Abstract
Objective: The purpose of the present study is to
describe our experience with endoscopic third ventriculostomy in children with
obstructive hydrocephalus secondary to posterior fossa tumours.
Methods: Between January 2000 and January 2006,
42 children with posterior fossa tumour were treated. Thirty patients had
symptomatic hydrocephalus. Third ventriculostomy was performed to relieve
intracranial pressure in all cases as an urgent procedure after admission. The
other 12 cases had no hydrocephalus or non symptomatic mild dilatation of
ventricles. They were excluded from the study.
Results: Pre craniectomy endoscopic third
ventriculostomy procedures were technically successful. One case was complicated
with infection. The procedure resolved the increased intracranial pressure
before posterior fossa surgery in all cases. One case developed post operative
hydrocephalus and was treated by ventriculo-peritoneal shunt insertion.
Conclusions: Endoscopic third ventriculostomy is a
plausible choice for the emergency control of severe hydrocephalus caused by
posterior fossa tumours. It can quickly
eliminate symptoms. In addition, it eliminates the risks of cerebrospinal fluid
infection related to external drainage, minimizes the risk of over drainage
because it provides more physiological cerebrospinal fluid drainage than the
other procedures and avoids the complications of shunting procedures.
Key words: Cerebrospinal fluid shunt, Endoscopic
third ventriculostomy, Hydrocephalus, Neuroendoscopy, Posterior fossa tumor.
JRMS
August 2008; 15(2): 47-51
Introduction
Tumours of the central
nervous system are the most common solid neoplasms in infancy and most of them
are located in the posterior fossa.(1,2)
The proximity of these lesions to the
fourth ventricle explains the common presentation of these patients with
obstructive hydrocephalus as described in about 80% of the cases.(3-6)
Neurosurgeons still differ in their
opinions concerning the best way to manage obstructive hydrocephalus secondary
to posterior fossa tumours.
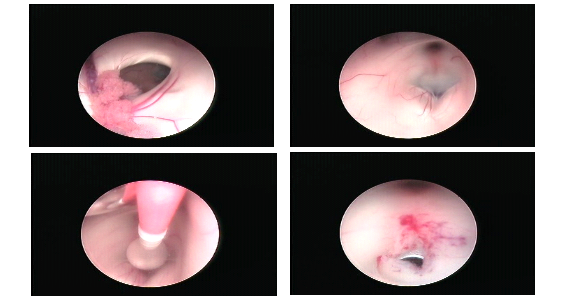
Fig.1:
Neuroendoscopic view of dilated foramen of Monro
Floor of the third ventricle
Fenestration of floor of third ventricle using Fogarty
catheter
Fenestrated floor of third ventricle
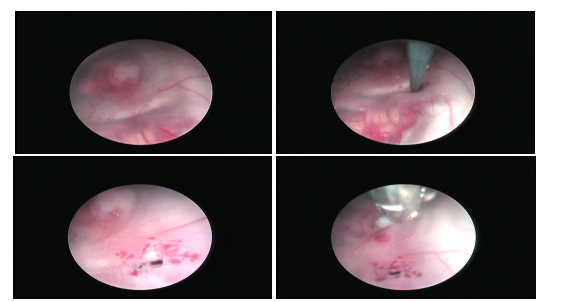
Fig. 2.
Neuroendoscopic view of a suprasellar intraventricular
seedling in a case of posterior fossa medulloblastoma
Fenestration of floor of third ventricle using blunt
probe
Fenestrated floor of third ventricle
Biopsy of suprasellar seedling
Some authors proposed a preoperative indwelling
cerebrospinal fluid shunt as
most advantageous for the subsequent surgical approach to the tumour.(3,5,7-10) Others proposed pre-treatment with corticosteroids
and direct approach to the posterior fossa pathology, when possible, and/or
external ventricular drainage, when necessary.(2,6,11-16) Based
on recent reports,(8,9,13,17,18) we
adopted the policy of performing a preoperative endoscopic
third ventriculostomy (ETV) in cases of symptomatic hydrocephalus. Our
experience over the past six years in 30 patients is discussed.
Methods
Between January 2000 and January
2006, 42 patients with posterior fossa tumour were admitted to the neurosurgery department at King
Hussein Medical Centre. All 42 patients had a CT
scan upon admission. Patients with no hydrocephalus, mild non symptomatic
dilatation of ventricles, and shunted patients were excluded from this study.
Thirty patients with CT scan showing severe
hydrocephalus, and had symptoms and signs of intracranial hypertension constituted
the study group.
Patients’ age ranged from three
to 13 years (mean age six years), 17 females and 13 males. All thirty patients were
started on corticosteroid agents on admission, brain and whole spine MRI were
obtained and ETV performed on urgent basis (seven cases as emergency
procedure). Follow up CT scan was performed after ETV for all patients.
Endoscopic third
ventriculostomy was performed using a rigid neuroendoscope. A blunt probe was
used to fenestrate the floor of third ventricle followed by fogarty catheter
number four dilatation, Lilliquest membrane was always sought and fenestrated. (Fig.
1) Biopsy was performed in one case where seedling of tumour was detected. (Fig.
2)
Tumour resection was
scheduled under non-emergency conditions on the next available surgical slot.
Results
Endoscopic third
ventriculostomy was performed in the thirty patients. There were no technical
difficulties in the procedure even in the cases associated with anatomical
distortion of the floor of the third ventricle due to the tumour. Ventricular
drainage device (reservoir) was inserted in 5 cases for the suspicion of
inadequate ventriculostomy.
The signs and symptoms of
increased intracranial pressure improved after ETV in all patients. Follow up
brain CT scan showed no complications related to third ventriculostomy except
for insignificant asymptomatic airocele in four cases. The size of ventricles
showed reduction in 25 cases (83%). One
patient developed fever and meningeal irritation signs after three days from
ETV, external ventricular drain was inserted and antibiotics started. Patient improved
and surgery was performed with no sequels.
Twenty cases underwent
definitive surgery on the next available operating slot that was 2-4 days from
performing ETV. Surgery in six patients was deferred till their general and
clinical conditions improved. Those patients presented with altered level of
consciousness and poor general condition related to vomiting and increased intracranial
pressure. Three patients’ operation was delayed due to theatre time
availability.
The definitive surgery showed satisfactory
posterior fossa condition in relation to the CSF pressure. Even with cases
which showed some tightness in the posterior fossa the routine measures were
adequate to control the pressure, especially after the cisterna magna was
opened and more CSF released.
Total resection was achieved in all cases
except for one where the tumour was adherent to the floor of the fourth ventricle.
The anatomical pathway of the CSF was opened in all cases with satisfactory
flow. The histopathology of tumours is shown in Table I.
Table I. Histopathological type of tumors
Type of Tumor | Number of cases | % |
Medulloblastoma | 15 | 50 |
Pilocytic Astrocytoma | 10 | 33 |
Ependymoma | 5 | 17
|
The post operative period showed no
complications related to CSF pressure; there was no hydrocephalus, no CSF leak,
or any CSF collection in the wound area in all cases.
None of the thirty patients needed any
further drainage procedures during the early post operative period or later on
follow up visits including the shunted case.
Discussion
The association of posterior
fossa tumors with hydrocephalus, both potentially lethal conditions,
necessitates urgent surgical treatment. The routine placement of preoperative
shunts significantly reduces the overall morbidity and mortality rates. The
advantages of preliminary shunting are rapid normalization of raised
intracranial pressure (ICP), lowering of the risk of infection due to continuous
extraventricular drainage (EVD), improvement of the patient’s general
condition, prevention of postoperative ICP elevation, and the possibility of
implementing further diagnostic and therapeutic procedures through a reservoir.(3,4,7,11,12,19)
Nevertheless, several
arguments have been raised against systematic preshunting. There is
considerable morbidity when compared with EVD for less than 5 days with a very
low complication rate (2.2%),(2,7,20-22) where a 10% rate of upward
herniation in cases of posterior fossa tumors subjected to preliminary shunting,(20) and spreading of medulloblastomas through
ventriculo-peritoneal shunts was reported.(23-25)
These arguments and the
improvements in the availability and type of neuroimaging systems that permit
earlier diagnosis have caused neurosurgeons to question the need for routine
shunt placement. Therefore, a more expectant policy (Corticosteroid therapy,
early surgery, and external ventricular drainage when needed.) was proposed and
adopted. Steroids reduce posterior fossa swelling. Preoperative drainage is
required where, despite steroids, there are serious problems, such as
decreasing consciousness or visual impairment due to papilledema.
Although theoretically appealing, this
protocol is not without concern. External ventricular drainage used in these
situations is not without the attendant risk of infection (10% reported by
Rappaport and Shalit and 4.9% by Schmid and Seiler)(12,14) and upward herniation or
hemorrhage. Seventeen to 40% of patients treated with this protocol have
uncontrolled hydrocephalus after tumor removal and required placement of a
definitive CSF shunt.(5,9,19-26)
This kind of hydrocephalus
occurs predominantly within the first month of surgery. These patients, placed
at risk of suffering intracranial hypertension, have an increased rate of CSF leakage and pseudomeningocel
formation, a prolonged hospitalization, and a high risk of pseudobulbar palsy.
Endoscopic
third ventriculostomy in the management of hydrocephalus secondary to posterior
fossa tumours was proposed, for the first time, by Chumas et al. in 1995(8)
and its efficacy was reviewed by Sainte-Rose et al. (13)
in 2001. The rational basis of ETV is provided by the obstructive nature of
hydrocephalus that is due to the presence of blockage of the CSF pathway at the
level of fourth ventricle outlets or at the aqueduct. ETV creates a
communication between the ventricular system and subarachnoid spaces at the
level of the floor of the third ventricle.
Sainte-Rose et al. reviewed 67 ETVs performed
before tumour removal in patients with severe hydrocephalus. In this series
there were no deaths and no permanent morbidity related to the procedure, a
98.5% rate of immediate symptomatic resolution, and a 94% rate of shunt-free
patients after tumour removal.(13)
Comparing these results with patients with
hydrocephalus who underwent a “conventional treatment” (steroid medications,
early surgery, and ventricular drainage) and with patients with no evidence of
ventricular enlargement, they concluded that ETV had a curative effect on
intracranial hypertension and a prophylactic effect by preventing the development
of hydrocephalus after tumour removal.
Preoperative normalization of CSF
hydrodynamics seems to decrease the risk of permanent postoperative impairment of
CSF circulation. Hopf et al.(17) and Valenzuela and Trellez(18)
have also reported a significant experience in 17 and 21 cases respectively,
both with a 76% success rate in controlling hydrocephalus.
In our unit we adopted the
policy of treating severe hydrocephalus in patients with posterior fossa tumour
with ETV. The patients were also started on steroids on admission. The procedure seems to provide a valid
alternative to placement of a permanent shunt in cases in which hydrocephalus
develops following posterior fossa surgery
ETV is a procedure that can
be performed on emergency basis, allows rapid relief of clinical signs and symptoms,
avoids the risks and complications of other approaches to treat hydrocephalus
like shunt infection and failure, upward herniation and possible peritoneal
seedling. It allows restoration of normal mechanism of CSF flow.
The burr hole used for ETV can
provide a rapid access to the ventricles post operatively if need arises. CSF
is obtained for cytology during procedure.
ETV proved successful in
immediate and long-term control of hydrocephalus both clinically and
radiological with minimal risk and complications. Pre operative ETV allowed
time to schedule the patients for definitive surgery on more convenient basis
and resuscitating patients. ETV resulted in satisfactory posterior fossa
surgical conditions. The post operative period had no complications related to
hydrocephalus, no CSF leak from posterior fossa or ETV wounds, and no
pseudomeningeocele.
Conclusion
Our work supports the trend of adopting the preoperative ETV for the
management of hydrocephalus secondary to posterior fossa tumours and is in
accordance with the conclusions reached by other authors who adopted the same
policy.
Reference
1. Cassoto A,
Buoncristiani P. Medulloblastoma in childhood. Childs Brain 1982; 9:299-308.
2. Lee M, Wisoff
JH, Abbott R, et al. Management of hydrocephalus in children with
medulloblastomas: prognostic factors for shunting. Pediatr Neurosurg 1994;
20:240–247.
3. Albright L,
Reigel DH.
Management of hydrocephalus secondary to posterior fossa tumours. J
Neurosurg 1977; 46:52–55.
4. Bognar L,
Borgulya G, Benke P, et al. Analysis of CSF shunting procedures requirement
in children with posterior fossa tumours. Childs Nerv Syst 2003; 19:332–336.
5. Reni M, Gatta
G, Mazza E, Vecht C. Ependymoma. Crit Rev Oncol Hematol 2007; 63(1):81-89.
6. Due-Tonnessen
BJ, Helseth E. Management of hydrocephalus in children with posterior fossa
tumors: role of tumor surgery. Pediatr Neurosurg 2007; 43(2):92-96.
7. Albright AL. The value of precraniotomy
shunts in children with posterior fossa tumours. Clin Neurosurg 1983; 30:278–285.
8. Chumas P,
Saint-Rose C, Cinalli G, et al. III Ventriculostomy in the management of
posterior fossa tumours in children. Proceedings of the ISPN congress, Santiago, Chile,
26–29 September 1995. Childs Nerv Syst 1995; 11:540.
9. Cinalli G. Alternatives to shunting. Childs
Nerv Syst 1999; 15: 718–731.
10. Culley DJ,
Berger MS, Shaw D, et al. An analysis of factors determining the
need for ventriculoperitoneal shunts after posterior fossa tumor surgery in
children. Clinical study. Neurosurgery 1994; 34:402–408.
11. Papo I,
Caruselli G, Luongo A. External ventricular drainage in the management of posterior
fossa tumours in children and adolescents. Neurosurgery 1982; 10:13–15.
12. Rappaport ZH,
Shalit MN. Perioperative external
drainage in obstructive hydrocephalus secondary to infratentorial brain
tumours. Acta Neurochir (Wien) 1989; 96:118–121.
13. Sainte-Rose
C, Cinalli G, Roux FE, et al. Management of hydrocephalus in pediatric
patients with posterio r fossa tumours:
The role of endoscopic third ventriculostomy. J
Neurosurg 2001; 95:791-797.
14. Schmid UD,
Seiler RW.
Management of obstructive hydrocephalus secondary to posterior fossa tumours by
steroids and subcutaneous reservoir. J Neurosurg 1986; 65:649-653.
15. Shalit MN,
Ben Ari Y, Eynan N. The management of obstructive hydrocephalus by the use of
external continuous ventricular drainage. Acta Neurochir (Wien) 1979;
47:161–172.
16. Taylor WA, Todd NV, Leighton SEJ. CSF drainage in patients with
posterior fossa tumours. Acta Neurochir (Wien) 1992; 117:1–6.
17. Hopf NJ,
Grunert P, Fries G, et al. Endoscopic third ventriculostomy: An
outcome analysis of 100 consecutive procedures. Neurosurgery 1999; 44:795-806.
18. Valenzuela S,
Trellez A.
Pediatric neuroendoscopy in Chile.
Analysis of the first 100 cases. Childs Nerv Syst 1999; 15:457-460.
19. Gross P, Goat
M, Knoblich OE. Disorders of CSF circulation after interventions in the area of
the posterior cranial fossa with prior shunt operation. Adv Neurosurg 1978;
5:199-202.
20. Epstein F,
Murali R.
Paediatric posterior fossa tumours: hazards of the “preoperative” shunt. Neurosurgery
1978; 3:348–350.
21. McLaurin RL. Disadvantages of preoperative
shunt in posterior fossa tumours. Clin Neurosurg 1983; 30:286-292.
22. Muszynski CA,
Laurent JP, Cheek WR. Effect of ventricular drainage and dural closure on
cerebro-spinal fluid leaks after posterior fossa tumor surgery. Pediatr
Neurosurg 1994; 21:227–231.
23. Fiorillo A,
Maggi G, Martone A, et al. Shunt-related abdominal metastases in an
infant with medulloblastoma: long-term remission by systemic chemotherapy and
surgery. J Neurooncol 2001; 52:273–276.
24. Hoffman HJ,
Hendrick EB, Humphreys RP. Metastasis via ventriculoperitoneal shunt in patients
with medulloblastoma. J Neurosurg 1976; 44:462– 466.
25. Klimo P Jr,
Goumnerova LC. Endoscopic third ventriculostomy for brainstem tumors. J
Neurosurg 2006; 105(4 suppl):271-274.
26. Steinbok P,
Singhal A, Mills J, Cochrane DD. Cerebrospinal fluid (CSF) leak and
pseudomeningocele formation after posterior fossa tumor resection in children:
a retrospective analysis. Childs Nerv Syst 2007; 23(2):171-174.
27. Sarrazin JL. Tumors of the posterior fossa
(French). J Radiol 2006; 87: 748-763.