distal occlusive disease of the infra inguinal vessels and requires distal revascularization to ensure tissue healing and relief of disabling symptoms(2-5).
Results of revascularization surgery have been improving lately and the treatment of critical limb ischemia has promptly involved the distal bypass to vessels beyond the popliteal artery trifurcation which leads to improving limb salvage in patients at risk of losing their legs(5-7).
We reviewed the feasibility of infragenicular bypass in critical limb ischemia salvage in terms of graft patency, limb salvage and patient survival.
Methods
A retrospective review of the records of patients who underwent infragenicular distal bypass procedures for critical limb ischemia between January 2002 and 2004 held at the vascular unit at Queen Alia Military Hospital was carried out.
There were 33 patients in the study, twenty seven (82%) were males while 6 (18%) were females. Their mean age was 63 years (range 30 – 82).
Rest pain was the presentation in 10 patients (30%) while 13 patients (40%) presented with dry gangrene, 5 patients (15%) with wet gangrene and 5 patients (15%) with ulceration.
Diabetes mellitus was reported in 22 patients (67%), smoking in 19 patients (58%) and hypertension in 16 patients (48 %) (Table I).
Table I: Risk factors and associated diseases in the reviewed patients.
|
Disease
|
Number of patients ( % )
|
|
Diabetes
Mellitus
|
22 (67 )
|
|
Smoking
|
19 (58)
|
|
Hypertension
|
16 (48)
|
|
Coronary
Disease
|
10 (30)
|
|
Hyperlipidaemia
|
9 (27)
|
|
Stroke
|
2 (6)
|
|
Renal
Failure
|
2 (6)
|
Preoperative evaluation of both the inflow and outflow vessels, the type of revascularization to be used as well as the quality of lower limb superficial veins was achieved by Duplex ultrasound and arteriography (Fig. 1).
In 25 patients (75%), the common femoral artery provided the inflow whereas the superficial femoral artery was the source in 3 patients (9%) and the popliteal artery in 5 patients (15%) (Fig. 2.) (Table II).
Table II: Inflow and out flow vessels.
|
Inflow
source
|
Run off
Vessels
|
|
Common
femoral artery
|
25
|
Posterior tibial artery
|
19
|
|
Popliteal
artery
|
5
|
Anterior tibial artery
|
11
|
|
Superficial
femoral artery
|
3
|
Peroneal artery
|
3
|
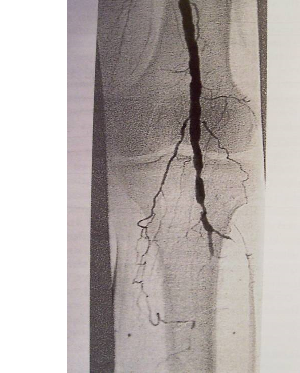
Fig. 1: Pre operative lower limb angiographic findings showing severe infragenicular arterial diseases.

Fig. 2: Clinical findings to show the scars in right thigh over common femoral artery (inflow) and over the harvested long saphenous vein.
Associated arterial surgery such as iliac angioplasty in 3 patients and common femoral artery endarterectomy in 5 patients were necessary to perform to improve the quality of the inflow stream.
Although the posterior tibial artery constituted the runoff vessel in 19 patients (58%) , the anterior tibial artery and the peroneal artery were used as the outflow vessels in 11 patients (33%) and 3 patients (9%) respectively (Fig. 3).
 Fig. 3:
Fig. 3: Clinical outcome of left lower limb following distal bypass to posterior tibial artery using long saphenous vein.
Reversed long saphenous vein was used for the bypass graft in 28 patients (85%). A composite graft of saphenous vein and polytetrafluoroethylene (PTFE) graft was used in 4 patients (12%) and prosthetic PTFE graft with a vein cuff in one patient (3 %).
Statistical analysis of the results of limb salvage, graft patency and survival rate over the time period was discussed.
Results
Patients were followed up post operatively with non invasive tests including clinical evaluation of the pedal pulse status and Ankle Brachial Pressure Index with Duplex ultrasonography before the discharge from hospital and with intervals of 30 days, 3,6,12 and 24 months, respectively.
The early patency rate ( within 30 days )of distal bypass was 64 % mostly due to graft occlusion and poor run off vessels with 5 amputations carried out in the first post operative week ;two of them were at above knee level. One bypass was complicated by early post operative death (third day) due to acute myocardial infarction while 2 patients had minor wound complications such as hematoma.
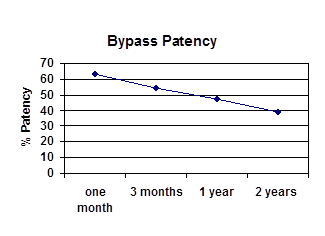
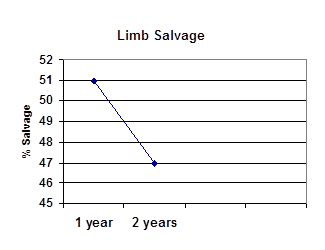
At 3 months 54 % of the remained functioning bypasses were still patent, 47 % at one year and 39 % at 2 years. The limb salvage rate was 51 % at one year and 45 % at 2 years. (Graph. 1 and 2).
 Graph. 1:
Graph. 1: Bypass patency rate
 Graph. 2:
Graph. 2: Limb salvage rate.
The total number of amputations performed was 14(42%); eight cases performed above knee, 5 cases below knee and one case of below knee was converted to above knee amputation. Two patients with late graft failure did not require amputation and intravenous anticoagulation and later anti platelets were administered.
Two extra death cases were reported in the study within the first 6 months post operatively that were diagnosed as acute myocardial ischemia.
Discussion
Revascularization is the gold standard treatment for ischemic limb salvage. It provides adequate vascularity for the eradication of sepsis, removal of all inevitably damaged tissues and creation of a functional limb as the ultimate goal of the limb salvage procedure(3,8,9).
Relatively high rates of early graft failure and subsequent amputation, in our study, in comparison with others were related to poor candidate status: poor inflow and run off vessels status, advanced infection of the foot and irreversible ischemia of the distal soft tissues, and the poor quality and length of the vein grafts(1,10,11). The late failures, however, were mainly due to intimal hyperplasia at the sites of anastomosis and the progression of the atherosclerotic disease in the native vessels nearby both ends of the conduit.
Proper selection of a good inflow to be bypassed to a patent non resistant arterial outflow to achieve a distal pulsatile blood flow and optimal tissue oxygenation constitutes the basic requirements of the operation(3,4). Initial pre operative evaluation of these arteries was done with Duplex ultrasound in all the patients and the arteriography in most of them to demonstrate the infra popliteal circulation including foot vessels.
As recommended by others, reconstruction procedures to improve the inflow were performed in some patients with percutaneous transluminal angioplasty and localized endarterectomy(4) .
Among the grafts used for our patients, reversed long saphenous vein harvested from the same leg were the majority of the grafts with a rate of 85% (28 patients). Autologous vein graft is recommended as it provides a better patency rate and is more resistant to infection compatible with the reports by other authors(1,6,10,11). We also implemented a composite graft with PTFE or PTFE graft alone with a vein cuff when the vein is inadequate or unavailable for the bypass to improve the patency rate as recommended by others(6,11).
Our results in the limb salvage rate are slightly inferior to others(1,4,6,10,12).This is due to various factors including: the delayed care by the late presentation of patients to the clinic, ignorance of the risk factors and the lack of medical insurance. We believe that to improve outcome, better understanding and awareness of the nature of the disease by patients, better control of the risk factors, better referral system and the multidisciplinary team approach by cardiologist, vascular surgeon, anesthetist, podiatrist and physiotherapist are mandated.
More than half of our patients for the distal revascularization were diabetics showing similarity to others' study findings(1,3,5,7). This is probably related to the specific nature of the ischemic angiopathy of diabetes mellitus with its unique distribution pattern affecting infragenicular arterial tree sparing the foot arteries. Medial arterial calcinosis leading to non compressible arteries and more likelihood of development of critical limb ischemia often mandate further distal bypass even to the pedal arterial level(2,3,7,13,14).
Following successful revascularization, secondary procedures were often required for foot salvage including wound debridement, minor amputations with or without flap application(1,8). These approaches improved the functional outcome parameters, the quality of life and the patient satisfaction among our patients; they became more independent in daily activities and improved in walking capabilities besides helping in the long term success of the distal bypass surgery. Fig. 4.

Fig. 4: Clinical findings of initial debridement and minor amputations as the secondary procedures to improve the outcome of limb salvage procedures.
Conclusion
A reconstructive surgery should be considered before a major limb amputation is warranted, as long as there is a chance of saving the limb in critical ischemia. Distal revascularization to tibial and pedal arteries is a feasible option for the limb salvage and to improving quality of life.
References
1.
Frankini AD, Pezzella MVC. Foot revascularization in patients with critical limb ischemia. J .Vasc Br 2002; 1(3): 193-200.
2.
Santilli JD, Santilli SM. Chronic limb ischemia: Diagnosis, treatment and prognosis. American Family Physician 1999; 59(7): 25-32.
3.
Damme HV. Crural or pedal artery revascularization for limb salvage: Is it justified? Acta Chir belg 2004; 104: 148-157.
4.
Zukauskas G, Ulevicius H. Simultaneous versus two stage multisegmental reconstruction for critical lower limb ischemia. Ann Saudi Med 1995; 15(4): 48-54.
5.
Wolosker N, Neto BM, Munia MA, et al. External aggression to the limb as a predictive factor in the evolution of patients undergoing arterial revascularization. Clinics 2005; 60(6): 36-40.
6.
Stonebridge PA, Naidu S, Colgan MP, et al. Tibial and peroneal artery bypasses using polytetrafluorethylene (PTFE) with an interposition vein cuff. J R Coll Surg Edinb 2000; 45: 17-20.
7.
Ionac M, Pascut M, Slovenschi M, Bordos D. Microscope aided femoral- or popliteal – to – distal bypass for salvage of limbs with critical ischemia. Romanian Journal of Hand and Reconstruction Microsurgery 1999; 4(2): 68-73.
8.
Luther M, lepantaio M, Alback A, Matzke S. Amputation rates as a measure of vascular surgical results. Br J of Surgery 1996; 83: 241-244.
9.
Panayiotopoulos YP, Tyrrell MR, Owen EE, et al. Outcome and cost analysis after femorocrural and femoropedal grafting for critical limb ischemia. Br J of Surgery 1997; 84(2): 207-212.
10.
Bhagavan NK, Vivekanand, Raghunandan ML, et al. Infra inguinal bypass procedure for ischemia in the lower limb. Bombay Hospital Journal 2001; 43(4): 53-58.
11.
Murphy GJ, Kipgen D, Dennis MJS, Sayers RD. An aggressive policy of bilateral saphenous vein harvest for infragenicular revascularization in the era of multidrug resistant bacteria. Post graduate Medical Journal 2002; 78: 339-343.
12.
Golledge J, Iannos J, Walsh JA, et al. Critical assessment of the outcome of infra inguinal vein bypass. Annals of Surgery 2001; 234(5): 697-701.
13.
Bizzini PG, Depairon M, Von Segresser L, Hayoz D. Vascular surveillance after peripheral artery interventions. Schweiz Med Wochenschr 1999; 129 : 413-419.
14.
Ahchong AHK, Chiu KM, Wong MWChun, et al. Diabetes and the outcome of infra inguinal bypass for critical limb ischemia. ANZ Journal of Surgery 2004; 74(3): 129-133.