ABSTRACT
We
present a case of left superficial temporal artery aneurysm in a sixteen year
old male patient who presented six weeks after sustaining a blunt trauma to the
left temporal region with a pulsatile non tender mass. Duplex study was
performed demonstrating a false aneurysm arising from the temporal artery. Surgical
excision was performed and diagnosis was confirmed. Despite its rarity,
superficial temporal artery aneurysm should be considered when temporal head mass
is evaluated.
Key
words: Aneurysm, Post-traumatic superficial, Temporal Artery
JRMS
August 2008; 15(2): 53-55
Introduction
Aneurysms of the superficial temporal artery are
uncommon with less than 200 cases reported in literature.(1-4)
The first case was described by Bartholin in 1740.(1-5) These
aneurysms are usually the sequalae of blunt or penetrating trauma or surgery to
the fronto-temporal region, although they may arise following infection or
autoimmune diseases.(6) Patients usually present within six
weeks with pulsatile periauricular mass with the majority being false
aneurysms.
In this report, we present a case of superficial temporal
artery aneurysm discussing its presentation, diagnosis and treatment.
Case Report
A sixteen year old male patient was referred to the
vascular surgery unit at Queen Alia Military Hospital six weeks after
sustaining a blunt trauma to his left fronto temporal region after presenting with
a painless temporal mass.
He noticed a progressive
increase in its size over
the
period with occasional ear discomfort especially at night. He did not complain
of headache or visual disturbances. The
patient visited a general surgeon who referred him to vascular surgeon
consultation after a trial of bloody aspiration, as a diagnosis of localized
abscess was considered.
Upon physical examination, a solitary mass at his left
temporal region was observed (Fig. 1). It
was pulsatile, non tender, well defined, 2cm x 2cm in size and with audible
bruit. Skull X-Ray and Duplex U/S were
performed. No skull fracture was noticed
and duplex showed superficial temporal artery mass with turbulent flow, narrow
neck and partial wall thrombosis confirming the diagnosis of superficial
temporal artery pseudo aneurysm (Fig. 2 and 3).
A decision of surgical excision was taken and patient
consent was achieved. Under general anesthesia, a longitudinal incision was
made over the swelling and after identification and ligation of the proximal
and distal parts of the temporal artery; the aneurysm was excised (Fig. 4 and
5).

|
Fig. 1. Left
superficial temporal artery aneurysm
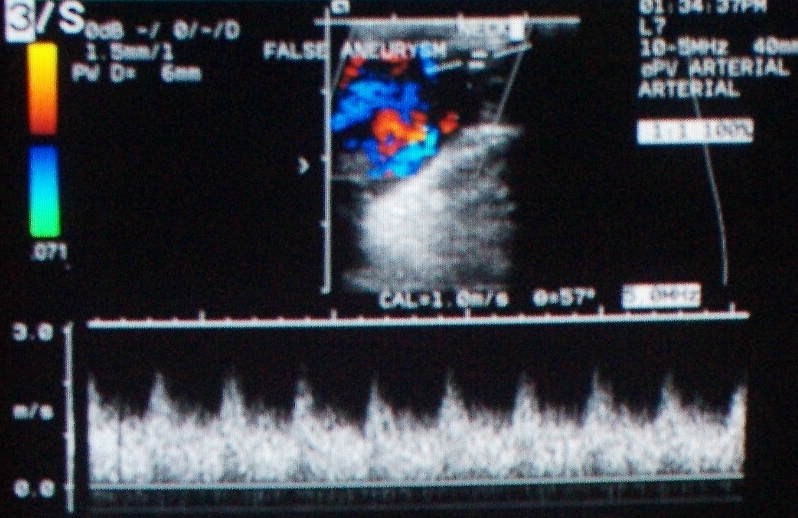
Fig .2. Duplex U/S showing temporal artery false aneurysm with turbulent flow
|
|
|
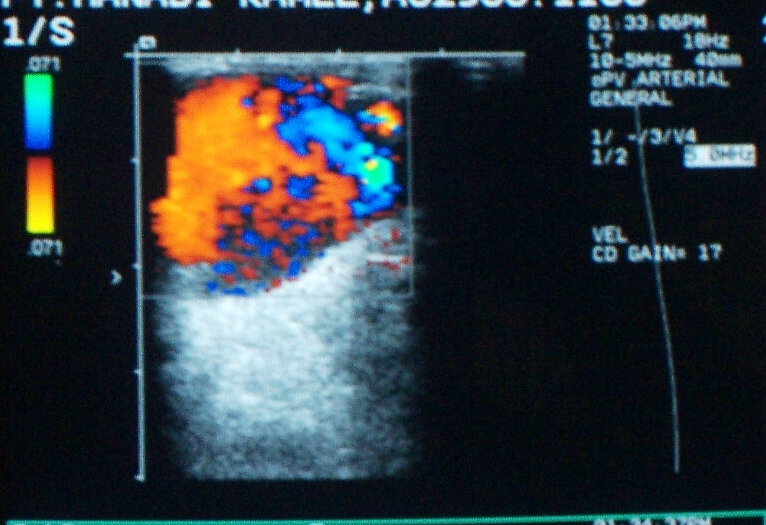
Fig. 3. Duplex
U/S showing false superficial temporal artery aneurysm 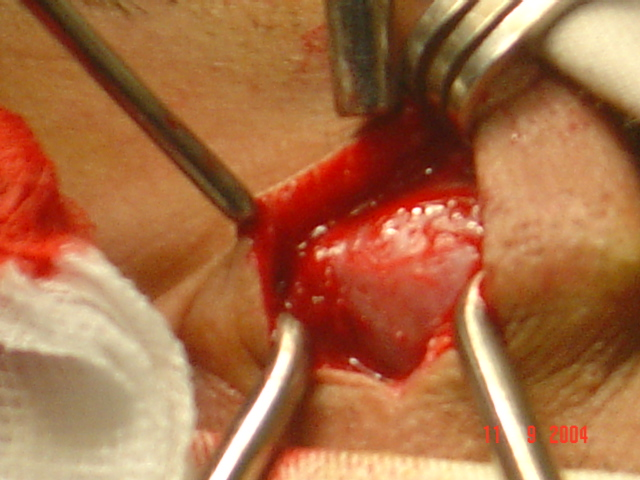
|
|
|
Fig. 4. Excision of superficial temporal artery false aneurysm

Fig. 5.
Ligation of proximal and distal superficial temporal artery and excision of
false |
Discussion
Superficial temporal artery aneurysm is an uncommon
entity being reported in less than 200 cases reviewed
in literature since it was first described in
the 18th century.(1,2,4,5,7)
They constitute less than 1% of all post traumatic aneurysms(3).
The superficial temporal artery is the smaller
terminal branch of the external carotid artery.(8) It runs up
and behind the temporomandibular joint coming in close relation to the trunks
of the facial nerve. It is separated from the skull only by the temporal muscle
and it divides into anterior and posterior branches which supply the skin over
the frontal and temporal regions. It crosses the posterior root of the
zygomatic arch where its pulsation can be felt above and in front of the tragus
of the ear.(3,5) This
relatively exposed course above the base of the parotid gland being uncushioned
by a muscle makes this artery vulnerable to trauma and injury.(3,5) Periarterial hematoma following incidental or iatrogenic
trauma is the beginning of the event.(2,3,5)
It results in partial or complete injury or necrosis
of the arterial wall. The hematoma remains in connection with the arterial
lumen. Later, when the thrombotic part is reabsorbed, the cavity provides a
space for the arterial blood to circulate. Thus creating a false aneurysm
surrounded by a pseudo capsule.
A history of trauma especially within the last two to
six weeks is the corner stone in the diagnosis.(1,2,5) It
constitutes the origin in the vast majority of superficial temporal artery
aneurysms. Trauma can be incidental or iatrogenic following craniotomies, external
ventricular drainage, temporomandibular joint excision arthroplasty and punch
hair grafting.(4,9)
A pulsatile mass in the pre-auricular area is the
clinical scenario. The pulsation can be controlled by compression of the
superficial temporal artery proximally. It is associated with headache, ear
discomfort and occasional visual disturbances, dizziness and hemorrhage.(1,7,9,10)
Invasive and non invasive modalities are used to
confirm the diagnosis, for surgical planning and to exclude other causes. These
include Duplex U/S, CT angiogram, MR angiogram and conventional angiogram.(2,4)
Differential diagnosis of superficial temporal artery aneurysm includes
vascular tumors, middle meningeal artery aneurysm, hematoma, abscess, neuromas,
soft tissue tumors, foreign body granulomas and epidermoid inclusion cyst.(4,5)
Treatment is indicated in relieving symptoms, preventing
bleeding and for cosmoses.(3,5) Although different successful
modalities were described including conservative management by compression, endovascular
embolization and percutaneous injection of thrombin, surgical excision of
pseudo aneurysm with ligation of afferent and efferent vessels under local or
general anesthesia remains the treatment of choice with excellent results.(2,3,5,6)
Special care must be considered for the anatomy of the temporal region
especially in proximally located aneurysms to prevent injury of the parotid
gland and its duct as well as the different branches of the facial nerve.
Conclusion
Although rare, superficial temporal artery aneurysm
should be considered in temporal head mass evaluation especially when history
of trauma is reported. Simple excision and ligation are usually curative.
References
1. Sanz HMA,
Pol NB, Perez JRS. Post traumatic aneurysm of the superficial temporal
artery, a reported case. Journal of Vascular
Surgery 1998; 27: 374-377.
2. Shenoy SN, Raja A. Traumatic superficial temporal artery aneurysm: case
report. Neural India 2003; 51: 537 -538.
3. Partap VA,
Cassoff J, Glikstein R. US -
guided percutaneous thrombin injection: A new method of repair of superficial
temporal artery pseudo aneurysm. Journal of Vascular & International
Radiology 2000; 11: 461-463.
4. Walker MT,
Liu BP, Salehi SA, et al. Superficial temporal artery pseudoaneurysm: diagnosis & pre
operative planning with CT Angiography. American Journal of Neuroradiology
2003; 24: 147-150.
5. Leal FSCB, Miranda CCV, Guimaraes ACA. Traumatic
pseudoaneurysm of the superficial temporal artery: Case report. Arq.Neuro-Psiquiatr
2005; 63(3): 25-26.
6. Isaacson G, Kochan PS, Kochan JP. Pseudoaneurysm
of the superficial temporal artery: treatment options. Laryngoscope 2004;
114 (6): 1000- 1004.
7. Magloire
DF, Reyes CR, Magloire MP. Right superficial
temporal artery aneurysm. Case report. Rev Mex Angiol 1999; 27 (2): 41- 44.
8. McMinn RMH. Head & neck & spine. Last‘s Anatomy.9th
edition. Longman Group UK
limited 1994; 454- 455.
9. Amlashi SFA, Riffaud L, Morandi X. Arteriovenous fistula of the superficial temporal
artery: an exceptional complication of the pterional approach. Journal of Neurology
Neurosurgery and Psychiatry 2004; 75: 1077 - 1078.
10. Asakura K, Tasaki T, Okada K. A case of
unruptured anterior temporal artery aneurysm showing pupil sparing oculomotor
palsy. No Shinkei Geka 1986; 14 (6): 777-782.