Hyperprolactinaemia in pregnancy is difficult to monitor due to the physiological rise in prolactin levels. Pre-existing pituitary macroadenomas can undergo significant enlargement and therefore have neurological sequelae. Microadenomas, on the other hand, very rarely cause such problems. We report on a 24 year old woman who had hyperprolactinaemia secondary to pituitary microadenoma. She was asymptomatic during most of the antenatal period, but she experienced symptoms two days prior to delivery at Queen Alia Hospital and was found to have enlargement of her adenoma. This unfortunately resulted in significant loss of her vision.
JRMS August 2007; 14(2): 46-48
IntroductionHyperprolactinaemia due to pituitary adenoma may impair fertility. The treatment of infertility is usually successful. However, the risk of tumour enlargement during pregnancy may cause pressure symptoms such as headache, nausea, vomiting, and visual disturbances. These are more likely to occur with a macroadenoma of the pituitary. We report a case of postpartum visual loss in a woman with pre-existing microadenoma of the pituitary, which apparently became enlarged during pregnancy.
Case report
A 24-year old woman (G2P1) was admitted to labour ward at Queen Alia Hospital at 39 weeks gestation. She had fever, headache and labour pains. She was known to have hyperprolactinaemia secondary to pituitary microadenoma. This was confirmed by a pituitary MRI performed one year prior to this pregnancy. Prolactin level was 104 ng/ml (normal <20 ng/ml) before Bromocriptine therapy. The latter was discontinued when pregnancy was achieved in combination with clomiphene, due to fear of adverse effects on the fetus. She did not receive antenatal care up to this point and therefore follow up with prolactin levels and visual field assessment was not done during the pregnancy.
At presentation her temperature was 38 degrees Celcius, pulse was 90 beats per minute and blood pressure was 100/60 mmHg. Vaginal examination revealed a four cm cervical dilatation. Four hours later she delivered a healthy baby weighing 3.2 kilograms. After delivery her headache persisted. Her blood pressure was normal throughout. Twelve hours following delivery she complained of partial loss of vision. Ophthalmologic assessment confirmed bitemporal hemianopia, decreased visual acuity but no papilloedema. Urgent brain MRI (Fig. 1) showed enlarged pituitary gland compatible with a microadenoma.
She was transferred to a tertiary centre for neurosurgical assessment. Medical treatment with large doses of dexamethasone for three days, which was thought to reduce oedema around the adenoma, thus decreasing pressure on the optic nerve, failed to improve her visual loss. Transsphenoidal hypophysectomy was performed on the fourth day. Histological examination confirmed the presence of pituitary adenoma (Fig. 2). Three months following surgery the patient continued to have the same visual impairment. In addition she was receiving hormonal replacement for pituitary insufficiency.
Discussion
The normal pituitary gland usually enlarges during pregnancy and previously asymptomatic pituitary tumours may become more apparent. In patients with pituitary macroadenoma 15% experienced symptomatic tumour enlargement during pregnancy. Half of these required surgery during pregnancy. On the contrary, only 1% of patients with microadenoma developed symptoms due to tumour enlargement and 4.5% had asymptomatic enlargement on radiologic examination.(1,2) In no cases was surgical intervention necessary.
Ganzell and Wang(3) reviewed the course of 85 women with previously untreated microadenoma and reported that only 5% experienced complications. Four of the five pregnancies associated with symptoms of headache and visual disturbance showed resolution following delivery. One patient who had a visual field defect noted early in pregnancy, subsequently underwent transsphenoidal hypophysectomy after Caesarean section for a triplet gestation at 36 weeks.(4) Similarly, Albrecht and Betz have confirmed a low rate of complications in women with untreated microadenoma during gestation.(5) Of 352 such cases, eight (2.3%) developed visual disturbance and 17 (4.8%) developed headaches.
Symptoms tend to occur more frequently in the first trimester than in the second or third trimesters, although the likelihood of developing visual symptoms did not differ in each trimester. Symptoms requiring therapy occurred in 20% of patients with untreated tumours, but only in 1% of treated ones.(6,7)
Although the risk of tumour expansion is small with pituitary microadenoma, careful follow up of visual field for clinical signs of pituitary fossa enlargement is essential. Follow up of prolactin levels may be difficult during pregnancy due to the physiological rise of the hormone (20 times at term), but abnormal increases of the prolactin level, outside the pregnant range for the given gestational age may signal rapid tumour enlargement.(8)
We report on this 24-year-old woman who had pituitary microadenoma before pregnancy. This unusually resulted in a major complication in the form of loss of vision in the peripartum period. It is impossible to identify which patient is at risk for symptomatic expansion during pregnancy. Very few patients develop problems. Despite that, surveillance during pregnancy is essential.
Limitation of the Study
It was not possible to perform immunohistochemical staining of the tumour specimen at our hospital. This is considered a limitation of our report.
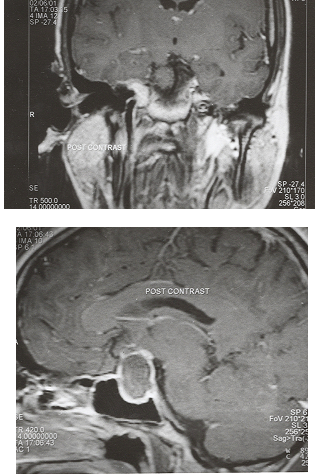
Fig. 1: Enlarged pituitary gland compatible with a microadenoma
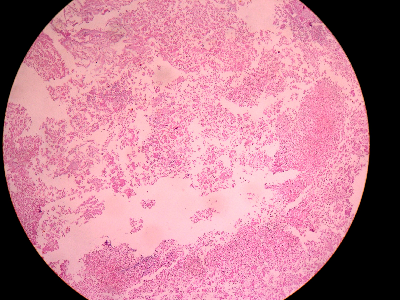 Fig. 2:
Fig. 2: Section showing necrotic tumour with focal areas of viable tissue consistent with adenoma (Haematoxylin and eosin x 40)
References
1.
Molitch ME. Pituitary disease in pregnancy. Semin Perinatol 1998; 22(6): 457-470.
2.
Molitch ME. Pregnancy and the hyper-prolactinaemic women. New England Journal of Medicine 1985; 312: 1365-1369.
3.
Ganzell C, Wang CF. Outcome of pregnancy in women with pituitary adenoma. Fertility and Sterility 1979; 31: 363.
4.
Feigenbeaum SL, Downey DE, Wilson CB, Jaffe RB. Transsphenoidal pituitary resection for preoperative diagnosis of prolactin secreting adenoma in women: Long term follow-up. J Clin Endocrinol Metab 1996; 81(5): 1711-1719.
5.
Albrecht BH, Betz G. Prolactin secreting pituitary tumours and pregnancy. In: Olesky JM, Robbins RJ (eds). Contemporary issues in endocrinology and metabolism: Prolactinoma. New York: Churchill Living stone 1995; 2: 195-218.
6.
Maygar DM, Marshall JR. Pituitary tumours of pregnancy. Am J Obst & Gyna 1978; 132: 739-740.
7.
Levy A, Lightman S. Diagnosis and management of pituitary tumours: Review. BMJ 1994; 308: 1087-1091.
8.
Soto-Ares G. Pituitary adenomas and pregnancy: Morphological features at MRI. J Radiol 2002; 86(3): 329-335.