Abstract
We report a case
of glucagonoma in a 60-year old diabetic lady who was seen by a dermatologist
for a superficial erythematous skin eruption with flaccid bullae over both legs
of recent onset. These findings warranted further investigations that revealed
a pancreatic mass lesion involving the distal body and tail with three
metastatic deposits within the right lobe of the liver. Distal pancreatectomy
and splenectomy were performed and histological examination of the excised
specimen confirmed the diagnosis of pancreatic glucagonoma with liver
metastasis. Blood sugar levels became more controlled postoperatively. The skin
lesion disappeared completely six months after surgery. The lady enjoys fairly good
health, and is maintained on Somatostatin analogues for control of metastasis
that are stable after 18 months of follow up.
Key words: Diabetes mellitus type II, glucagonoma,
necrolytic migratory erythema
JRMS
August 2009; 13(2): 47-50
Introduction
Glucagon
is a 29 amino acid peptide secreted by the pancreatic alpha cells in islets of
Langerhans. Its main effect is to keep normal blood glucose levels
counteracting the actions of insulin. Pharmacological administration of
glucagons is effective in the treatment of hypoglycemia but extrahepatic
effects are also well known.(1) Glucagonoma is a rare neuroendocrine tumor
arising from alpha islet cells of the pancreas,(2) it is
extremely rare but well-known with a current prevalence estimated at 1/20
millions.(3) Glucagonoma is associated with a characteristic
syndrome caused by glucagon hypersecretion. Patients typically present in their
fifth or sixth decade. Classical clinical features of glucagonoma syndrome
include: diabetes mellitus, cheilitis, normocytic anemia, painful glossitis, gastrointestinal
disturbances, thromboembolism and weight loss.(4) The
characteristic skin manifestation is necrolytic migratory erythema, which is an
erythematous painful and pruritic rash. It begins as macules that coalesce and
develop central bullae before eroding and leaving hyperpigmentation and crusts
at the periphery.(5) Necrolytic migratory erythema usually
starts at the perirectal area and subsequently spread to the perineum,
buttocks, thighs, and lower extremeties. It is a pathognomonic feature of glucagonoma.(6)
Necrolytic migratory erythema is typically characterized on skin biopsies by
|
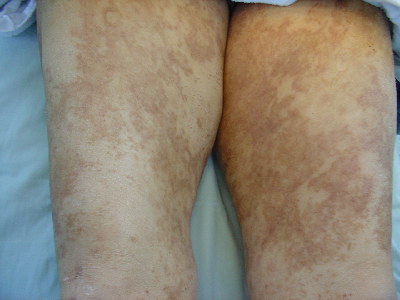
Fig.
1A. Showing
the necrolytic migratory erythema on lower limbs
|
|

Fig.
1B. Showing
the pancreatic lesion and the metastatic lesions in liver
|
|
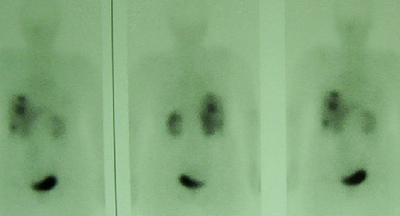
Fig.
1 C. Octreotide
scan showing the three metastatic lesions in the liver
necrolysis of the upper
epidermis with vacuolated keratinocytes.(7) Glucagonoma
usually becomes evident within 1-2 years of developing diabetes mellitus. We present
here a rare case of glucagonoma presenting with a typical skin eruption in a
lady with long standing Type 2 DM that became more controlled after tumor removal. |
Case Report
A 60
year old Jordanian lady, a mother of 11 children, consulted her doctor for an
itchy erythematous skin rash that started over both feet, then extended up to
the gluteal area over a two weeks period. She lost eight kilograms of body
weight in the last four months prior to presentation. The patient has had type II
diabetes for the past 10 years and essential hypertension for the last five
years. She had no history of surgeries or allergies. She smokes 20 cigarettes a
day since the age of 30. Her current medications include: Glibenclamide 5mg
bid, Metformin 850mg bid and Enalapril 5mg bid. Clinical evaluation revealed a
middle aged lady
|
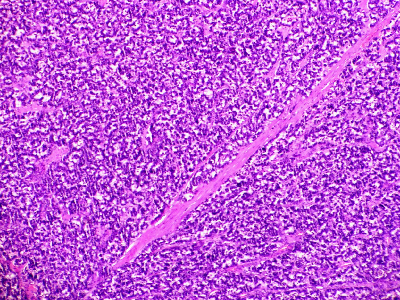
Fig.
2A.
Glucagonoma and normal pancreatic tissue (Right of the picture) 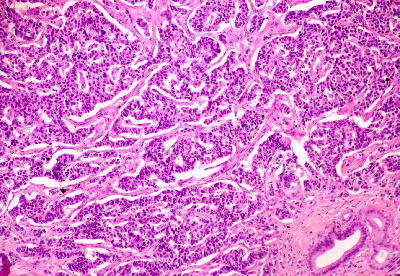 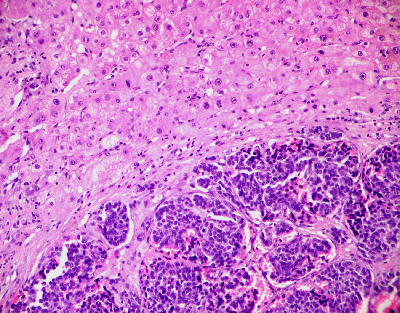
|
|
2B
2C
Fig. 2B. The tumor arranges in
trabecular and gland-like growth pattern (composed of small, round, uniform
cells with hyper chromatic nuclei and scant granular eosinophilic cytoplasm),
Fig. 2C. Liver with metastatic glucagonoma
|
|
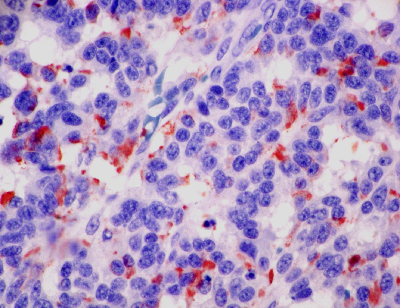
Fig.
2D. Tumor
cells reactive for chromogranin
with pale conjunctivae, blood
pressure of 136/88 mmHg, no goiter and no palpable abdominal organs or masses.
Examination of the lower limbs showed an erythematous rash over the posterior
aspect of both lower limbs from the heels upward to the gluteal region with
superficial flaccid bullae and minute pustules, scratch marks were also seen (Fig.
1A). |
She was treated initially with
systemic as well as topical antibiotics and antihistamines but without
improvement. Laboratory work up revealed normochromic normocytic anemia, normal
other blood counts, normal liver and kidney function tests.
The glucagon level
was not done due to laboratory factors, her diabetes was uncontrolled with
glycosylated hemoglobin of 10.6%. Scraping of the skin rash showed no evidence
of bacterial or fungal overgrowth.
Radiological imaging showed a normal chest
X-ray, abdominal ultrasound followed by computerized tomography scan revealed a
well defined lobulated, heterogeneously enhancing soft tissue mass lesion
arising from the distal body and tail of the pancreas measuring 5.5x4.5x3 centimeters,
partially encasing the splenic vessels and indenting the posterior aspect of
the fundus of the stomach. There were also three metastatic deposits in the
right lobe of the liver (Fig. 1B) which were confirmed by octreotide liver scan
(Fig. 1C).
The
lady underwent surgery with excision of the spleen and distal part of the
pancreas. Histopathological examination confirmed the diagnosis of glucagonoma
(Fig. 2A, 2B, 2C, 2D).
Follow
up visit at six months post surgery showed complete disappearance of the rash
and controlled blood sugar (HbA1c 6.8%). She enjoys a good health, kept on
twice monthly intramuscular injections of somatostatin analogue (Lanreotide LA
30mg) as well as one tablet of glibenclamide 5mg and antihypertensive drugs.
She is under close follow up. Octrotide scan after one year showed stable liver
metastases with no new lesions.
Discussion
Glucagonoma
is a rare neuroendocrine tumor of the pancreatic α islet cell associated with
characteristic syndrome caused by hypersecretion of glucagon. Glucagonoma is
often found in the pancreatic body and or tail and is usually large enough to
be localized by computed tomography.(8) It is often both well
developed and malignant at detection.(9) Necrolytic migratory
erythema is a characteristic skin
condition seen in the presence of pancreatic glucagonoma.(10) The
presence of necrolytic migratory erythema in the absence of a pancreatic tumor
has been termed the pseudoglucagonoma syndrome. In such cases, necrolytic migratory erythema is
commonly associated with conditions, such as liver disease, pancreatitis and
malabsorption disorders (celiac disease). There are many theories on the
pathogenesis of necrolytic migratory erythema, which include the direct action
of glucagon in inducing skin necrolysis, a nutritional or metabolic deficiency
of zinc or essential fatty acids and glucagon induction of inflammatory
mediators.(10) While some improvement of this dermatosis was
reported with aminoacid or zinc repletion, almost invariable disappearance of
the erythema is the rule after successful removal of the glucagon-producing
tumor.(11,12)
Surgery
is the main component of the treatment of glucagonoma and in some cases in
association with chemotherapy.(13) Chemoembolization is
another option for treatment of metastasis in lesions not amenable for surgery.
Early recognition of necrolytic migratory erythema, a clinical feature that may
appear in patients with glucagonoma, can lead to possible cure, whereas delayed
identification of the disease is associated with metastatic disease and poor
prognosis.(9)
Conclusion
As
diabetes became well controlled after removal of the glucagonoma tumor, we
speculate that glucagonoma tumor is a contributing cause for uncontrolled
diabetes in this case. The tumor was discovered in metastatic stage that needed
aggressive approach of treatment to obtain best control of disease.
References
1. Pollck CV Jr. Utility of glucagons in the
emergency department. J Emerg Med 1993; 11: 195-205.
2. Bouin M,
Aoustin LD. Clinical response of an atypical glucagonoma treated with long acting
somatostatin analog. Gastroenterol Clin Biol 2002; 26(10): 926-929.
3. Echenique-Elizondo M, Tuneu Valls A, Elorza Orue JL, et
al. Glucagonoma
and pseudoglucagonoma syndrome. JOP 2004; 5(4): 179-185.
4. Chastain MA. The glucagonoma syndrome: A
review of its features and discussion of new prospectives. Am J Med Sci
2001; 321: 306-320.
5. Johnson SM,
Smoller BR, Lamps LW, et al. Necrolytic migratory erythema as the only
presenting sign of a glucagonoma. J Am Acad Dermatol 2003; 49: 325-328.
6. Du Jardin P,
Cools P, Van der stighelin Y. Necrolytic migratory erythema: first symptom of
glucagonoma. A case report. Acta Chir Belg 2004; 104(4): 468-470.
7. Van Beek AP, de Haas ER, van Vloten WA, et al. The glucagonoma syndrome and
necrolytic migratory erythema: a clinical review. Eur J Endocrinol 2004; 151(5): 531-537.
8. Chen HW, Su
DH, Shun CT, Liu KL. Rare presentation of endocrine pancreatic tumor: a case of diffuse
glucagonoma without metastasis and necrolytic migratory erythema. J Formos
Med Assoc 2005; 104(5): 363-366.
9. Randy P, Eigentler TK, Soennichsen K, et al. Metastatic glucagonoma:
treatment with liver transplantation. J
Am Acad Dermatol 2006; 54(2): 344-347.
10. Tierney EP,
Badger J.
Etiology and pathogenesis of necrolytic migratory erythema: review of the literature. Med Gen Med 2004; 10; 6(3): 4.
11. Von Schenk H, Thorell JI, Berg J, et al. Metabolic studies and glucagons
gel filtration pattern before and after surgery in a case of glucagonoma
syndrome. Acta Med Scand 1979; 205(3):155-162.
12. Marynick SP, Fagadau WR, Duncan LA. Malignant glucagonoma syndrome:
Response to chemotherapy. Ann Inter Med 1980; 93(3):453-454.
13. Pautrat K, Bretagnol
F, de Muret A, de Calan L. Recurrent glucagonoma 20 years after surgical resection.
Gastroenterol Clin Biol 2003; 27(12): 1163-1165.