ABSTRACT
Objectives: To assess the results of primary coronary angioplasty in comparison to thrombolytic therapy for the treatment of patients with acute myocardial infarction, and to compare the time from arrival of a patient with acute myocardial infarction at the coronary care unit of Queen Alia Heart Institute to having reperfusion therapy.
Methods: This is a retrospective study looking at consecutive reperfusion eligible patients with acute myocardial infarction who were treated (according to their physician's discretion) with either primary angioplasty or thrombolysis at Queen Alia Heart Institute between November 2002 and July 2005. Data regarding patients' demographic characteristics, door to reperfusion time, risk factors for coronary artery disease, hospital stay, in-hospital mortality and various complications were collected.
Results: We had a total of 277 reperfusion eligible patients, including 143 who had primary angioplasty and 134 had thrombolysis. The mean age of our population was 57.9 years. Eighty percent of them were males. Sixty six percent were smokers. The prevalence of diabetes and hypertension were 39% and 41% respectively. The mean hospital stay in the primary angioplasty group was 3.9 (SD±2.1) days compared to 6.6 (±SD 3.4) days in the thrombolysis group (P < 0.001). Primary angioplasty was associated with a statistically significant lower in-hospital mortality (2%) compared with 8.5% in the thrombolysis group (P = 0.01). There was no statistical significant difference in the incidence of reinfarction between the thrombolysis groups (1.9%) versus the angioplasty group (2.0%) (acute stent thrombosis) (P > 0.50). The mean time from arrival to the emergency room to first balloon inflation of the infarct related artery was 63 minutes compared to 42 minutes door to needle time in the thrombolysis group.
Conclusions: Our data showed that primary coronary intervention for patients presenting with acute myocardial infarction at our centre has a favorable outcome with lower in-hospital mortality and a shorter hospital stay compared to thrombolysis.
Key words: Acute myocardial infarction, Jordan, Reperfusion.
JRMS April 2009; 16(1):38-42
IntroductionReperfusion therapy using primary coronary angioplasty or intravenous thrombolytic therapy is the standard care for patients with acute myocardial infarction.(1) Despite its proven efficacy, thrombolytic therapy has limitations.
Some patients are ineligible for treatment with thrombolytics. According to the Thrombolysis in Myocardial Infarction (TIMI) classification system, thrombolysis results in a grade III flow in only 60 percent of patients, even with current fibrin-specific agents.(2)
Percutaneous coronary intervention (PCI) has been shown to be superior to fibrinolysis in the treatment of acute myocardial infarction in patients with ST segment elevation myocardial infarction (STEMI) admitted to highly experienced angioplasty centers.(3-6)
The aim of our study was to compare results of primary angioplasty for acute STEMI at Queen Alia Heart Institute (QAHI) to traditional thrombolysis. To do this we looked at hospital stay, in-hospital mortality and complications encountered during the index hospitalization. We also looked at the time from arrival of a patient with acute myocardial infarction at the emergency room to having reperfusion therapy.
MethodsWe conducted a retrospective analysis of patients with acute STEMI admitted to QAHI between November 2002 and July 2005.
We enrolled all patients who were admitted with acute STEMI and were treated with either mode of reperfusion therapy. Patients presenting within 12 hours from the onset of symptoms, with chest pain lasting at least 20 minutes, accompanied by electrocardiographic signs of ST-segment elevation of at least 0.2 mV in two or more contiguous leads or new left bundle-branch block were studied. Patients who had rescue angioplasty and those who were sent for surgery were excluded.
Data was collected regarding the demographic characteristics, risk factors for coronary artery disease, the type of myocardial infarction, time from onset of pain to presentation to the emergency room door to needle time, hospital stay, complications encountered during the index hospitalization period.
A comparison was done between the two modes of reperfusion therapy i.e. thrombolysis versus primary PCI.
ResultsThere were 277 reperfusion eligible patients with acute STEMI who were treated with either primary PCI (n=143) or thrombolysis (n=134) (Streptokinase or tPA), at the discretion of the treating physician.
Baseline characteristics of patients in the two groups were similar (Table I & Fig. 1). Prior use of aspirin, B blockers, and lipid lowering therapy was also similar in both groups.
The mean age of our population was 57.9 years. Eighty percent of them were males. Sixty six percent were smokers. The prevalence of diabetes and hypertension were 39% and 41% respectively. Family history of coronary artery disease was present in 28% and hypercholesterolemia in 26%. Hypercholesterolemia was defined as a total cholesterol of >200 mg/dl or LDL cholesterol of >130 mg/dl of the blood sample withdrawn on arrival to the Coronary Care Unit (CCU).
The mean time from onset of chest pain to seeking medical treatment was three hours and 20 minutes. The mean time from arrival to the emergency room to first balloon inflation of the infarct related artery (IRA) was 63 minutes compared to 42 minutes of door to needle time in the thrombolysis group.
The types of myocardial infarction treated included: anterior myocardial infarction in 47.3% (38.8% in the thrombolysis group versus 52% in the PCI group), inferior MI 46% (50% with thrombolysis versus 43.7% with PCI), the rest had lateral, right ventricular or posterior infarcts.
The mean hospital stay in the primary PCI group was 3.9 days (±SD 2.1 days) compared to 6.6 days (±SD 3.4) in the thrombolysis group (P < 0.001). Primary angioplasty was associated with a significantly lower in-hospital mortality (2%) compared to 8.5% in the thrombolysis group (P < 0.001).
Complications encountered during the index study period occurred in 30.5% in the thrombolysis group compared to 23% in the PCI group (P >0.10).
Complications ranged from bleeding (3.7% in the thrombolysis group versus 1.4% in the PCI group) (P > 0.317), hypotension (7.3% in the thrombolysis group versus 4.9% in the PCI group) (P > 0.317), ventricular arrhythmia (primary or secondary that needed medical treatment) i.e. ventricular tachycardia and ventricular fibrillation (6.1% in the thrombolysis group versus 7% in the PCI group) (P>0.50) as illustrated in Table II.
Bleeding was defined as any bleeding with a significant drop of hematocrit of more than 15%, intracranial or at any other site that needed medical attention or blood transfusion.
Table I:Demographic and clinical characteristics of patients in the two study groups
|
|
Thrombolytic group
|
PCI* group
|
P Value
|
|
Mean age in years
|
58.4
|
57.7
|
> 0.50 (NS)
|
|
Percentage of males
|
81.7%
|
78.3%
|
> 0.50 (NS)
|
|
Prevalence of hypertension
|
39%
|
42.6%
|
> 0.50 (NS)
|
|
Prevalence of diabetes
|
36.6%
|
40.5%
|
> 0.50 (NS)
|
|
Prevalence of smoking
|
68.4%
|
65%
|
> 0.50 (NS)
|
*PCI = Percutaneous coronary intervention
Table II: Complications encountered during the index hospitalization
|
Complications
|
Thrombolysis group
|
PCI* group
|
P Value
|
|
Bleeding
|
3.7%
|
1.4%
|
> 0.31 (NS)
|
|
Hypotension
|
7.3%
|
4.9%
|
> 0.31 (NS)
|
|
Ventricular arrhythmia
|
6.1%
|
7.0%
|
> 0.50 (NS)
|
|
AV Block
|
1 with 1st degree atrioventricular block
|
3 with 3rd
degree atrioventricular block
|
> 0.50 (NS)
|
|
Deaths
|
8.5%
|
2%
|
< 0.001
|
|
Reinfarction
|
1.9%
|
2%
|
> 0.50 (NS)
|
|
Total
|
30.5%
|
23%
|
> 0.10 (NS)
|
*PCI = Percutaneous coronary intervention
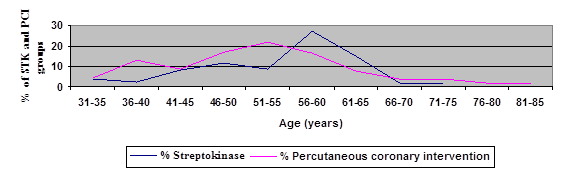 Fig. 1:
Fig. 1:Comparison between Thrombolytic and PCI groups according to age distribution
Hypotension was defined as a drop of blood pressure that required inotropic support. In the thrombolysis group, reinfarction during hospital stay occurred in 1.9% versus 2% in the angioplasty group (acute stent thrombosis), a statistically non significant difference (P > 0.50). Reinfarction was defined as rise in creatinine phosphokinase (CPK) of 1.5 times the previous value if within 48 hours of the index event, or 3 times the normal (190 U/L) if more than 48 hours of the index event. The success rate of primary angioplasty for the infarct related artery (IRA) was 96 %.
DiscussionAcute myocardial infarction remains the most alarming presentation of coronary artery disease. Figure 2 shows the typical appearance of a ruptured plaque that triggers the cascade leading to acute myocardial infarction. Patients who have an open IRA in STEMI have better clinical outcomes than patients without an open artery.(1,7-9)
Nearly two decades after clinical trials established that fibrinolytic therapy for acute myocardial infarction preserves left ventricular function and reduces mortality, there is evidence that mechanical reperfusion therapy is superior in reducing the rates of death, reinfarction, intracranial bleeding, reocclusion of the infarct-related artery, and recurrent ischemia.(1,7-9)
Initially introduced as an alternative to fibrinolytic therapy (to circumvent contraindications to its use and the risk of intracranial bleeding), primary percutaneous coronary intervention is now increasingly recognized as the reperfusion therapy of choice. The ability to restore robust coronary flow promptly in more than 90 percent of patients and the nearly linear relation between patency of the infarct-related artery (IRA) at 90 minutes after the initiation of reperfusion therapy and in-hospital mortality rates lend credibility to the momentum behind primary PCI for patients with acute STEMI.
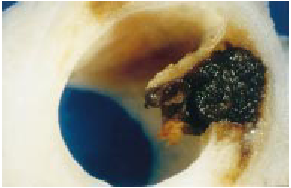
Fig. 2. A photo of a coronary artery showing a ruptured plaque with a thrombus
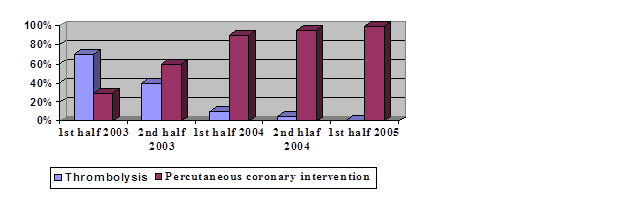 Fig. 3.
Fig. 3. The percentage of the two treatment modalities with time
In fact, a meta-analysis of 23 randomized trials in which primary PCI was compared with fibrinolytic therapy revealed that the former was superior in reducing the hospital mortality (7 percent, vs. 9 percent with fibrinolytic therapy; P<0.001), nonfatal reinfarction (3 percent vs. 7 percent; P<0.0001), stroke (1 percent vs. 2 percent; P=0.0004), and the combined end point of death, nonfatal reinfarction, and stroke (8 percent vs. 14 percent; P<0.001).(6)
Nevertheless, fibrinolytic therapy remains the mainstay of reperfusion treatment around the globe because it is more widely available than coronary angioplasty; it is easily administered without the need for sophisticated and expensive equipment and highly experienced medical personnel. In fact it is still used in up to 70% of cases of acute STEMI.(10,11)
Primary PCI for acute STEMI is now the main mode of treatment for such patients at QAHI. Nowadays the service is available 24 hours a day seven days a week. Figure 3 illustrates the decline of the number of patients getting thrombolysis for acute STEMI, and the surge of acute PCI.
The longest delay to reperfusion has been in getting medical advice. The mean time of arrival to our emergency room has been three hours and 20 minutes, thus missing out on the best window for getting reperfusion and loosing cardiac muscle since time is myocardial tissue. This is mean time is much longer than mean times reported from western counties (around 110 minutes).(12,13) This is a significant time delay that has to be addressed on a national level. Steps such as education of patients and the general public about heart disease, the seriousness of chest pain and the use of the emergency medical services should be addressed.
The mean door to needle time in the thrombolytic group was 42 minutes and the door to first balloon inflation of the IRA time was 63 minutes. This is quite good even compared to statistics from USA and UK hospitals.(14,15)
The mean age of presentation with a myocardial infarction in our study population was 57.7 years compared to 62 years in the USA, and 61 years in the UK.(12,13) This could be a reflection of the longer life expectancy in the later countries, and the higher prevalence of smoking, diabetes and hypertension in our population.
Our results show a higher prevalence of diabetes (39% versus 19% in USA & 21% in the UK). The high prevalence of diabetes mellitus has been a national concern over the past several years; this is reflected in our data. Sixty six percent of our patients were smokers (compared to 41% in the USA & 49.6% in the UK). The high prevalence of smoking confirms the need for a national strategy to combat this modifiable risk factor.
The percentage of males was 80% (72% in the USA, 80% in the UK). Family history of coronary artery disease was present in 28% of our population compared to 48% in US reports. Hyper-cholesterolemia was found in 26% compared to 37% in the USA. This could be due to our diet being a Mediterranean one.
Our hospital stay was significantly less in the PCI group (3.9 days (±SD 2.1) versus 6.6 days (±SD 3.4) than the conventional thrombolysis group (P<0.001). Our figures of hospital stay in the PCI group are comparable to those of US reports.(13) PCI is associated with a statistically significant less mortality (2% versus 8.5%) (P=0.01). Complications in total in the PCI group were less.
Our rate of reinfarction is less than that reported in US studies (2% versus 3.1%). This could be due to strict adherence to the definition of reinfarction in the USA.
ConclusionOur data showed that primary coronary intervention for patients presenting with acute myocardial infarction at our centre has a favorable outcome with lower in-hospital mortality and a shorter hospital stay compared to thrombolysis.
References1.
The GUSTO Angiographic Investigators. The effects of tissue plasminogen activator, streptokinase, or both on coronary artery patency, ventricular function, and survival after acute myocardial infarction. N Engl J Med 1993; 329:1615-22.
2.
Cannon CP, Gibson CM, McCabe CH, et al. TNK-tissue plasminogen activator compared with front-loaded alteplase in acute myocardial infarction: results of the TIMI 10B trial. Circulation 1998; 98:2805-14.
3.
Grines CL, Browne KF, Marco J, et al. A comparison of immediate angioplasty with thrombolytic therapy for acute myocardial infarction. N Engl J Med 1993; 328:673-9.
4.
Zijlstra F, de Boer MJ, Hoorntje JC, et al. A comparison of immediate coronary angioplasty with intravenous streptokinase in acute myocardial infarction. N Engl J Med 1993; 328:680-4.
5.
Gibbons RJ, Holmes DR, Reeder GS, et al. Immediate angioplasty compared with the administration of a thrombolytic agent followed by conservative treatment for myocardial infarction. N Engl J Med 1993; 328:685-91.
6.
Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet 2003; 361:13-20.
7.
Puma JA, Sketch MH Jr, Thompson TD, et al. Support for the open-artery hypothesis in survivors of acute myocardial infarction: analysis of 11,228 patients treated with thrombolytic therapy. Am J Cardiol 1999; 83: 482-487.
8.
Fath-Ordoubadi F, Huehns TY, Al-Mohammad A, Beatt KJ. Significance of the Thrombolysis in Myocardial Infarction scoring system in assessing infarct related artery reperfusion and mortality rates after acute myocardial infarction. Am Heart J 1997; 134: 62-68.
9.
French JK, Hyde TA, Patel H, et al. Survival 12 years after randomization to streptokinase: the influence of thrombolysis in myocardial infarction flow at three to four weeks. J Am Coll Cardiol 1999; 34: 62-69.
10.
Eagle KA, Goodman SG, Avezum A, et al. Practice variation and missed opportunities for reperfusion in ST-segment-elevation myocardial infarction: findings from the Global Registry of Acute Coronary Events (GRACE). Lancet 2002; 359: 373-377.
11.
The Fibrinolytic Therapy Trialists’ (FTT) Collaborative Group. Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomized trials of more than 1000 patients. Lancet 1994; 343:311-22.
12.
Andersen HR, Nielsen TT, Rasmussen K, et al. A Comparison of Coronary Angioplasty with Fibrinolytic Therapy in Acute Myocardial Infarction. N Engl J Med 2003; 349:733-42.
13.
Grines CL, Cox DA, Stone GW, et al. Coronary Angioplasty with or without Stent implantation for Acute Myocardial Infarction. N Engl J Med 1999; 341:1949-56.
14.
Pilot L, Callif RM, Sapp S, et al. Regional variation across the United States in the management of acute myocardial infarction. N Engl J Med 1995; 333: 565-72.
15.
Gershlick AH, Stephens-Lloyd A, Hughes S, et al. Rescue Angioplasty after Failed Thrombolytic Therapy for Acute Myocardial Infarction. N Engl J Med 2005; 353:2758-68.