Inflammatory periodontal
diseases (PD) are among the most common diseases affecting human beings and
continue to be a major concern for dentists and patients. They are caused by
microorganisms and their products and lead to destruction of the supporting
structures of the teeth. Numerous epidemiological studies, have appraised the
public health significance of PD.
The WHO Community
Periodontal Index of Treatment Needs (CPITN) was originally developed to assess
periodontal treatment needs of populations.(1) The index had been widely accepted and
extensively used in epidemiological studies for periodontal screening
worldwide. More than 300 CPITN studies from more than 100 countries are found
in WHO’s Global Oral Data Bank.(2) Data on periodontal status in
Afghanistan, however, are not available yet in the literature. This study was
conducted in the North of Afghanistan with aims of estimating the periodontal
treatment needs in relation to age, gender and level of education and
production of baseline data in this country.
Findings from this study will be useful for future comparison, analysis
and the development of strategies for PD prevention.
Methods
This is a cross-sectional
study performed at the dental clinic of the Jordanian Military Field Hospital
(JMFH) in Mazar-el-Sharif, the largest city and the capital of Balkh
Governorate in the North of Afghanistan. People come to Mazar-i-Sharif from
various surrounding rural areas, therefore it has a heterogeneous society but
with no definitive known demographic profile in terms of population number, age
and socioeconomic status. JMFH in Mazar-el-Sharif provides free medical as well
as dental care for people of Mazar-el-Sharif city and the area of Balkh
Governorate.
The aim of this study was to
determine the periodontal treatment needs based on a subset assessment. The study
was described for each patient or adult companion attending the clinic. Only two
hundred and ten subjects aged 8-62 years agreed to participate in the study and
signed a consent form. The subjects were examined between December 2002 and
February 2003 and their age, gender and level of education were recorded. The
same dentist performed the clinical examination in order to exclude
inter-examiner variability.
Assessment of periodontal
treatment needs was performed according to the CPITN criteria(1)
using a flat dental mirror and WHO periodontal probe. Each of the six dental segments
(sextants) (17 - 14, 13 - 23, 24 - 27, 37 - 34, 33 - 43, and 44 - 47) were
evaluated for each individual and was assigned a code number. Among adults aged
20 years or more, WHO suggests examining only 10 teeth: 17, 16, 11, 26 and 27
in the maxilla, and 47, 46, 31, 36 and 37 in the mandible and for subjects
under 20 years of age only six index teeth (16, 11, 26, 36, 31 and 46) were
used.(3) A sextant was examined if at least two functional
teeth were present otherwise it was considered as edentulous. If none of the
index teeth were present in the sextant, all the teeth remaining in the sextant
were examined. For each tooth, six sites were examined: mesial, midline and
distal on vestibular and lingual / palatal surfaces.
The condition of the worst affected site in the sextant
was recorded. Each sextant was designated as either healthy (score 0), bleeding
gingiva but no calculus detected (score 1), presence of supra-or subgingival
calculus or other plaque retentive factors (score 2), pockets of 4-5 mm (score
3), or 6 mm pockets or deeper (score 4). According to the highest score
recorded, the subjects and sextants were classified into the following
treatment need categories:
§
0 =
no treatment needed (score 0)
§
TN
1 = oral hygiene instructions (scores 1, 2, 3 and 4)
§
TN
2 = oral hygiene instructions and prophylaxis (scores 2, 3 and 4)
§
TN
3 = oral hygiene instructions, prophylaxis and complex treatment (score 4)
The CPITN codes were
analyzed using the individual as the unit of analysis and the CPITN score for
the individual was determined as the highest code given to any sextant in that
individual.
The collected data were
entered on a spreadsheet and analyzed using a standard SPSS®
statistical program version 10, software. Descriptive statistics were applied
and Chi-square test was used to test variables with the patient as the unit.
The level of statistical significance was set to 95%.
Results
The study population
consisted of 125 males (59.5%) and 85 females (40.5%) who were divided into
eight age groups. There was nearly equal distribution of males but no females
within the age bands: 20-24, 25-29, 30-34, 35-44 and 45-54 years. None of the
patients examined was edentulous. Age and certain demographic data of patients
are shown in Table I.
CPITN findings (Fig. 1)
revealed that 98.1% of periodontal pockets ³6mm that required complex periodontal therapy (CPITN
score 4). Table II shows the distribution of the CPITN scores the examined
patients required periodontal treatment but only 13.8% of the sample had and
within the age groups < 25 years. Gingival bleeding (score 1) was the highest (39.1%) among
the age according to different age groups. CPITN score 0 was recorded in 4
patients (1.9%) of the sample group 20-24 years while it was the lowest in
patients aged ³ 55 years where it was totally absent. The greatest age group at risk
for deep pockets was 45-54 comprising 16.2% of the whole sample.
|
|
Gender
|
Total
|
|
Age group:
|
Female
|
Male
|
No.
|
(%)
|
|
8 - 14
|
4
|
5
|
9
|
4.3
|
|
15 - 19
|
10
|
10
|
20
|
9.5
|
|
20 - 24
|
13
|
20
|
33
|
15.7
|
|
25 - 29
|
11
|
21
|
32
|
15.2
|
|
30 - 34
|
14
|
23
|
37
|
17.6
|
|
35 - 44
|
18
|
22
|
40
|
19.0
|
|
45 - 54
|
15
|
19
|
34
|
16.2
|
|
55 +
|
0
|
5
|
5
|
2.4
|
|
Level of education:
|
|
|
|
|
|
Illiterate
|
50
|
37
|
87
|
41.4
|
|
Basic school
|
30
|
58
|
88
|
41.9
|
|
College/ University
|
5
|
30
|
35
|
16.7
|
|
Total
|
85
|
125
|
210
|
100.0
|
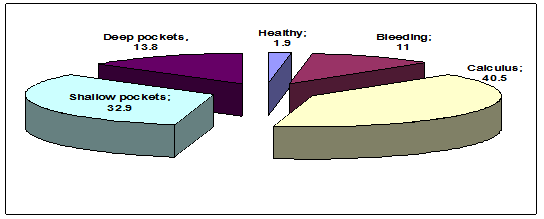
Fig. 1.
Percentage distribution of CPITN scores
|
Age group
|
Healthy
|
Bleeding
|
Calculus
|
Shallow pockets
|
Deep pockets
|
|
No.
|
%
|
No.
|
%
|
No.
|
%
|
No.
|
%
|
No.
|
%
|
|
8 - 14
|
2
|
1.0
|
3
|
1.4
|
4
|
1.9
|
0
|
0.0
|
0
|
0.0
|
|
15 - 19
|
1
|
0.5
|
4
|
1.9
|
8
|
3.8
|
6
|
2.9
|
1
|
0.5
|
|
20 - 24
|
1
|
0.5
|
9
|
4.3
|
16
|
7.6
|
7
|
3.3
|
0
|
0.0
|
|
25 - 29
|
0
|
0.0
|
2
|
1.0
|
11
|
5.2
|
12
|
5.7
|
7
|
3.3
|
|
30 - 34
|
0
|
0.0
|
2
|
1.0
|
20
|
9.5
|
8
|
3.8
|
7
|
3.3
|
|
35 - 44
|
0
|
0.0
|
2
|
1.0
|
17
|
8.1
|
17
|
8.1
|
4
|
1.9
|
|
45 - 54
|
0
|
0.0
|
1
|
0.5
|
7
|
3.3
|
16
|
7.6
|
10
|
4.8
|
|
55 +
|
0
|
0.0
|
0
|
0.0
|
2
|
1.0
|
3
|
1.4
|
0
|
0.0
|
|
Total
|
4
|
1.9
|
23
|
11.0
|
85
|
40.5
|
69
|
32.9
|
29
|
13.8
|
p<0.05, the Chi-square test
It is
obvious that periodontal treatment needs increased with age and Chi- square
test showed that there was a statistically significant difference in CPITN
sores by age (p=0.00).
A comparison by gender based
on means and SD of CPITN scores was found to be higher for females compared to males
(Table III). Fig. 2 shows that generally, healthy gingivae were found
more often in males compared to females who had lower prevalence of gingival
bleeding, calculus and shallow pockets, while the prevalence of deep pockets
was higher. However, the gender specific differences were not significant (p=0.28). Additionally, female patients have shown
highermean CPITN scores than males in the age groups 25 years and elder (Table IV), while in younger age groups males have worse periodontal conditions than females but the difference was statistically insignificant (p= 0.28). Moreover, individuals with college/university level of education had less bleeding, calculus, shallow and deep pockets compared to patients with no or basic school education. The difference in the patients’ level of education, however, was statistically insignificant (p=0.07) (Table III).
Table III. Means and SD of CPITN scores by, age, gender and
education
|
Age group:
|
No.
|
(%)
|
Mean
|
SD
|
P-value
|
|
|
9
|
4.3
|
1.22
|
0.83
|
0.00
|
|
|
8 - 14
|
|
|
15 - 19
|
20
|
9.5
|
2.10
|
0.97
|
|
|
20 - 24
|
33
|
15.7
|
1.88
|
0.78
|
|
|
25 - 29
|
32
|
15.2
|
2.75
|
0.88
|
|
|
30 - 34
|
37
|
17.6
|
2.54
|
0.87
|
|
|
35 - 44
|
40
|
19.0
|
2.58
|
0.75
|
|
|
45 - 54
|
34
|
16.2
|
3.03
|
0.80
|
|
|
55 +
|
5
|
2.4
|
2.60
|
0.55
|
|
|
Gender
|
|
|
|
|
0.28
|
|
|
Female
|
85
|
40.5
|
2.54
|
0.97
|
|
|
Male
|
125
|
59.5
|
2.40
|
0.90
|
|
|
Level of education
|
|
|
|
|
0.07
|
|
|
Illiterate
|
87
|
41.4
|
2.60
|
0.90
|
|
|
Basic school
|
88
|
41.9
|
2.28
|
0.99
|
|
|
College/ University
|
35
|
16.7
|
2.54
|
0.78
|
|
Table IV.
Means and SD of CPITN scores in different age groups by gender
|
|
Females
|
Males
|
P-value
|
|
Age group:
|
Mean
|
SD
|
Mean
|
SD
|
|
|
8 - 14
|
1.00
|
0.82
|
1.40
|
0.89
|
0.28
|
|
15 - 19
|
2.10
|
0.74
|
2.10
|
1.19
|
|
|
20 - 24
|
1.69
|
0.63
|
2.00
|
0.86
|
|
|
25 - 29
|
3.27
|
0.79
|
2.48
|
0.81
|
|
|
30 - 34
|
2.64
|
0.84
|
2.48
|
0.90
|
|
|
35 - 44
|
2.67
|
0.84
|
2.50
|
0.67
|
|
|
45 - 54
|
3.20
|
0.68
|
2.89
|
0.87
|
|
|
55 +
|
|
|
2.60
|
0.55
|
|
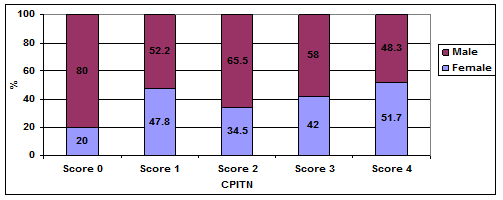
Fig. 2.
Percentage distribution of CPITN scores for females and males
Discussion
CPITN has been criticized
for overestimating both prevalence and severity of periodontitis among
young age groups and underestimating these parameters among older ones.(4)
The value of treatment needs component was criticized too, and it was omitted
from the 4th edition of the WHO Oral Health Surveys (1997).(3)
Moreover, the changes in CPITN before and after periodontal treatment were mainly
found in scores 1, 2 and 3, while other categories (scores 0 and 4) remain
approximately unchanged after treatment, with a very low percentage of subjects
with completely healthy periodontal tissues.(5) It is worthy
of note that in terms of public health, what is more important first is to know
that subjects are at risk for developing severe PD, and then, which treatments
are effective at preventing these diseases.
Regardless of what has been
mentioned previously, the CPITN has been employed as a measure of periodontal
treatment needs, in a large number of epidemiological surveys performed in
various countries and areas.(2) In addition, the system was
most suitable in respect to time available for examining periodontal status in
the present study.
This study was carried out
on a small sample of Afghan nationals attending the dental clinic at JMFH in
Mazar-i-Sharif. It is not obvious whether
it is representative of the population of the North of Afghanistan or the
entire Afghan people. However, this study was the first study conducted on
Afghan individuals using the CPITN index to assess periodontal treatment needs
of the rural population in Mazar-i-Sharif and the results of this study reveal
the periodontal treatment needs of the examined population. Moreover, the findings
are an important step towards reaching the WHO goal of Global Oral Data Bank.
Results presented here
confirm other CPITN studies(5-9) showing that most of our
subjects (98.1%) need some form of periodontal treatment and subjects with
completely healthy periodontal tissues comprised only a minority. Moreover,
more subjects here had periodontal pockets of 4mm or more (46.7%) than the
22.2% in the rural areas of Ninevah, Iraq,(10) and lower than
the 86.5% in Eastern Germany(7) and 64.8% in Quebec, Canada.(9)
Similar to other studies,(10,11) the most frequent
periodontal finding was calculus (40.5%).
It is noted that the
interpretation of the results of this limited CPITN study regarding calculus
should focus on health promotion and education, leading to improved oral
hygiene rather than on calculus removal only. After improving oral hygiene,
removal of calculus can be carried out. This approach not only manages the
present situation efficiently; but also will lead to lower calculus figures in
succeeding generations.
When making comparisons with
other studies, for example in the age group 15-19 years, these findings are
comparable to those from France (1985),(12) while for the age
group 35- 44 years our finding are comparable to those in Hong Kong (1984), and
Japan (1984) but are higher than Australia (1984), New Zealand (1981) and
Zimbabwe (1986).(13) To compare results to a Mediterranean
country, Taani in 2004(14) in North of Jordan had shown that fewer
subjects between 20 and 60 years of age have shallow and deep pockets than
subjects in the same age band in our study. Our study show higher bleeding and
calculus in younger ages while subjects in older age groups have more deep
pockets, this may be due to the strong impact of age on the periodontium. This
finding is in agreement with many studies showing increased periodontal treatment
needs with increase in age.(6-8, 10, 11)
Although, males consistently
have a higher prevalence and severity of PD than females,(15)
the percentage of males with healthy periodontal tissues (3.2%) was higher in
our study than that of females (1.2%). Bleeding, calculus and shallow pockets
were observed more in males while deep pockets were more prevalent in females.
However, the gender specific differences were not significant (p>0.05).
Our results regarding
periodontal treatment needs are similar to those of various international
studies, including those carried out in industrialized countries(6,13)
that reported high periodontal treatment needs in all age groups. Moreover, treatment
needs recorded among individuals living in industrialized countries was higher
than those in some developing countries (12) where dental care
system is confined virtually to emergency treatment. Our results also indicate
that the most frequent periodontal treatment needed was improved oral hygiene
practice and scaling as recommended in the CPITN methodology.(1)
Therefore, priority should be given to primary preventive programs aimed at
improving the periodontal health of the majority of population under study.
According to WHO country
profiles,(16) socioeconomic indicators of Afghanistan show
that in 1997 literacy was only 16% in adults, 25% in school first level and 15%
in school second level. Literacy was higher for males compared to females in the
three levels mentioned. Our results show that educated individuals in this study
population, whether in basic school level, or in college or university level,
have less need for periodontal treatment than non-educated subjects. This
conclusion is drawn from the fact that none of the illiterate subjects had
CPITN score 0. This finding is in agreement with Mengel et al. 1993(7)
and Paulander et al 2003(17) who reported
low CPITN scores were associated with a higher education level. Higher
education was found to have a positive effect on adopting health-promoting
measures. For example, highly educated subjects use dental services more than
subjects with lower level of education. Additionally, people with higher
education were also found to have less dental anxiety, which is one of the cultural
factors that was shown, according to Milgrom et al. 1985,(18)
to have an impact on patients' health behavior.
Conclusion
Periodontal status in Mazar-el-Sharif
in the North of Afghanistan was poor in different age groups with most
individuals requiring simple periodontal treatment. Therefore, comprehensive
prophylactic concepts need to be developed and introduced in childhood and
early adulthood life for the population of Mazar-i-Sharif to prevent PD. Further
research and larger studies are needed to confirm our results and monitor
changes in CPITN over time.
References
1. Ainamo
J, Barmes DE, Beagrie G, et al. Development of the World Health Organization (WHO) Community
Periodontal Index of Treatment Needs (CPITN). Int Dent J 1982; 32:
281-291.
2.
Pilot
T, Miyazaki H. Global results:
15 years of CPITN epidemiology. Int Dent J 1994; 44: 553-560.
3 .WHO Oral Health Surveys, 4th ed., 1997 in: http://www.whocollab.od.mah.se/expl/methods.html
4.
Baelum
V, Manji F, Wanzala P, et al. Relationship between CPITN and periodontal attachment loss findings in
an adult population. J Clin Perio 1995; 22: 146-152.
5.
Butterworth
M, Sheiham A. Changes in the
community periodontal index of treatment needs (CPITN) after periodontal
treatment in general dental practice. Br Dent J 1991; 171:
363-366.
6.
Flores-de-Jacoby
L, Bruchmann S, Mengel R, et al. Periodontal conditions in Rio de Janeiro City (Brazil)
using the CPITN. Community Dent Oral Epidemiol 1991; 19: 127-128.
7. Mengel
R, Koch H, Pfeifer C, Flores-de-Jacoby L. Periodontal health of the population in Eastern
Germany (former GDR). J Clin Perio 1993; 20: 752-755.
8.
Rababa’h
TA, Jama’ni F, Al-Omari MA.
Oral health survey at an airbase in Jordan. East Mediterr Health J 1998;
4: 332-337.
9.
Benigeri
M, Brodeur J-M, Payette M, et al. Community periodontal index of treatment needs and
prevalence of periodontal conditions. J Clin Perio 2000; 27: 308-312.
10. Khamrco TY. Assessment of periodontal disease using the CPITN
index in a rural population in Ninevah, Iraq. East Mediterr Health J
1999; 5: 549-555.
11. Guile EE. Periodontal status of adults in Central Saudi Arabia. Community
Dent Oral Epidemiol 1992; 20: 159-60.
12. Pilot T, Barmes DE, Leclercq MH, et
al. Periodontal conditions
in adolescents, 15-19 years of age: an overview of CPITN data in the WHO Global
Oral Data Bank. Community Dent Oral Epidemiol 1987; 15: 336-338.
13. Pilot T, Barmes DE, Leclercq MH, et
al. Periodontal conditions
in adults, 35-44 years of age: An overview of CPITN data in the WHO Global Oral
Data Bank. Community Dent Oral Epidemiol 1986; 14: 310-312.
14. Taani DSMQ. Oral health in Jordan. Int
Dent J 2004; 54(6 suppl 1): 395-400.
15. Carranza FA, Newman MG. Clinical periodontology, 8th ed. Philadelphia,
1996: WB Saunders, 74.
16. WHO country profiles in: http://www.emro.who.int /emrinfo/CountryProfiles-AFG.htm#HealthStatus
17. Paulander J, Axelsson P, Lindhe J. Association between level of education and oral health
status in 35-, 50-, 65- and 75-year-olds. J Clin Perio 2003; 30:
697-704.
18. Milgrom P, Weinstein P, Kleinknecht R,
et al. Treating fearful
dental patients. Reston: Reston publishing company Inc. 1985.