Objective: To evaluate the clinical effectiveness of periradicular nerve root infiltration of corticosteroids for lumbar radicular pain.
Methods: This study was conducted in King Hussein Medical Center between June 2003 and June 2005. A total of 28 patients with sciatica were evaluated retrospectively. All patients were investigated by MRI (20 patients had disc herniations and 8 patients had foraminal stenosis) and were treated with periradicular nerve root infiltration of corticosteroids. The periradicular therapy was indicated in patients with MRI documented disc herniations or foraminal stenosis with at least three months of persistent lumbar radicular pain that did not respond to physical therapy or other conservative therapy.
Results: After three months of follow up, 100% pain reduction was reported in 10 patients (35.7%) according to visual analogue scale, nine patients (32.1%) reported 90% pain reduction, five patients (17.9%) said that their pain decreased by 70-80%, and four patients (14.3%) reported pain reduction less than 60%. Two patients required repeated injections since periradicular nerve root infiltration did not have accepted pain relief after one week post injection.
Conclusion: Periradicular nerve root infiltration is effective and safe tool in the management of lumbar radicular pain and may deserve to be used as part of the conservative management of lumbar radicular pain before resorting to more invasive methods.
Key words: Periradicular nerve root, Infiltration, Sciatica, Disc herniation.
JRMS Dec 2007; 14(3): 46-49 IntroductionSciatic pain is classified as pain radiating from the back into the dermatome of the affected nerve root along the femoral or sciatic nerve trunk.(1) It represents a prevalent medical and socioeconomic problem.(2) More than half of the patients with sciatica report a decline in their activities of daily living and ability to work.(3) Intervertebral disc herniations are the most common cause of lumbosacral radiculopathy, and 10% to 15% of these patients eventually require surgery.(4) Overall, the vast majority of patients with lumbosacral radiculopathy recover with conservative care.(5)
Treating lumbosciatic pain caused by intravertebral disc herniation remains challenging.(6) Not only does the symptamology put a strain on patients, it is also of enormous socioeconomic impact. Next to conservative measures that include physical therapy and adequate pain medication, surgery is absolutely indicated in cases of cauda equina syndrome and severe motor deficits. In some cases, surgery seems to have identical long-term results compared with conservative management. Yet neither conservative measures nor surgery always cause sufficient results. Moreover there are a number of patients who not respond to conservative therapy, but on the other hand have no indication for surgery.(6) As a result alternative, minimally invasive, image guiding therapies, like periradicular steroid therapy has been introduced in recent years.(7-10)
Historically epidural steroid injections have been used as an adjunct in the treatment of sciatica with reported success rates ranging from 20% to 100%.(11) Selective periradicular nerve root infiltration with local corticosteroids and anesthetics has been used for preoperative evaluation of lumbosacral pain and sciatica patients in order to determine the not always clear correlation between the clinical symptoms and imaging findings.(12) Selective nerve root injection has been used to map sensory dermatomes supplied by lumbar and cervical roots.(13,14) The safety and diagnostic usefulness of nerve root injection are now well established.(15)
Most studies were done in patients with nerve root pain due to foraminal or extraforaminal disc herniation or to lateral lumbar stenosis suggesting that nerve root injection with glucocorticoids might be of therapeutic value.(15, 16)
The aim of this study is to evaluate the clinical effectiveness of periradicular nerve root infiltration of corticosteroids for lumbar radicular pain.
MethodsThis study was conducted at King Hussein Medical Center (KHMC) between June 2003 to June 2005. A total of 28 patients with sciatica were evaluated retrospectively in this observational study. The patients were selected with an unequivocal morphological imaging finding explaining the radiculopathy. The inclusion criteria were: lumbar radicular pain without sensory or motor deficit, disc herniation or foraminal stenosis with unequivocal morphological, correlate at MRI and duration of symptoms of more than three months that did not respond to physical therapy or other non invasive conservative treatment. Exclusion criteria were: workers with lifting requirements, relevant motor deficit or cauda equina syndrome, previous spinal surgery, known tumors or metastasis, traumatic spinal injury, circulatory disturbances of the lower limb and cervical myelopathy.
A total of 28 patients were included in this observational study, 10 females and 18 males with mean age of 48, five years (±10, 2), 20 patients with disc herniation and eight patients with foraminal stenosis documented by MRI analysis, were diagnosed as source of leg pain. The degree of pain was assessed after a three months period by visual analogue scale. All patients included in this study were thoroughly informed prior to the treatment; the follow up period was for three months after injection treatment.
TechniqueThe nerve root block was performed under sterile conditions. The exact level was identified with fluoroscope, and a #20 gauge spinal needle was directed toward the appropriate foramen in between two and eight cm from the midline, after the skin was anaesthetized with 2-3ml Xylocaine 2%. No premedication was given. In the medial approach the transverse process was used to gauge the depth of penetration. The needle was advanced to the transverse process (Fig.1), the depth noted, and then passed off the caudal edge approximately one cm where it should lie in close proximity to the emerging root. A more lateral approach allowed the needle to lie in a more medial position within the foramen (Fig. 2).
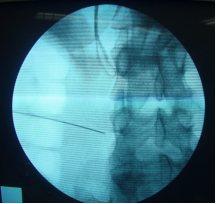 Fig. 1:
Fig. 1: Needle placement in AP view of the lumbar spine
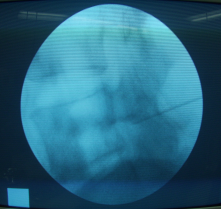 Fig. 2:
Fig. 2: Needle placement in lateral view of the lumbar spine
Lateral and anteroposterior fluoroscopic imaging was used to confirm the position of the needle, and its correct placement was confirmed by the injection of several milliliters of water with the patient feeling the same radicular pain that had been the complaint. Subsequently, 2ml bupivacaine 0.5% and 1ml triamcinolone (4mg) were injected. It should be stressed that this was a periradicular and not an intraneural injection. With this technique the nerve roots L1-L5 could be targeted. To perform a selective nerve root block at the level of S1, a different technique is required. First the image intensifier was positioned perpendicular to the foramen S1. A spinal needle was inserted perpendicular to the surface of the sacrum into the foramen.
Results
After three months of follow up, 91-100% pain reduction was reported in 10 patients (35.7%) according to visual analogue scale. Nine patients (32.1%) reported 81-90% pain reduction. Five patients (17.9%) said that their pain decreased by 71-80%, and one patient (3.6%) had a decrease of 61-70%. Only three patients (10.7%) reported pain reduction less than 60% as shown in Table I.
Table I: Pain reduction in patient after periradicular nerve root infiltration according to visual analogue scale
|
Pain reduction
(%)
|
Number of
patients
|
(%) of pain
reduction among the Study group
|
|
91-100
|
10
|
35.7
|
|
81-90
|
9
|
32.1
|
|
71-80
|
5
|
17.9
|
|
61-70
|
1
|
3.6
|
|
< 60
|
3
|
10.7
|
|
Total
|
28
|
100
|
In two patients periradicular nerve root infiltration did not show sufficient pain reduction despite a correct periradiculogram, the nerve root infiltration had to be repeated since pain reduction was 40% and 20% respectively.
One patient of the later two had 100% pain reduction and the other had 60% pain reduction, and did not require surgery. There were no major complications, in particular any infections, or nerve root injuries.
DiscussionIn the lumbosacral area, nerve root infiltration has been used for preoperative evaluation of sciatic pain,(17) this may be necessary because the imaging findings do not correlate with the clinical findings.(18) While pure mechanical compression was considered as a source of sciatica, there is increasing evidence that chemical irritation of the nerve root plays an essential role and perhaps is more important.(19) Nerve root infiltration with steroids have therapeutic effect on the discogenic sciatic pain,(12) in addition, it seems to prevent surgery in contained disc herniation.(20) The efficacy of lumbar epidural steroid injections for radicular pain ranges from 0% to 100% and lasts for less than three months.(8,21,22) Almost two thirds of the patients in this study showed more than 90% reduction of their pain and at least 70% pain reduction in 85.6% of the patients.
Several studies have sought to determine whether glucocorticoids are more effective when injected within the nerve root sheath rather than via intraspinous route.(23,24) The data obtained from this study supports that nerve root injection improves most patients with disc related sciatica.
There was no significant difference in pain reduction between lumbar disc herniations and foraminal stenosis supporting the findings obtained from other studies.(25) The study was conducted in hospitalized patients as well as outpatients. All were advised for strict bed rest for 3-5 days, as it may have enhanced efficacy on the injections.(26) Bed rest as treatment of sciatica is a controversial issue but most authors agree upon the need for 48 hours bed rest in acute sciatica
The high efficacy of periradicular nerve root infiltration with steroids can be explained by their presumed four mechanism of action: the precise delivery of the steroid and xylocaine solution, both of which have nociceptive properties, the nerve membrane stabilizing properties of both the steroid and xylocaine, the washout effect of the solution which decreases the regional levels of inflammation mediators such as interleukin-1, tumor necrosis factor, and phospholipase A2, and the potent anti-inflammatory properties of the steroids.(27,21) It remains unclear whether an acute inflammation is the reason for the sudden pain onset in disc herniation and foraminal stenosis. Our results support the hypothesis of an inflammatory mechanism because 67.9% of our patients had rapid and nearly full relieve of there pain after steroids infiltration.
All 28 patients with sciatica had fulfilled the inclusion criteria. Workers with lifting requirements were excluded because there is evidence of worse outcome in association with sciatica.(28) They were treated by periradicular nerve root infiltration.
This study had many limitations such the retrospective study design and pain relief assessment on retrospective basis is questionable and no prospective outcome can be defined, which limits the conclusion which can be drawn. Despite these limitations, there is circumstantial evidence, that periradicular nerve root infiltration is an effective, safe, and less invasive intervention, and may deserve to be used as part of the conservative management of lumbar radicular pain before restoring to more invasive methods.
References1.
Van Akkerveeken PF. Pain patterns and diagnostic blocks. In: Wiesel SW, Weinstein JN, Herkowitz H, et al, eds. The lumbar spine. Philadelphia: WB Saunders, 1996: 105-122.
2.
Lee HM, Weinstein JN, Meller ST, et al. The role of steroids and their effects on phospholipase A2: An animal model of radiculopathy. Spine 1998; 23: 1191-1196.
3.
Heliovaara M, Knekt P, Aromaa A. Incidence and risk factors of herniated lumbar disc or sciatica leading to hospitalization. J Chronic Dis 1987; 40: 254-285.
4.
Bush K, Cowan N, Katz DE, et al. The natural history of sciatica with associated disc pathology: A prospective study with clinical and independent radiologic follow-up. Spine 1992; 17: 1205-1212.
5.
Saal JA, Saal JS. Nonoperative treatment of herniated lumbar intervertebral disc with radiculopathy: An outcome study. Spine 1989; 14: 431-437.
6.
Groenemeyer DHW, Gevargez A, Schindler O, et al. CT-guided periradicular injections of corticosteroids in the management of lumbar radiculopathy associated with disk herniation. Journal of Radiology 11/15/01 Available from: URL: http://www.jradiology.com.
7.
Postacchini F. Results of surgery compared with conservative management for lumbar disc herniations. Spine 1996; 21: 1383-1387.
8.
Viton JM, Peretti- Viton P, Rubino T, et al. Short- term assessment of periradicular corticosteroid injections in lumbar radiculopathy associated with disc pathology. Neuroradiology 1998; 40: 59-62.
9.
Lutze M, Stendel R, Vesper J, Broc KM. Periradicular therapy in lumbar radicular syndromes: Methodology and results. Acta Neurochir 1997; 139: 719-724.
10.
Vijay BV, Atul LB, Gregory EL, Cammisa F. Transforaminal Epidural Steroid Injections in Lumbosacral Radiculopathy. Spine 2002; 27: 11-16.
11.
Bogduk N, Brazenor G, Christophides N, et al. Epidural steroids in the management of low back pain and sciatica of spinal origin: Report of the working party. Sydney: National Health and Medical Research Council 1993: 102-106.
12.
Lutz GE, Vad VB, Wisneski RJ. Florouscopic transforaminal lumbar epidural steroids: an outcome study. Arch Phys Rhabil 1998; 79: 1362-1366.
13.
Nitta H, Tajima T, Sugiyama H, Moriyama A. Study on dermatomes by means of selective lumbar spinal nerve block. Spine 1993; 18: 1782-1786.
14.
Curtis WS, Christopher TP, Randal AP, et al. Sumptoms Provocation of Flouroscpicaly Guided Cervical Nerve Root Stimulation. Spine 1998; 23: 2235-2242.
15.
Tajima T, Furukawa K, Kuramochi E. Selective lumbo-sacral radiculography and block. Spine 1980; 5: 68-77.
16.
Kikuchi S, Hasue M. Combined contrast studies in lumbar spine diseases: myelography and nerve root infiltration. Spine 1988; 11: 1327-1331.
17.
Dooley JF, McBroom RJ, Taguchi T, Macnab I. Nerve root infiltration in the diagnosis of radicular pain. Spine 1988; 13: 79-83.
18.
Stanley D, McLaren MI, Euinton HA, Getty CJM. A prospective study of nerve root infiltration in the diagnosis of sciatica: a comparison with radiculography, computed tomography and operative findings. Spine 1990; 15: 540-543.
19.
Olmarker K, Rydevik K. Pathphysiology of sciayica. Orthop Clin North Am 1991; 22: 223-343.
20.
Jaro K, Arto O, Antti M, et al. Cost Effectiveness of Periradicular Infiltration for Sciatica. Spine 2001; 26: 2587-2595.
21.
White AH, Derby R, Wynne G. Epidural injections for the diagnosis and treatment of low back pain. Spine 1980; 5: 78-86.
22.
Jaro K, Antti M, Mauno K, et al. Periradicular Infiltration for Sciatica. Spine 2001; 23: 1059-1067.
23.
Slosar PJ, White AH, Wetzel FT. Controversy. The use of selective nerve root blocks: diagnostic, therapeutic, or placebo? Spine 1998; 23: 2253-2256.
24.
Imed K, Joel D, Jean-Marie B, et al. Efficacy of nerve root versus intespinious injections of glucocorsteroids in the treatment of disc-related sciatica. Joint Bone Spine 2000; 67: 113-118.
25.
Narozny M, Zanetti M, Boos R. Therapeutic efficacy of selective nerve root blocks in the treatment of lumbar radicular leg pain. Available from: URL: http://www.smw.ch/pdf200x/2001 /05/smw-09689.pdf.
26.
Imed K, Joel D, Jean-Marie B, et al. Efficacy of nerve root versus interspinous injections of glucocorticoids in the treatment of disk-related sciatica. JBJS 2000; 67: 113-118
27.
Saal JS, Franson RC, Dobrow R, et al. High levels of inflammatory phospholipase A2 activity in the lumbar spine disc herniations. Spine 1990; 15: 674-678.
28.
Henry C, Jahmal CW, Andrew JH, et al. Predicting outcomes of transformational epidural injections for sciatica. Spine 2003; 3: 430-434.