This report documents a case of pleuropulmonary blastoma presenting in a four year old boy. This is a rare and highly malignant childhood intrathoracic neoplasm that has certain clinical and histological features which differs from the adult form of pulmonary blastoma. The differential diagnosis of an intrathoracic childhood pulmonary blastoma includes other childhood solid small round cell tumours.
Key words: Childhood, Pleuropulmonary Blastoma, Tumour.
JRMS August 2007; 14(2): 49-52IntroductionIntrathoracic and chest wall neoplasms in the paediatric age group are uncommon. Yet, they are some of the more important solid tumours of childhood. For instance, Ewing’s sarcoma, primitive neuroectodermal tumour (Askin’s tumour), and rhabdomyosarcoma are principle tumour types of the chest wall, whereas neuroblastoma, teratoma and malignant lymphoma are the major intrathoracic tumours.
Pulmonary blastoma is a rare and highly malignant neoplasm which occurs mainly in adults. Their occurrence in the paediatric age group is extremely uncommon, usually occurring in children before the age of 5 years and exhibiting variable anatomic locations within the thoracic cavity. They are commonly associated with cystic malformations of the lung.(1-5)
The diagnosis of pulmonary blastoma may be suggested by fine needle aspiration biopsy, but histopathologic examination of tissue is mandatory for a definitive diagnosis.(6) We report on an isolated case, in a four year old boy, that presented with a lung mass for the first time at King Hussein Medical Center.
Case report
A 4-year-old boy presented with cough and dyspnoea that was progressive over a period of three weeks. On examination, his general condition was poor. He had tachycardia, cyanosis and absent air entry on the left side of the chest. There was no lymphadenopathy and no organomegaly was felt on abdominal examination.
Chest radiograph and computed tomography revealed the presence of a large homogenous tumour occupying the left hemithorax with associated right shift of the mediastinum (Fig. 1 & 2). A fine needle aspiration was performed and the cytopathology report confirmed the presence of a malignant small round cell tumour.
As the patient’s condition was grave and unfit for immediate surgery, he received four cycles of chemotherapy in the form of Vincristine, Cyclophosphamide, Carboplatin, and VP16. The general condition of the boy improved with remarkable shrinkage of the mass as seen radio- logically (Fig. 3). A decision was then taken to operate and remove the residual tumour.
A hemithoracotomy was performed and a large tumour was seen adherent to the left pleura, which was compressing the underlying left lung.
The tumour was shelved from the parietal pleura, the superior surface of the left diaphragm, and the prespinal muscles. The recovery from the operation was uneventful. Unfortunately, the tumour recurred while the patient was on postoperative chemotherapy and died 8 months later because of severe respiratory distress due to extensive mediastinal recurrence. There was no evidence of distant metastases at the time of death.
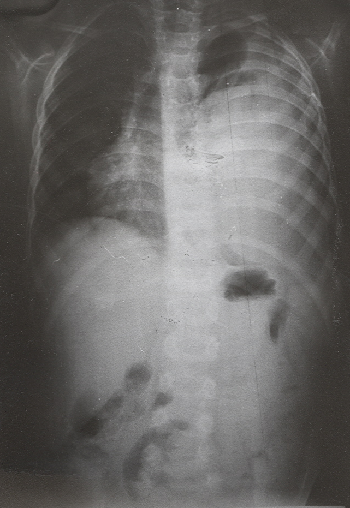 Fig 1:
Fig 1:Chest radiograph showing a large mass occupying the left hemithorax
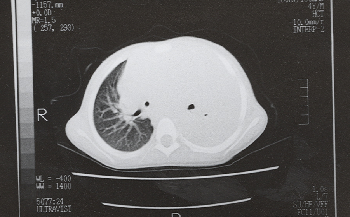
Fig 2:CT scan showing a large tumour in the left hemithorax with displacement of the mediastinum to the right (Prior to treatment).
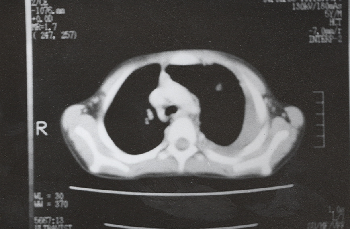 Fig 3:
Fig 3:CT scan showing marked shrinkage of the tumour following chemotherapy.
Histopathology
Gross examination of the specimen showed a multilobated mass, which was partially covered by a glistening capsule and measured 12cm in its greatest dimension. On sectioning the tumour was variegated in appearance with solid grey to white areas, with focal haemorrhagic cystic component at the periphery. Foci of frank cartilaginous component were also noted. Multiple sections were taken for histology.
Histologically, H&E stained sections revealed a malignant cellular polymorphic tumour composed predominantly of small cells with round to oval hyperchromatic nuclei, arranged in condensed blastematous islands with numerous mitotic activity.
These blastematous areas blended with immature malignant chondroid element (Fig. 4), and a loosely arranged spindle mesenchymal component composed of highly pleomorphic cells including multinucleated bizarre tumour giant cells with large eosinophilic cytoplasm (Fig. 5). Intracytoplasmic and extra-cytoplasmic eosinophilic inclusions were seen. There were extensive foci of tumour necrosis and multiple small cystic foci lined by benign appearing respiratory type epithelium were present (Fig. 6), fulfilling the criteria needed for the diagnosis of pleuropulmonary blastoma of childhood. The periphery of the tumour showed attached normal pleura and subpleural lung tissue.
Immunohistochemistry confirmed the presence of mixed epithelial and sarcomatous components. Both the blastematous and the large multinucleated cells were immunoreactive with alpha-1-antitrypsin. The mesenchymal areas showed focal immunoreactivity with myoglobin suggesting a rhabdomyosarcomatous differentiation. The chondroid areas stained uniformly with S100 protein. The cells lining the cystic spaces were immunoreactive with epithelial membrane antigen and cytokeratin.
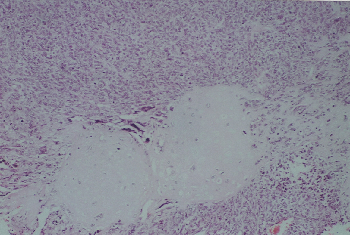 Fig 4:
Fig 4: Islands of malignant chondroid tissue surrounded by blastematous round cell component. (H&E x200)
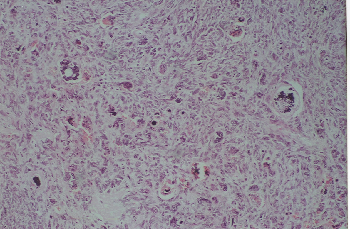
Fig 5: High-grade malignant mesenchymal component with numerous bizarre multinucleated tumour giant cells. (H&E x 400)
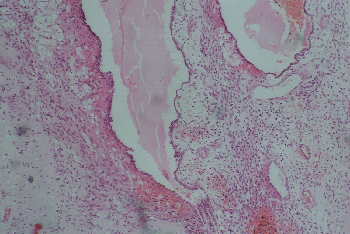
Fig 6: Cystic spaces lined by benign columnar epithelium and surrounded by malignant mesenchymal component. (H&E x 200)
Discussion
Pulmonary blastoma is an uncommon and highly malignant neoplasm, that occurs mainly in adults.(1-5) It was described first by Barnard(7) in 1952 as “embryoma of lung” because of its resemblance to fetal lung. In 1961, Spencer(8) reported three new cases and suggested the name “pulmonary blastoma”, because of its resemblance to nephroblastoma, and because of the postulated concept that these tumours arose from primitive totipotential cells capable of forming both malignant mesenchymal and epithelial elements.
Pulmonary blastoma is considered as one of two distinct clinical pathological types of mixed malignant tumours of the lung, the other being carcinosarcoma. The latter tumour is applied to lesions containing a mixed squamous carcinoma and frank fibrosarcomatous stroma and usually appears as an endobronchial polypoid mass(3,4) and carries a worse prognosis.
The typical pulmonary blastoma on the other hand is composed of well to poorly differentiated glands in a cellular primitive mesenchymal tissue, which may contain cartilage or bone.(1-7) This neoplasm is usually located in the peripheral portion of the lung and has a striking resemblance to fetal lung.
Childhood pulmonary blastomas, which are also known as pleuropulmonary blastoma, are rare and differ from the adult type in several aspects. The adult type is virtually always located within the lung substance and is composed of malignant epithelial and mesenchymal/blastemal tissue.
In contrast, the childhood tumours can occur in the lung, pleura or mediastinum, as seen in our case which was pleural based. In addition, in all the reported cases of childhood pulmonary blastoma, none contained malignant epithelial component(1-10) but if they do exist, they must be exceedingly rare and therefore, it is justifiable to separate the adult type from the childhood type on both clinical and pathological grounds.
Childhood pulmonary blastoma has been divided into three subtypes: Type I that is predominantly cystic; Type II that is cystic and solid, and Type III that is predominantly solid, as in our case.
A case of childhood pleuropulmonary blastoma was examined by immunohistochemical, ultrastructural, and cytogenetic methods.(10) Ultrastructurally, only undifferentiated mesenchymal cells were present. Cytogenetic analysis revealed abnormalities of 2q, namely partial trisomy. Involvement of 2q has also been described in other childhood tumours such as hepatoblastoma and embryonal rhabdomyosarcoma. This observation suggested a common genetic mechanism in some paediatric embryonal malignancies.
Furthermore, certain genetic abnormalities have also been recently described, namely gains in chromosome 8 in all the mesenchymal elements of the tumour,(11) and P53 mutations demonstrated by polymerase chain reaction.(12)
Pulmonary blastoma occurring in children is undoubtedly a rare tumour with around 76 cases reported so far. Their ages ranged from 2 months to 15 years of age. The cytological appearances of pulmonary blastoma have been described,(6,13,14) but confirmatory diagnosis requires histopathologic diagnosis with the support of immunohistochemistry.
The behaviour of these tumours is unpredictable, but usually grave. Surgery is the preferred treatment, as the effectiveness of radiotherapy and chemotherapy has not been conclusively established. Although some patients survive for a long time,(5) the prognosis is generally poor.
Bad prognostic factors include the presence of metastasis at the time of diagnosis, tumours larger than 5cm, and the predominance of solid areas.
References1.
Manivel JC, Priest JR, Watterson J, et al. Pleuropulmonary blastoma. The so-called pleuropulmonary blastoma of childhood. Cancer 1988; 62: 1516-1526.
2.
Ohtomo K, Araki T, Yashiro N, Iio M. Pulmonary Blastoma in Children Radiology 1983; 147: 101- 04.
3.
Dehner LP. Paediatric Surgical Pathology 2nd ed. Baltimore, Williams&Wilkins 1987; 229-230, 245-247.
4.
Rosai J. Lung and Pleura. Ackerman’s surgical pathology. New York: Mosby-year Book, 1996: 400-402.
5.
Gibbons JRP, Mckeown F. Pulmonary blastoma with hilar lymph node metastases. Cancer 1981; 47: 152-155.
6.
Shin BK, Kim MK, Park SH, et al. Fine needle aspiration cytology of Pleuropulmonary blastoma: a case report with unusual features. Diagnostic cytopathology 2000; 25: 397-402.
7.
Barnard WG. Embryoma of lung. Thorax 1952; 7: 299-301.
8.
Spencer H. Pulmonary blastoma. J Pathol.Bacteriol 1961; 82: 161-165.
9.
Karcioglu ZA, Someren AO. Pulmonary blastoma. A case report and review of literature. Am J Clin Pathology 1974; 61: 287-295.
10.
Sciot R, Dalcin P, Brock P, et al. Pleuropulmonary blastoma: Genetic link with other embryonal malignancies? Histopathology 1994; 24: 559- 563.
11.
Vargas SO, Nose V, Fletcher JA, Peres-Atayde AR. Gains of chromosome 8 are confined to mesenchymal components in pleuropulmonary blastoma. Pediatriatric Dev Pathology 2002; 5(2): 221-222.
12.
Kusafuka T, Kuroda S, Inoue M, et al. P53 gene mutations in pleuropulmonary blastoma. Pediatr Haematol Oncol 2002; 19(2): 117-128.
13.
Drut R, Pollono D. Diagnosis by fine needle aspiration cytology: A case report. Diagnostic cytopathology 1998; 19: 303-305.
14.
Nicol K, Geisinger K. The cytomorphology of pleuropulmonary Blastoma. Archives path Lab Med 2000; 124:416-418.