A 12-years-old female presented with clinical and radiological findings of acute disseminated encephalomyelitis, which is an inflammatory demyelinating disease of the central nervous system (few pediatric series have been published). We report this case to stress the importance of early screening by magnetic resonance imaging and early therapeutic intervention in acute disseminated encephalomyelitis for the prevention of high rates of morbidity and mortality.
JRMS April 2007; 14(1): 47-49
IntroductionAcute disseminated encephalomyelitis (ADEM) is a rare autoimmune inflammatory condition of the central nervous system (CNS) it is most often monophasic. Typically it is antedated by an infectious illness, most commonly measles, mumps, influenza A or B, Rocky mountain spotted fever, hepatitis A or B, infection with herpes simplex, Human herpes virus type 6, varicella, rubella, vaccinia, Epstein Barr virus, cytomegalovirus, Mycoplasma pneumonia, or streptococci. ADEM can also follow immunization; rabies, diphtheria, tetanus, small pox, Japanese B encephalitis and hog(1-3). It usually presents with multifocal neurological disturbance and altered level of consciousness(4).
Magnetic Resonance Imaging (MRI) is regarded as the investigation of choice(5-7) and usually demonstrates white matter changes, although involvement of gray matter is not uncommon(7). There is apparent improvement in outcome of ADEM if early treatment with steroids was initiated which is now widely used in treatment of ADEM.
We report a 12-year girl with ADEM who improved dramatically with steroids.
Case Report
A 12-year-old female, previously healthy and developmentally normal except for speech and language problems followed up by speech therapy, arrived at the emergency room at King Hussein Medical Center (KHMC) with a history of headache, vomiting, confusion and generalized weakness over the last few days. No history of arthralgia or arthritis and no skin rash were present. She was confused, afebrile, had stable vital signs, had meningismus and there were no focal motor findings apart from an element of hypertonia in both lower limbs, and no papilledema. Brain CT scan was normal; electroencephalogram (EEG) revealed generalized slowing consistent with the encephalopathic process. Cerebrospinal fluid (CSF) yielded the following values: protein 44mg/dl, glucose 76mg/dl with no cells, CSF culture was negative for bacteria and tuberculosis.
CSF for herpes simplex type 1, 2 by PCR was negative, CSF virology study was negative for RSV, Influenza A & B, para Influenza type 1, 2 and 3, MMR, Herpes simplex, varicella zoster, polio, coxzakie B type 1,2,3,4,5,6, Cytomegalovirus, Chlamydia, Echo virus, Rota virus, EBV, Adeno virus, and negative for Mycoplasma pneumonia and Q fever. Human immunodeficiency virus was negative, PPD negative, Cold agglutinin positive titer 1/128, ASOT titer negative, CRP negative, EBV IGM negative, ESR 10, R.F negative, ANA negative, ANCA negative, PT 14/12, PTT 40/42 and coagulation study include protein C, S, Ant thrombin III were normal, CSF lactate 21.8 mg/dl (normal < 25 mg/dl).
She was treated with Acyclovir, Cefotaxime, Vancomycin, and Dexamethasone. On the fifth day of admission the patient was unconscious but responsive to painful stimuli. Physical examination revealed stable vital signs with equal pupillary response to light. Doll’s eye response was intact, cranial nerves I, II, III, IV, V, VI, were intact.
The patient had no voluntary movement. Deep tendon reflexes were pathologically brisk in the lower extremities bilaterally with no ankle clonus. Plantar responses were equivocal. She received five days of IV high-dose Methylprednisolone 20mg/kg/day and Immunoglobulin 2g/kg over five days. Brain MRI revealed asymmetric confluent hyperintense lesion on T2W images involving the basal ganglia, right aspect of genu of corpus callosum and part of the periventricular white matter. The lesion showed no enhancement post IV contrast.
On the 10th day of admission she started to improve and became conscious, oriented with good memory and intact cranial nerves. On the 50th day of admission she had normal gait and good sphincteric control. Follow-up nine months later revealed normal neurological examination. Follow up MRI showed no significant improvement but no new lesions(9).
Discussion
ADEM is a rare inflammatory demyelinating disease of the CNS affecting predominantly children and young adults. Clinical features include sudden onset of multifocal neurological disturbances such as bilateral optic neuritis, visual field defects, aphasia, motor and sensory deficits, ataxia, movement disorders and signs of acute meningoencephalopathy with meningismus, depressed level of consciousness, focal or generalized seizures and psychosis(8).
ADEM has been described following a variety of infections including measles, varicella, infectious mono nucleosis, Mycoplasma pneumonia, and nonspecific febrile illness as in our case(15). The illness in our case started with confusion, meningismus with focal motor findings that culminated in light coma on the fifth day.
Discrimination between ADEM and the first presentation of multiple sclerosis has important prognostic and therapeutic implications. Patients with ADEM generally recover completely(9) as in our case that made complete recovery on the 10th day whereas in multiple sclerosis they may have recurrent relapses or progressive deterioration over time. Ataxia, which is common in ADEM, is uncommon feature in multiple sclerosis(10).
The corpus callosum is usually not involved in ADEM although we identified lesions in our case. We found a significant involvement of the deep gray matter particularly the basal ganglia; this finding may prove useful in distinguishing ADEM from multiple sclerosis.
Chopra et al studied the CSF electrophoresis with evaluation of the Beta-1 fraction, and showed that significant decrease in Beta-1 fraction in multiple sclerosis could prove to be an early indicator in differentiating between multiple sclerosis and ADEM(11). This was not performed in our case.
After identification of ADEM by MRI and exclusions of other possible causes of disease it is important to rapidly institute an empirical trial of high dose corticosteroids. Our patient was treated with pulse therapy of methylprednisolone with dramatic response to steroid therapy as reported by most authors(12-14).
Finally, absolute confirmation of the diagnosis of ADEM would require brain biopsy. In this case the patient improved after a trial of high dose intravenous steroids and immunoglobulin and has remained asymptomatic, brain biopsy therefore was not performed.
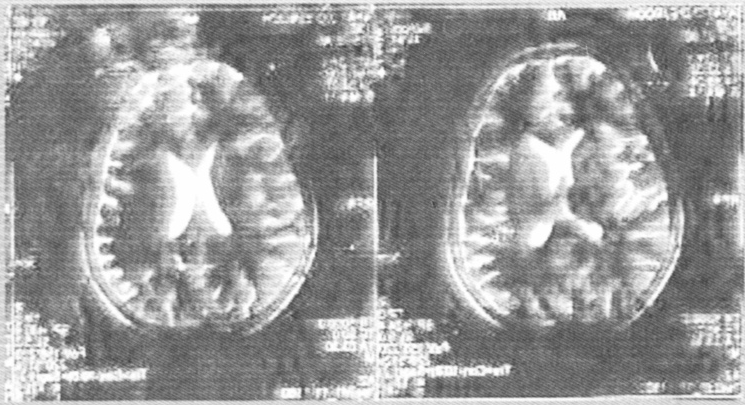
Fig. 1:T2W images revealed asymmetric confluent hyperintense lesion on T2W images involving the basal ganglia. Right aspect of genus of corpus callosum and part of the periventricular white matter
References1.
Tenmbaum S, Chamoles N, Feje-Man N. Acute disseminated encephalomyelitis: Along term follow-up study of 84 pediatric patients. Neurology 2002; 22: 1224-1231.
2.
Ruste RS. Multiple sclerosis acute disseminated encephalomyelitis, and related conditions. Semmin Pediatric Neural 2000; 7: 66-90.
3.
Dale RC, Desousa C, Chong WK, et al. Acute disseminated encephalomyelitis, multiphase disseminated encephalomyelitis and multiple sclerosis in children. Brain 2000; 123: 2407 - 2422.
4.
Johnson RT. Post-infectious demyelinating disease. In: Johnson RT. Viral infections of the nervous system. 2nd ed. Philadelphia: Lippincott-Raven 1998; 181- 210.
5.
Miller DH, Ropp SA, Ormerod IEC, et al. Magnetic resonance imaging of inflammatory and demyelinating white-matter disease of child-hood. Dev Med Child Neural 1990; 32: 97-107.
6.
Kesselring J, Miller DH, Robb SA, et al. Acute disseminated encephalomyelitis. MRI findings and the distinction from multiple sclerosis. Brain 1990; 113: 291-302.
7.
Caldemeyer KS, Smith RR, Harris TM, Edwards MK. MRI in acute disseminated encephalomyelitis. Neuroradiology 1994; 36: 216-220.
8.
Hartun HP, Grossman MB. ADEM distinct disease or part of the MS spectrum? Neurology 2001; 56: 1257-1260.
9.
Hynson JL, Kornberg AJ, Coleman LT, et al. Clinical and neuroradiologic features of acute disseminated encephalomyelitis in children. Neurology 2001; 56: 1308 -1312.
10.
Duguette P, Murry TJ, Pleins J, et al. Multiple sclerosis in childhood clinical profile in 125 patients. J Pediatric 1987; 111: 359-363.
11.
Chopra B, Abraham R, Abraham A. CSF Beta-1 globulin- a potential marker in differentiating multiplesclerosis and acute disseminated encephalomyelitis. Neurology India 2002; 50: 41- 44.
12.
Okun MS, Miliar B, Watson R. Early Diagnostic Magnetic Resonance Imaging in acute disseminated encephalomyelitis. Southern Medical Journal 2000; 93(8): 793-796.
13.
Schwarz S, Mohr A, Knauth M, et al. Acute disseminated encephalomyelitis. A follow up study of 40 adult patients. Neurology 2001; 56: 1313- 1318.
14.
Hooshang S, Remirajes AV, Zahra T. Radiological case of the month. American Medical Association 2000; 1269- 1270.
15.
Paty DW, Oger JJF, Kastrukoff LF, et al. MRI in the diagnosis of MS, a prospective study with comparison of clinical evaluation, evoked potentials, oligoclonal banding, and CT. Neurology 1988; 38: 180-185.