Objective: To
evaluate the anti-tussive effect of brompheniramine maleate a
non-selective, sedative antihistamine using capsaicin challenge.
Methods:
Twelve subjects, five females and seven females, mean age 32 years with
a range of (23-39) years, were studied on two occasions. On the two
visits a baseline capsaicin dose-response was performed to determine C5
(the lowest concentration causing 5 coughs). After 30 minutes two C5
doses of capsaicin were given and the total cough over one minute was
counted. On the first visit Brompheniramine 8mg or a matched placebo
was given orally, and 120, 240 minutes after administration, two C5
doses of capsaicin were given and the total coughs over one minute
period were counted. This was repeated exactly in the second visit
except subjects received either a placebo or active treatment; either
which they had not received on their first visit. Subjects were also
asked to quantify their drowsiness using a 100 mm visual analogue scale.
Results:
Baseline mean cough number (confidence interval) was similar on the two
study occasions 9.9 (8.2-11.7) before Brompheniramine and 9.2
(7.3-11.1) before placebo. Cough number did not differ on the two study
days at 120 and 240 min after Brompheniramine treatment: 7.7 (5.5-9.8),
7.4 (5.1-9.6) compared to 8.7 (6.4-11.0), 8.3 (6.8-9.8) after placebo.
Mean visual analogue scale (confidence interval) after Brompheniramine
was 31 (14-48) and 40 (21-60) compared to 7 (2-12) and 7 (2-12) after
Placebo at 120 and 240 min respectively (p<0.008).
Conclusion: The sedative anti histamine Brompheniramine did not affect capsaicin induced cough though it produced significant drowsiness.
Key words: Brompheniramine, Capsaicin, Cough.
JRMS April 2007; 14(1): 26-29
IntroductionCough
is the most common respiratory symptom, however there is no specific
anti tussive agent of proven efficacy(1-4). Opioids are effective anti
tussive agents but at their effective doses they also cause physical
dependence, respiratory depression, and gastrointestinal symptoms.
The
non-narcotic opiate isomer Dextromethorphan is used as anti tussive
agent but it has a sedative effect. Persistent non-productive cough can
be a major clinical problem. A selective, non-sedating anti histamine
(terfenadine) has been shown to have an effect on cough in seasonal
rhinitis without sinusitis or post nasal drip, but it had no effect on
induced cough suggesting an indirect mechanism of action on cough
reflex(5). Non-selective antihistamines are common constituents of over
the counter cough and cold remedies and they are claimed to have an
anti-tussive effect(2,3,6).
The mechanism of action of these
non-selective antihistamines is not very well understood; it was thought
to be due to their sedative effect, which can suppress most respiratory
reflexes(1). Brompheniramine maleate is a histamine H1-receptor
antagonist given by mouth for the symptomatic relief of hypersensitivity
reactions and in pruritic skin disorders. It is common ingredient of
cough and cold preparations. It may cause some adverse effects such as
sedation and antimuscarinic effects. In this study the anti-tussive
effect of brompheniramine maleate was examined using the capsaicin
challenge.
Methods
The study had the approval
of the Royal Postgraduate Medical School (RPMS) and Hammersmith Hospital
Research Ethical Committee. All the subjects gave their written
informed consent.
Verbal consent was obtained from Healthy
employed volunteers recruited from the RPMS and Hammersmith hospital.
Subjects were excluded if they were smokers, had bronchial asthma,
chronic obstructive pulmonary disease, chronic sinusitis or allergic
rhinitis, persistent cough, a clinically significant history of other
drug intake, drug or alcohol abuse, or a respiratory tract infection
within the previous eight weeks. Subjects were asked if they had taken
an investigational drug in the previous three months and they were asked
not to drive on the study days.
The study was randomized, double
blind, placebo-controlled, cross over design. 12 healthy volunteers (5
females and seven males), mean age 32 years with a range of (23-39)
years attended on two separate days with a minimum interval of two days
between the visits and a maximum interval of four weeks from the last
visit.
On the first visit the study was explained and informed
consents were obtained. After history taking and physical examination
baseline data (height, weight and lung functions) were collected.
Capsaicin cough challenge was then carried out using doubling
concentrations starting at 0.500 μM at one minute interval according to a
standard protocol(7). Subjects inhaled (starting from just below
functional residual capacity) a single breath of capsaicin from a
nebulizer attached to a breath-activated dosimeter (PK Morgan Ltd, UK).
The output and the mass median diameter of the aerosol were 5-7 μl and
3.5-4μ respectively(7).
The number of coughs in response to
each concentration (over the one minute period immediately after each
breath of capsaicin) was recorded by an experienced observer. The
challenge was stopped when the lowest concentration required to elicit
at least 5 coughs (C5) was reached. After a 30 minute delay, two C5
doses of capsaicin were then administered within 30 seconds apart and
the total coughs in the first minute following the first C5 dose
(expected to equal 10) were recorded. After further 5 minutes either
Brompheniramine 8 mg or exactly matched placebo (which was prepared at
Hammersmith Hospital pharmacy) were given orally.
Two doses (C5)
of capsaicin were then administered with cough counting, as at
baseline, at 12o and 240 minutes. At these time points subjects were
asked to quantify the degree of drowsiness they were experiencing using a
10 cm visual analogue scale (VAS), this was marked “fully alert” at one
end and “extremely sleepy” at the other. In the second visit the
procedure was repeated exactly as the first, except that subjects were
crossed over to receive either placebo or active treatment, either which
they had not received on their first visit.
ResultsThe
procedures were well tolerated by all subjects. Capsaicin produced a
reproducible cough response though individual sensitivity varied. Cough
number was expressed as mean ± confidence interval (CI).
Analysis
of variance was used to compare the differences in the two visits.
Wilcoxon rank test used to compare the number of cough and the level of
alertness VAS between treatments. Results were expressed as treatment
(active-placebo) differences (Table I).
There was no significant
difference between baseline cough number on the two study days; 9.9
before Brompheniramine and 9.2 before placebo (p=0.34). Mean total cough
in response to capsaicin after placebo pretreatment were similar at 120
and 240 minutes; (8.7, 8.3 respectively).
Though there was a
slight trend to a decrease of mean total cough after placebo treatment,
there was no significant difference between mean total cough at 240
minutes 8.3 (6.8-9.8) and baseline 9.2 (7.3-11.1) (p=0.43). Mean total
cough (CI) at 120 min on the active day of treatment was 7.7 (5.5-9.8)
compared to 9.9 (8.2-11.7) at baseline (p=0.49). Mean total cough at 240
min after Brompheniramine treatment was 7.4 (5.1-9.6) compared to 9.9
(8.2-11.7) at baseline (p=0.42).
The comparison between the two
treatment days did not show any statistically significant results at
both time points (Fig. 1). Oral Brompheniramine did not induce a
significant inhibitory effect on capsaicin-induced cough compared to
placebo. Oral Brompheniramine induced significant level of drowsiness at
120 min and 240 min following intake; mean VAS (confidence interval)
was 31 (14-48) and 40 (21-60) compared to 7 (2-12) and 7 (2-12) after
placebo at 120 and 240 min respectively (p<0.008), (Fig. 2).
DiscussionThis
study demonstrated for the first time, that oral Brompheniramine has no
statistically significant effect on capsaicin-induced cough in normal
subjects.
Rafferty et al(5) reported that the selective, non-sedative
antihistamine, terfenadine, was effective at reducing cough in seasonal
rhinitis patients without sinusitis and post-nasal drip suggesting
terfenadine may have a direct action on the sensory limb of the cough
reflex.
Studham and Fuller(8) demonstrated that terfenadine does
not reduce the cough response to inhaled capsaicin in normal volunteers
suggesting the effect of the non-selective antihistamines used over the
counter remedies and that of the terfenadine in rhinitis is probably
indirect.
The effect in rhinitis is likely to be
eitherthrough prevention of post-nasal drip, although the patients did
not report symptom or through inhibition of histamine release in the
airways in amounts that did not lead to brnchospasm.
It had been
postulated that the anti-tussive effect of the non-selective
antihistamine could be through inhibition of post-nasal drip in patients
with viral infections or through inhibitions of other receptors, such
as acetylcholine or 5-hydroxytryptamin receptors(5).
The most
likely effect of these drugs was thought to be through sedation, which
will suppress most respiratory reflexes. The hypothesis in this study
was that brompheniramine possibly by its central sedative activity might
have an inhibitory effect on the sensory afferent arm of the cough
reflex(8). Capsaicin by inhalation caused cough and is used as a
clinical measure of the sensitivity of the cough reflex.
Patients
with dry cough are hypersensitive to capsaicin. In this study
Brompheniramine had a significant drowsiness effect at both time points
of the study in comparison to the baseline as was measured by VAS.
Brompheniramine did not show a statistically significant effect on
capsaicin-induced cough in comparison to the baseline at both time
points (120 and 240 min).
The measured effect of Brompheniramine
on alertness did not reflect on cough response measured by
capsaicin challenge. The effect of Brompheniramine on capsaicin cough
challenge is comparable to that of the non-sedative antihistamine
terfendine(8). Cough is inhibited by morphine and local anesthetics but
the selective, non-sedative antihistamine terfendine was shown to have
no effect in a placebo-controlled study in normal volunteers(8).
This
study showed that the purported anti-tussive action of the
non-selective antihistamines might not be related to there sedative
effect.
Further research is needed in order to provide a better
understanding of cough reflex using the same capsaicin cough reflex
which stimulates the C-fibers or the identification of several new
mechanisms which may lead to new drugs that target the increased
sensitivity of sensory fibers resulting in exaggerated cough.
Acknowledgment Thanks
are addressed to Philip Ind, MD, Haleema Shakur, RN, John Meyers, MD,
Respiratory Division, Hammersmith Hospital, London, UK for their help
and support in conducting this work.
Table I: Cough number and alertness visual analogue scale (VAS) in mm. at different time points
|
Time points
|
Baseline
|
120 min
|
240 min
|
|
Cough
|
VAS
|
Cough
|
VAS
|
Cough
|
VAS
|
|
Brompheniramine
|
9.9
|
8.0
|
7.7
|
31
|
7.4
|
40
|
|
Placebo
|
9.2
|
6.7
|
8.7
|
7.0
|
8.3
|
7.0
|
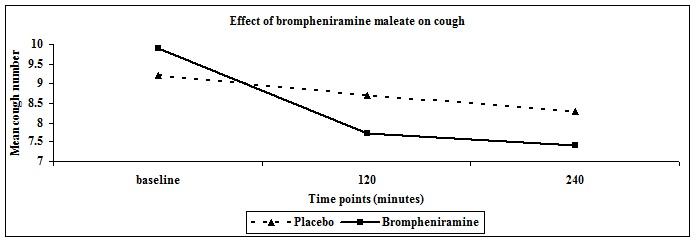 Fig. 1:
Fig. 1:Effect of brompheniramine maleate on cough.
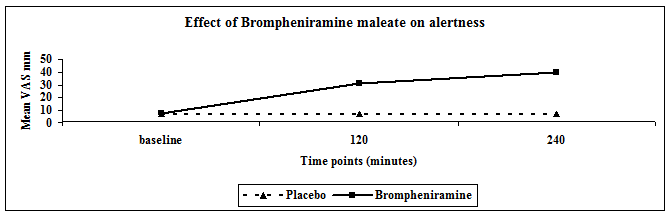 Fig. 2:
Fig. 2: Effect of brompheniramine maleate on alertness
References1.
Fuller RW, Jackson DM. Physiology and treatment of cough. Thorax 1990; 45(6): 425-430. Review.
2.
Curley FJ, Irwin RS, Pratter MR, et al. Cough and the common cold. Am Rev Respir Dis. 1988; 138(2): 305-311.
3.
Belvisi MG, Geppetti P. Cough. 7: Current and future drugs for the treatment of chronic cough. Thorax. 2004; 59(5): 438-440.
4.
Chung KF, Lalloo UG. Diagnosis and management of chronic persistent dry cough. Postgrad Med J 1996; 72(852): 594-598.
5.
Rafferty P, Jackson L, Smith R, Holgate ST.
Terfenadine, a potent histamine H1-receptor antagonist
in the treatment of grass pollen sensitive asthma. Br J Clin
Pharmacol 1990; 30(2): 229-235.
6.
Morice AH, Fontana GA, Sovijarvi AR, et al. The diagnosis and management of chronic cough. Ur Respir J 2004; 24(3): 481-492.
7.
O'Connell F, Thomas VE, Pride NB, Fuller RW. Capcaisin cough sensitivity decreases with successful treatment of chronic cough. Am J Respir Crit Care Med 1994; 150: 347-380.
8.
Studham J, Fuller W. The effect of oral terfenadine on the sensitivity of the cough reflex in normal volunteers. Pulm Pharm 1992; 5: 51-52.