Objective: Saudi Arabia has a high incidence of urolithiasis. This study was undertaken to understand the composition and location of the stones from patients living in the province of Al-Jouf of Saudi Arabia.
Methods: Fifty-eight renal calculi from Al-Jouf area of Saudi Arabia were analyzed by semiquantitative titrimetric and colorimetric methods.
Results: The urinary stones were mainly localized in the bladder (36.3%) followed by the kidneys (27.6%) and were more frequent in males (88%). The result of the analysis shows that the calculi belong to oxalate (84.5%), calcium (65.5%), magnesium (58.6%), urate (36.2%), phosphate (27.6%), carbonate (13.8%), ammonium (6.9%) and cystine (1.7%). The most frequent chemical constituent was calcium oxalate (48.3%) followed by ammonium urate (22.4%), calcium phosphate (15.5%) and magnesium phosphate (13.8%) and pure form of uric acid (13.8%). Oxalate containing stones were more frequent in males than in females while phosphates containing ones were less frequent in males than in females.
Conclusion: The findings of the present work indicate that urolithiasis in the province of Al-Jouf represent common urological problem and is correlated with the nutritional, environmental and genetic factors.
Key words: Urinary calculi, Uric acid, Ammonium, Calcium Oxalate, Phosphate, Cystine, Saudi Arabia.
JRMS Dec 2007; 14(3): 15-19
IntroductionUrinary calculi have afflicted humankind since antiquity. Scientists have found evidence of kidney stones in an Egyptian mummy more than 7000 years old.(1) These stones are more common in some parts of the world including Saudi Arabia.(1,2) The risk of urolithiasis shows different frequencies: 1-5% in Asia, 5-9% in Europe, 13% in North America and 20% in Saudi Arabia.(3-6) One in five of all patients attending the urologic clinics of King Abdulaziz University Hospital, Jeddah had urinary calculi.(1)
Epidemiological studies show that renal stone formation is a complex multifactorial disease associated with dietary habits, life-style, socio-economic status, environmental and genetic factors.(7,8) The majority of the reports showed no evidence of any rise in the risk of stone formation in relation to tap water hardness.
The chemical composition and location of the urinary calculi differ in various parts of the world and change over time due to environmental, nutritional and genetic factors.(5,7,9) Chemical analysis gives important evidences for the origin, etiology and the metabolic basis of stone formation. Accordingly, this investigation was done to characterize the chemical composition of renal stones from Al-Jouf province of Saudi Arabia.
Methods
Fifty-eight urinary calculi belonging to Saudi (n=46) and non-Saudi (n=12) patients resident in Al-Jouf province of Saudi Arabia were used for chemical analysis. These stones were either removed surgically or were expelled by urination during the period January 2004 to January 2005. The sample represented six nationalities (Saudi, Egyptian, Bengali, Sri Lankan, Syrian and Pakistani) that were resident in Al-Jouf area for three years or more.
Analyses have been carried out at the central laboratory of Prince Abdel-Rahman Al-Sudary Hospital, Skaka-Al-Jouf and at the research laboratories of the Department of Medical Laboratory Sciences, Al-Jouf University. The stones were powdered in a mortar and were analyzed chemically by semiquantitative titrimetric and colorimetric methods by using two different kits supplied by Semmelweis Co., Maascia Bruneli division (Italy) and Lancer, Sherwood Medical Co. (Ireland) respectively. Both powdered stones and the standards were analyzed for carbonate, oxalate, phosphate, uric acid, ammonium, magnesium, calcium and cystine contents. Organic and inorganic nature of the renal stones was identified by flame and burning tests.(10)
Results
Out of 58 renal stones, 51 (88%) stones belonged to males while 7(12%) belonged to females giving a male to female ratio of 7.3:1. The age of the patients ranged from three to 56 years while 36(62.1%) of the patients were in their third decade of life (Table I & Fig. 1).
Table I: Distribution of calculi according to age
|
Group age (years)
|
Number of stones
|
Percentage
|
|
Less than 20
|
1
|
1.7
|
|
20-29
|
7
|
12.1
|
|
30-39
|
36
|
62.1
|
|
40-49
|
13
|
22.4
|
|
50-59
|
1
|
1.7
|
|
Above 60
|
0
|
0.0
|
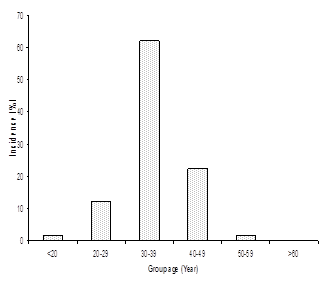
Fig. 1: Distribution of calculi according to age
Calculi were mainly localized in the bladder (36.2%) followed by kidneys (27.6%), and ureters (25.9%) while 10.3% were passed calculi (Table II & Fig. 2). The ratio of right kidney to left kidney stones was 5:3 with no bilateral kidney nephrolithiasis.
Table II: Distribution of calculi according to location
|
Location
|
Number of Stones
|
Percentage
|
|
Right kidney
|
10
|
17.2
|
|
Left Kidney
|
6
|
10.4
|
|
Ureters
|
15
|
25.9
|
|
Urinary bladder
|
21
|
36.2
|
|
Urethral
|
0
|
0.0
|
|
Expelled calculi
|
6
|
10.3
|
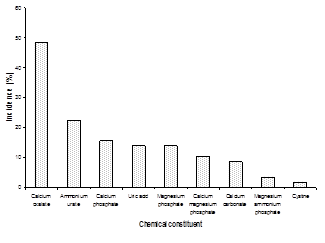 Fig. 4:
Fig. 4: Incidence of the chemical constituents of the urinary stones
Discussion
Renal stones represent major urological problem in all parts of the world including Saudi Arabia.(1,2,11) About 12% of the population of the European Union suffers at least one process related to urolithiasis with variable frequency as shown with the epidemiological studies such as Italy (13%), Sweden (8.9%) and Spain (12.3%).(5,12)
Urinary stones incidence is higher in countries with warm or hot climates. Exposure to sunlight and seasonal variation may enhance calcium absorption and urinary excretion, which leads to stone formation.(13,14) An increase of stone formation was noticed among American army personnel deployed in Kuwait from March through August 2003.(15) Reports from different parts of the world indicate that geographical variations in the incidence of urinary calculi are correlated with socio-economic conditions.(11) Obesity, calculi family history together with high protein, fat, energy and vitamins intake is also risk factors.(5,9,16-19) No evidence of stone formation risk was found in relation to drinking tap water.(5,17)
The population of Al-Jouf Province is about 361,000 where Saudi to non-Saudi ratio is about 6:1. The present study shows that males of this province are more affected with urolithiasis than females with a ratio of 7.3:1. This ratio is higher than those recorded in other provinces of Saudi Arabia.(1,11,20,21) The male predominance may be related to the climate conditions and life-style in Saudi Arabia where women, in contrary to men, spend most time indoors with their families. Chronic exposure to hot environment and massive sweating with subsequent dehydration and urine concentration increase the prevalence of urolithiasis. Reports from other countries indicated that males are more affected than females such as Libya 2.5:1, Algeria, 4:1, Sweden, 3:1 and United Kingdom, 2.7:1.(22) Some studies ascribed the high prevalence of nephrolithiasis in males to the effect of sex hormones on some lithogenic risk factors where androgens appear to increase and estrogen to decrease urinary oxalate excretion and kidney calcium oxalate deposition.(5, 23)
The present work shows urolithiasis in Al-Jouf Province develops more frequently in the age group of the third decade of life. This result is in agreement with other studies from Saudi Arabia where the peak age of presentation is 22-44 years.(1,21,24-27) The urolithiasis peak age in Al-Jouf province is similar to those of Sudan,(28) Jordan(29) and Southern Iraq.(30)
The results also show that the urinary stones in Al-Jouf province are mainly localized in the bladder. In the last three decades, bladder stone has almost disappeared in the Western countries where it is presently mainly restricted to elderly men with prostatic obstruction. Bladder stones are related to poor socio-economic conditions(5) and still predominate in the developing countries including Saudi Arabia.(1,31-34) For instance, the bladder stones dropped from 30% in 1965 to 5% in 1985 in India(35) and from 50% in 1950 to 5% 1985 in Japan(36) as a result of improved socio-economic conditions. Bladder stones are also associated with prostatic hyperplasia, neurogenic bladder and cancer.(37)
In the industrialized countries both sides of the urinary tract are affected equally and about 40% of the patients have bilateral calculi. In the present investigations the right kidney was more affected than the left one with the ratio of 3:2 and bilateral kidney calculi were not seen. Bilateral stones have been reported from other regions of Saudi Arabia.(38) Kidney stones are associated with family history, stressful life and genetic factors as seen in cystinuria and tubular acidosis.(9)
Most of the investigated calculi contained calcium mainly in the form calcium oxalate followed by calcium phosphate, calcium magnesium phosphate and calcium carbonate in this order. Calcium oxalate stones were also reported to be the most frequent in other regions of Saudi Arabia(27) and as seen by similar works in other countries, with 66.7% in Sudan(39), 90.4% of the upper urinary tract stones and 65% of the bladder stones in Norway,(12) 70.5% in Algeria(40) and 75.4% in Albania.(6) Calcium stones occur with hypercaliuria as a potential side effect of high dietary calcium, hyperparathyroidism and calcium supplement.
The present investigation further reveals high prevalence of oxalate calculi in males than in females. This may be due to the fact that androgens increase while estrogens decrease urinary oxalate excretion and kidney calcium oxalate deposition.(41) Oxalate calculi could result from too much oxalate in the diet and likely to occur in people having tubular epithelial injury and those suffer a lack of urinary inhibitors of crystal formation.
The results also show that phosphate stones predominated in women. Infection of the urinary tract, which is more common in women, plays an important role in phosphate stone formation. The struvite calculi (made of magnesium ammonium phosphate mixed with mucopolysaccharide matrix) were observed in 3.4% of the investigated stones. These stones have high potential life-threatening complications and formed as a consequence of urinary tract infection caused by certain types of bacteria specially urea-splitting ones.(22,42) The incidence of these stones was 3% in Riyadh province,(27) 7% Sudan,(39) 1.6% in Japan,(43) 10.3% in Albania(6) and 24.6% of the pediatric urolithiasis in Algeria.(40) Struvite stones occur in patients with chronic urinary tract infection and are also known as infection calculi.
Uric acid stones frequency in Al-Jouf province as seen in the present study is higher than those reported in Riyadh area (19%),(27) Sudan (13.2%), Japan (2.9%), Albania (12.5%).(6,39,43) Uric acid calculi are diet related and develop with increased urine acidity which crystallizes undissociated uric acid. The Saudi diet including that of Al-Jouf Province is over rich in animal proteins.(2,17)
Ammonium calculi incidence in Al-Jouf province as is shown in the present investigation is lower than that seen in similar studies: 32.9% in Sudanese children,(39) 29.5% in Algeria,(40) and 7.2% in Albania.(6) Ammonium urate predominated in the chemical components of the bladder stone in the 20th century.(1,6) The possible etiologic factors related to these calculi are those that increase the urinary ammonium concentration.
The frequency of cystine calculi in Al-Jouf province is in line with most incidences from other regions of Saudi Arabia and some countries such as Sudan and Albania.(6,39) Cystine calculi are diagnostic of cystinuria, a hereditary condition in which the kidneys do not reabsorb this amino acid which is insoluble and precipitate when the urinary pH value becomes lower than 6.0.(10)
More work is needed to understand the pathogenesis of urolithiasis in Al-Jouf province and other parts of Saudi Arabia.
Limitation of the Study
The size distribution of the calculi can not be done because a considerable number of the patients of Al-Jouf province attend the urologic clinics in Riyadh and Jordan for better facilities.
References
1.
Kassimi MA, Abdul-Halim RE, Hardy MJ. The Problem of urinary stones in Western Region of Saudi Arabia. Saudi Med J 1986; 7(4): 394-401.
2.
Robertson WG, Nisa M, Husain I, et al. The importance of diet in the etiology of primary calcium and uric acid stone formation: the Arabian experience. In: Walker VR, Sutton RL, Cameron EB, Pak CC, Robertson WG, editors. Urolithiasis. London: Plenum Press 1989; 735-739.
3.
Pak CY. Kidney stones. Lancet 1998; 351: 1797-1801
4.
Robertson WG, Hughes H. Epidemiology of urinary stone disease in Saudi Arabia. In: Ryall R, Bais R, Marshall VR, Rofe AM, Smith LH, Walker VR. Editors. Urolithiasis New York: 1996; 1652.
5.
Ramello A, Vitale C, Marangella M. Epidemiology of nephrolithiasis. J Nephrol 2000; 13(3): 45-50
6.
Bulo A, Refatllari E, Koci K, et al. Infrared spectroscopy in kidney and biliary stone disease. Jugoslov Med Biochem 2004; 23: 285-288
7.
Robertson WG, Hughes H. Importance of mild hyperoxaluria in the pathogenesis of urolithiasis: new evidence from studies in the Arabian peninsula. Scanning Micros 1993; 7: 391-394
8.
Serio A, Fraioli A. Epidemiology nephrolithiasis. Nephron 1999; 81(1): 26-30.
9.
Curhan GC, Willet WC, Rimm EB, Stampfer MJ. Family history and risk of kidney stnes. J Am Nephrol 1997; 8: 1568-1573.
10.
Jarrar BM, Taib NT. Laboratory techniques for calculi analysis. Riyadh: King Saud University Press 2003; 70-72
11.
Abdel-Halim RE. Urolithiasis in adults: Clinical and biochemical aspects. Saudi Med J 2005; 26(5): 705-713.
12.
Otnes B. Crystalline composition of urinary stones in Norwegian patients. Scan J Urol Nephrol 1983; 17(1): 85-92.
13.
Al-Hadramy MS. Seasonal variations of urinary stones colic in Arabia. J Pak Med Assoc 1997; 47: 281-284.
14.
Stuart RO, Hill K, Poindexter J, Pak CY. Seasonal variations in urinary risk factors among patients with nephrolithiasis. J Lithotr Stone Dis 1991; 3: 18-27.
15.
Evans K, Costabile RA. Time to development of symptomatic urinary calculi in a high risk environment. J Urology 2005; 173(3):858-861.
16.
Abdel-Halim RE, Baghlaf AO, Farag AB. Clinical chemical study of urinary stones in Saudi Arabia. 1. Uric acid stones. In: Schwille PO, Smith LH, Robertson WG, Vahlensieck W. (editors). Urolithiasis and related clinical research. London: Plenum Press. 1985; 715-718.
17.
Abdel-Halim RE, Baghlaf AO, Sibaei AL, et al. Urolithiasis in the Western Region of Saudi Arabia: A clinical, biochemical and epidemiological study, Riyadh: King Abdel-Aziz City for Science and Technology 1996; 274-278.
18.
Curhan GC, Willet WC, Rimm EB, Stampfer MJ. A prospective study of dietary calcium and other nutrients and the risk of symptomatic kidney stones. N Engl J Med 1993; 328: 833-838.
19.
Curhan GC, Willet WC, Knight EL, Stampfer MJ. Dietary factors and the risk of incident kidney stones in younger women: Nurse health study 11. Arch Intern Med 2004; 164: 884-891.
20.
Taha S, Mitry NF, Hiondi G. The pattern of the urinary calculi in the Eastern Province of Saudi Arabia. Arab Journal of Medicine 1985; 4: 4-8
21.
Hanash KA, Bissada NK, Woodhouse NJ. Pattern of calcium in normo- and hypercalciuric patients with calcium urolithiasis in Saudi Arabia.Urology 1985; 26(1): 27-32.
22.
Naas T, Al-Agili S, Bashir O. Urinary calculi: bacteriological and chemical association. Eastern Mediterranean Health J 2001; 4(5): 756-762.
23.
Chandhoke FJ, Grampas SA. Role of sex hormones in experimental calcium oxalate nephrolithiasis. J Amr Soc Nephrol 1999; 10(14): 376-380.
24.
Abdel-Halim RE, Baghlaf AO, Farag AB. Clinico- chemical study of urinary stones in Jeddah. 11. Oxalate stones. In: Jardin A.(editor). Proceeding of the xxe Congres de la Societe International Urologie.Paris: la Societe Internationale Urologie; 1985; 221-227.
25.
Abomelha MS, Al-Khader AA, Arnold J. Urolithiasis in Saudi Arabia. J Urology 1990; 35: 31-34.
26.
Al-Rasheed SA, El-Faqih SR, Hussain I, et al. The aetiological and clinical pattern of childhood urolithiasis in Saudi Arabia. Int Urol.Nephrol 1995; 27: 349-355.
27.
Khan AS, Rai ME, Gandapur AS, et al. Epidemiological risk factors and composition of urinary stones in Riyadh, Saudi Arabia. J Ayub Med Coll Abbottabad 2004; 16: 56-58.
28.
Ibrahim A, Zein M, Beleil O. Clinical aspects of Urolithiasis in the Sudan. J R Coll Surg1979; 24: 34-39.
29.
Dajani AM, Abu-Khadra A. Urinary calcui and urinary tract infection. In: Walker VR, Sutton RL, Cameron EB. Pak, CC, Robertson WG. (editors). Urolithiasis. London: Plenum Press 1989; 277- 278.
30.
Al-Naama LM, Luay SP, Baqir YA, et al. Incidence and composition of urinary stones in Southern Iraq. Saudi Med J 1987; 8: 456.
31.
Sutor DJ, Wooly SE Illingworth JJ. A geographical and historical survey of the composition of urinary stones. Br J Urol 1974; 46: 393-407.
32.
Talut K, Rizal A, Broked JG. The endemic bladder stones of Indonesia- epidemiology and clinical features. Br J Urol 1976; 48: 617-621
33.
Nimmannist S, Malasit P, Susaongrat W. Prevalence of endemic distal renal stone in the Northeast of Thailand. Nenphron 1996; 72: 604-610.
34.
Hari P, Bagga A, Vasudev V. Etiology of nephrolithiasis in North Indian children. Pediatr Nephrol 1995; 9: 474-475.
35.
Thind SK, Sidhu H, Nath R, et al. Chronological variation in chemical composition of urinary calculi between 1965-1968 and 1982-1986 on North- Western India. In: Walker VR, Sutton RL, Cameron EB, Pak CC, Robertson WG. (editors). Urolithiasis. New York: Plenum Press 1989; 673-675.
36.
Yoshida O, Okada Y, Horii Y, Takeuchi H. Descriptive epidemiology of urolithiasis in Japan. In: Walker V, R, Sutton RL, Cameron EB, Pak CC, Robertson WG. (editors). Urolithiasis. New York: Plenum Press 1989; 651-654.
37.
Takasaki E, Suzuki T, Honda M, et al. Chemical composition of 300 lower urinary tract calculi and associated disorders in the urinary tract. Urol Int 1995; 54(2): 89-94.
38.
Abdullah AM, Abdullah MA, Abdurrahman MB, Al- Husain MA. Glucose-galactose malabsorption with renal stones in Saudi children. Ann Trop Paediatr 1992; 12(3): 327-329.
39.
Balla AA, Salah AM, Khattab AH, et al. Mineral composition of renal stones from the Sudan. Urologia Internationalis 1998; 61: 154-156.
40.
Harrache D, Mesri A, Addou A, et al. Urolithiasis in children in West Algeria. Ann. Urol (Paris) 1997; 31(2): 84-88.
41.
Fan J, Chandhoke PS, Grampas SA. Role of sex hormones in experimental calcium oxalate nephrolithiasis. J Am Soc Nephro 1999; 10(14): 376-80.
42.
Rodman JS, Seidman C, Jones R. Not all kidney stones are created equal. In: No More Kidney Stones 1996; 20-25.
43.
Ishihara Y, Tanifuji T, Higaki Y, et al. The clinical study of 794 patients with an upper urinary tract stone analyzed by Infrared spectroscopy. Hinyokika Kiyo 1987; 33(3): 344-352.