ABSTRACT
This is a case report of a rare and severe form of congenital ichthyosis involving skin, eyes, ears, mouth, feet and hands. Unfortunately, the patient died at the fifth day of age due to sever cardio-pulmonary compromise.
JRMS April 2009; 16(1): 52-54
Introduction
The Harlequin fetus is a rare keratinizing disorder,(1) with an incidence of about 1 in 300,000 births.(2,3) The earliest record of its description is from Oliver-hart in 1750.(3)
It is the most severe form of congenital Ichthyosis,(3,4) with an ominous prognosis.(3) The term Harlequin is derived from the newborn’s facial expression and the triangular diamond shaped pattern of hyperkeratosis,(4) which resembles the uniform of the comic actor Harlequin who is a masked clown dressed in multicoloured diamond-patterned tights.
This disease primarily affects the entire skin as well as the eyes, ears, mouth and the limbs can be abnormally contracted.(4) The condition is inherited as an autosomal recessive trait,(2,5) however, a new autosomal dominant mutation may be possibly responsible.(3)
Case Report
A female infant was admitted to the neonatal unit at 36-weeks gestation weighing 2.2 kg and was the first baby of healthy consanguineous parents who were first cousins. She was a product of normal vaginal delivery with Apgar scores of 8 at 1 minute and 9 at 5 minutes.
On examination her temperature was 36.50C rectally, pulse rate was 125/min and respiratory rate 45/min. The clinical appearance was shocking; the skin was hard, thick with large shiny plates of hyperkeratotic scales separated by deep erythematous fissures (Fig. 1). The ears were poorly developed; the nose was flat and deformed. There was severe ectropion and eclabium (Fig. 2). Arms, legs and fingers were semiflexed (Fig. 3). The genitalia were normal.
The infant was nursed in a humidified incubator, an umbilical catheter was inserted, intra-venous fluids and antibiotics were started. The dermatologist was consulted who advised regular emollient and oil baths. Systemic retinoid therapy was not used. The ophthalmologist was also consulted who advised ophthalmic lubricants to protect conjunctivae.
The patient’s condition deteriorated and at the age of 5 days, she developed severe cardio-pulmonary compromise and unfortunately died.
Discussion
Harlequin ichthyosis is the most severe form of congenital ichthyosis, which includes x-linked ichthyosis, autosomal recessive lamellar ichthyosis, autosomal dominant ichthyosis vulgaris, bullous ichthyosis and
congenital non-bullous ichthyosiform erythroderma.(6) The disease is
inherited as autosomal recessive with no racial or sexual
predilection.(3,4)

Fig. 1:Large thick hyperkeratotic scales separated by deep erythematous fissures.
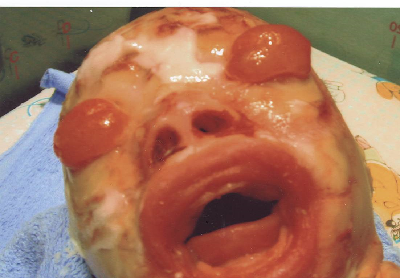 Fig. 2:
Fig. 2: Shows ectropion and eclabium.

Fig. 3: Shows flexion contractures at elbows and digits. The fingers are hypoplastic and ischemic with absent nails.
The clinical presentation in our case was similar to the cases reported elsewhere which includes markedly thickened ridged and cracked skin forming horny plates over the entire body disfiguring the facial features and constricting the digits.(1) Facial anomalies include bilateral ectropion (complete eversion of the eyelids with occlusion of the eyes), eclabium (eversion of the lips), absence of external ears and nasal hypoplasia.(7) The nails and hair were underdeveloped.
The limbs encased in the thick hyperkeratosis resulting in flexion contracture of the arms, legs and the digits.(4) The fingers and toes appear hypoplastic and ischemic.(3) The histopathologic abnormalities of the skin have confirmed the heterogeneous nature of the disorder and suggested that it is characterized by absent or abnormal lamellar bodies and absent intercellular lamellae.(8) Three biochemical phenotypes have been identified-failure to convert profilaggrin to fillagrin, and K6 and K16 expression in the epidermis-suggesting that it is a distinct disorder.(9)
The most prominent clinical complications of harlequin fetus occur secondary to breakdown of protective epithelial barrier and include sepsis and dehydration with resulting hypernatremia, in addition to impaired nutrition and pneumonia from the restrictive effects of scales on sucking and respiration.(3,4,5,10) They are extremely susceptible to changes in temperature which can result in hyperthermia.(3,4)
Most infants die within a few weeks of birth.(2,10) Unfortunately our patient died at the age of five days, however in recent years survivors have been reported due to intensive nursing and medical care. A report of survival to nine years of age has been published.(5,7)
Treatment involves intensive care of the skin, eyes and close monitoring of fluids and electrolyte status, constant support and counseling of parents and surveillance against infection and side effects of medication.(11) Retinoid therapy represents the treatment of choice for severe inherited disorders of keratinization.(12) Oral administration of isotrertinoin in a dose of 0.5 mg/kg/day within the first few days of life has improved survival of Harlequin fetuses. Prenatal diagnosis is possible by fetal skin biopsy taken at 17-20 weeks gestation.(1,7)
References1.
Behrman RE, Kliegman RM, Jenson HB. Disorders of keratinization. In: Behrman RE, Kliegman RM, Jenson HB editors. Nelson Textbook of Pediatrics. 17th edition, Saunder Philadelphia 2004; 648: 2200-2201 .
2.
Bianca S, Ingegnosi C, Bonaffini F. Harlequin foetus. J Postgrad Med 2003; 49: 81-82.
3.
Gurses D, Kilic L, Baskan M. A case of Harlequin fetus with psoriasis in his family. The Internet Journal of Pediatrics and Neonatology 2001; 2 (1): 1-7.
4.
Au S, Prendiville J. Ichthyosis fetalis. e-Medicine-Dermatology-Pediatric Diseases. Last updated: March 16. 2005; 1-12.
5.
Rook A, Wilkinson D, Ebling F. Harlequin Ichthyosis. In: Rook A, Wilkinson D, Ebling F editors. Textbook of Dermatology. 6th edition. Blackwell Science. USA 1998; 2: 1501-1503.
6.
Fitzpatrick TB, Eisen AZ, Wolff K, et al.Ichthyosis. In: Fitzpatrick TB, Eisen AZ, Wolff K, et al editors. Dermatology in General medicine. 4th edition. McGraw Hill New York 1993; 2: 2956-2957
7.
Vijaraghavan SB, Lalitha R, Ahmed AKJ. Congenital icthyosis. The fetus Net 2004; 11:09-14.
8.
Akiyama M, Dale BA, Smith LT, et al. Regional difference in expression of characteristic abnormalty of harlequin ichthyosis in affected fetuses. Prenat Diagn 1998; 18(s): 425-436.
9.
Odom RB, James WD, Berger GB. Harlequin Fetus. In: Odom RB, James WD, Berger GB editors. Andrew`s Diseases of the skin. 9th edition, 2000; 2: 704-705.
10.
Singalavanija S, Sangtawesin V, Horpoapan S, et al. Harlequin baby: A case report. J Med Assoc Thai 1998; 81(S): 365-370.
11.
Prasad RS, Pejaver RK, Hassan A, et al. Management and follow-up of harlequin siblings. Br J Dermatol 1994; 130(5): 650-653.
12.
Lacour M, Mehta-Nikhar B, Atherton DJ, et al. An appraisal of acitretin therapy in children with inherited disorders of keratinization. Br J Dermatol 1996; 134(6): 1023-1029.