A 27 year-old female was referred to the cardiology clinic at Queen Alia Heart Institute for further evaluation upon finding abnormal chest radiography, for her symptoms of reduced exercise tolerance and cough. Her chest computerized tomography showed pulmonary arteriovenous fistulae. Her cardiac catheterization confirmed the presence of bilateral lower lobe large pulmonary arteriovenous fistulae both of which were treated using transcatheter with MReye™ embolization coils.
JRMS April 2007; 14(1): 44-46IntroductionPulmonary arteriovenous fistula (PAVF) is a rare condition with well defined signs, symptoms and long-term risks.
Case Report
In 1999, during the evaluation of a 27-year old female patient for the complaint of cough chest radiography showed bilateral lower lobe lesions, and a further chest computerized tomography confirmed the presence of PAVFs. At the time further management was aborted upon the patient and family’s wish.
In 2001, the patient presented again with reduced exercise tolerance. Physical examination showed clubbing of fingers, central and peripheral cyanosis. A continuous murmur was present over the posterior region of both lower pulmonary lobes. Echocardiography revealed normal chamber dimensions, good LV function, and the absence of congenital heart defects like atrial septal defect (ASD) or ventricular septal defect (VSD).
Pulmonary artery pressure was 25mm Hg as measured by Doppler. Arterial oxygen saturation values were 85% when lying down and 89% when sitting up. The haemoglobin concentration was 17mg\dl. Her right and left heart catheterization done in June 2002 showed normal intracardiac pressures and bilateral selective pulmonary artery angiogram demonstrated large PAVFs of both lower lobes.
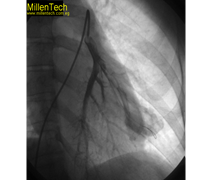
Fig. 1 A 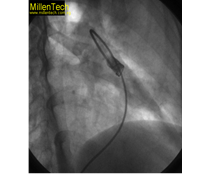 Fig. 1BFig. 1
Fig. 1BFig. 1 A. Left pulmonary arteriovenous fistula
B. Post occlusion angiogram left pulmonary
arteriovenous fistula
The left pulmonary PAVFs was selected using JR 3.0 guiding catheter (Fig. 1A), occluded with COOK,
MReye™ embolization coil 38-10-8, (Fig. 1B) and the right one (Fig. 2A ) was occluded using the same guiding catheter with COOK MReye™ embolization coil 38-8-5 (Fig. 2B).
Fig. 2 BFig. 2. A. Right pulmonary arteriovenous fistula
B. Post occlusion angiogram right pulmonary
arteriovenous fistula
Following the procedure her arterial oxygen saturation increased to 93%. Two weeks following the procedure the patient presented with pleuritic chest pain, low grade fever and mild cough. Chest radiography showed small shadowing of the right lower lobe. The diagnosis of small pulmonary infarct was presumed and treated with a combination of anticoagulants and antibiotics. Within few days her symptoms disappeared, fever subsided and her chest radiography cleared within two weeks.
In late 2004 the patient got pregnant and successfully carried her pregnancy to full term, and had an uneventful normal delivery. Her neonate was small for its gestational age but otherwise was healthy.
Discussion
PAVFs are vascular malformations that represent an intervening capillary bed. They occur with an incidence of 2-3 per 100,000 population. Females are more often affected than males(1). Multiple fistulae are found in 33-50% of patients.
Although most patients are asymptomatic, serious complications may occur and these complications can be prevented if the PAVFs are managed appropriately with Transcatheter embolotherapy (TCE). PAVFs can cause dyspnea due to right-to-left shunt, and they can also cause hemothorax. Because of paradoxical emboli, various central nervous system complications including stroke and brain abscess may occur.
Approximately 70% of the cases of PAVFs are associated with hereditary hemorrhagic telangectasia (HHT); on the other hand approximately 15-35% of patients with (HHT) have PAVFs(2-5). Currently spiral computed tomography is often the most practical method for establishing the presence of PAVFs(6). Most patients with this malformation need to be treated.
Shenstone performed the first surgical intervention(7) which was pneumonectomy for a large central lesion. This was followed by several reports of surgical procedures for PAVFs(8). TCE using metal coils or detachable balloons have been described in the literature(9). TCE can prevent many of debilitating and life threatening complications.
In experienced hands TCE is a safe and effective procedure for occlusion of PAVFs and is preferable to standard surgical therapy. TCE is currently recommended for all PAVFs with a feeding artery ≥3mm(10-12). The anatomic location of PAVFs should be carefully evaluated so as not to interrupt the arterial branches to viable lung tissue after percutaneous closure procedures. The topic of PAVFs has recently been extensively reviewed(13).
These patients can live for many years and lead a normal life. This is the first case managed in our institution with TCE. Pregnancy in the hypoxic patient is possible, but the rate of fetal loss is increased when hypoxia is corrected. The ability to conceive and have a normal pregnancy is possible.
References
1.
Puskas JD, Allen MS, Moneure AC, Wain JC. Pulmonary arteriovenous malformations: therapeutic options. Ann Thoracic Surgery 1993; 56: 253.
2.
Vase PM, Holm H. Pulmonary arteriovenous fistulas in HHT. ACTA Med Scand 1985; 218: 105-109.
3.
Hodgson CH, Burchelly HB, Good CA, Claggett OT. HHT and pulmonary arteriovenous fishula. N England J Med 1959; 261: 925-636.
4.
Haitgema TF, Dish TTC, Overtoom CJJ, et al. Screening family members of patients with HHT. Am J Med 1995; 99: 519-524.
5.
Allister KAF , Lennon B, Bowles-Bieseckey WC, et al. Genetic heterogeneity in HHT: Possible correlation with clinical phenotype. J Med Genet 1994; 31: 927-932.
6.
Pick A, Deshamps C, Stanson AW. Pulmonary arterio venous fistula: Presentation, diagnosis and treatment. World J Surg 1999; 23(11): 1118-1122.
7.
Shenston NS. Experiences with total pneumonectomy. J Thoracic Surg 1942; 11: 405.
8.
Browse PW, Renner JW. Staged bilateral thoracotomy for multiple pulmonary arterio venous malformations complicating HHT. J Thoracic Cardiovascular Surg 1982; 83: 285.
9.
Berman W, Tripp RR, Raisher BD, Yahek SN. Transcatheter occlusion of large PAVFs. Catheterization and Cardiovascular Intervention 2000; 51: 220-222.
10.
White IR, Lynch-Nylan A, Terry P, et al. PAVFs: Techniques and long-term outcome of embolotherapy. Radiology 1988; 169: 663-669.
11.
Lee DW, White RI, Eggline JV, et al. Embolotherapy of large PAVFs: long-term results. Ann Thorac Surg 1997; 64: 930-939.
12.
Dulton TAE, Jackson JE, Hughes, JMB, et al. PAVFs results of treatment with coil embolization in 53 patients. AGR Am J Roentogenol 1995; 165: 1119-1125.
13.
Gossage JR, Kanj G. PAVFs a state of the art review. AMJ respiratory critical care Med 1998; 1558: 643-661.