Abstract
Objective: The objective of the study was to look at the effect
of using ß-blockers perioperatively in patients undergoing coronary artery
bypass graft surgery at Queen Alia Heart Institute.
Methods: This is a retrospective analysis of all patients who
underwent coronary artery bypass graft surgery between April 2005 and September
2006 at Queen Alia Heart Institute. The data collected included the patients' demographic
characteristics, risk factors for coronary artery disease, history of
myocardial infarction, renal dysfunction, history of prior cardiac surgery and
the nature of coronary artery disease. We assessed operative mortality, rate of
stroke, atrial or ventricular arrhythmias, duration of ventilatory support and Intensive
Care Unit stay. Inclusion criteria were
adult patients who were admitted for coronary artery bypass graft surgery, excluding
patients who had valvular surgery, aneurysmectomy and off pump bypass surgery.
Results: We
had a total of 916 patients. Four hundred and ten patients were on b-blockers while the rest were not. The two groups did
not differ in their characteristics. The mean age was 60.0 ± 11 years, with 24%
females. The mean Intensive Care Unit stay was 1.8 ± 0.5 days for the b-blockers group and 2.0 ± 0.6 days for the non-b-blockers group (P=0.001). Patients who had b-blockers had a rate of atrial or ventricular
arrhythmias of 26% compared to 38% in the non-b-blockers group (P=0.001). The mean post-operative hospital stay for
patients who received b-blockers was 7.2 ± 3 days compared to 8.4 ± 3.2 days in the non-b-blockers group (P<0.001). In-hospital mortality
was 4.2% in the b-blockers group and 5.3% in the non-b-blockers group (P=NS). Stroke was seen in 2.1% in the
first group compared to 3.3% in the non-b-blockers group (P=NS). Ventilatory support for more
than 24 hours was seen in 7.1% compared to 6.9% in the non-b-blockers group (P=NS). Intra-Aortic Balloon Pump
support was used in 4.9% compared to 5.2% in the non-b-blockers group (P=NS).
Conclusion:
Perioperative b-blockers use is associated with significantly lower
incidence of arrhythmias, shorter hospital stay and non-significant lower in-hospital
mortality. They had no effect on ventilatory support or the use of intra-aortic
balloon pump support.
Key words: Coronary artery disease, Coronary bypass, Jordan.
JRMS December 2009; 16(3): 42-46
Introduction
ß-Blockers are one of the oldest and most commonly used
drugs for the treatment of ischemic heart disease.(1) They
have been shown to improve acute outcomes and long term prognosis in ischemic
heart disease(2-4) and to reduce perioperative events
among high risk patients undergoing major non-cardiac and vascular surgery.(5-8)
Prior ß-blocker therapy has also been shown to have a
cardio-protective effect in limiting CK-MB release and lower
intermediate term mortality rate following percutaneous coronary interventions.(9)
Interest is now concentrating on exploring this beneficial effect in
patients undergoing Coronary Artery Bypass Graft (CABG) surgery. Most of the
evidence comes from extrapolations of the cardioprotective benefits of b-blockers from major noncardiac and vascular surgery. Operating
on a ß-blocked heart is controversial with concerns arising
about the negative inotropic effect of ß-blockers and complications of ß-blockade
like bronchospasm.(10-13)
Accordingly, many cardiac surgeons have not considered use of b-blockers perioperatively in their CABG patients.
The aim of this study was to quantify the effect of preoperative b-blocker therapy continued to the day of surgery and
postopeatively on outcome, morbidity and mortality following coronary artery
bypass grafting in the patient population at Queen Alia Heart
Institute (QAHI).
Methods
This was a retrospective analysis of all patients who had CABG surgery between
April 2005 and September 2006 at Queen Alia Heart Institute. The data collected
included the patients' characteristics, risk factors for coronary artery
disease (CAD), history of myocardial infarction (MI), renal dysfunction, and
history of prior cardiac surgery and the nature of CAD. We assessed operative
mortality, rate of stroke, atrial and ventricular arrhythmias (atrial
fibrillation, flutter, ventricular tachycardia or ventricular fibrillation),
duration of ventilatory support, use of intra-aortic balloon pump (IABP)
support and Intensive Care Unit (ICU) stay.
Inclusion criteria were adult patients who were admitted for CABG
surgery, excluding patients who had valvular surgery, aneurysmectomy, off pump
bypass and those who had concurrent carotid endarterectomy.
Electrocardiographic monitoring was done continuously during ICU stay
and at least daily ECG or more often upon the discretion the treating surgeon
once the patient was back on the ward. Definition
of risk factors was similar to criteria set in the Euro Heart Survey of
patients with Acute Coronary Syndromes.(14) Current smoking
was defined as smoking up to one month before surgery. Hypertension was defined
as prior diagnosis, current use of antihypertensive medications or blood
pressure readings of > 140 mmHg systolic or > 90 mmHg diastolic on more
than two occasions. Diabetes was defined as prior diagnosis or current use of
hypoglycemic medications. Hypercholesterolemia was defined as total cholesterol
of > 200 mg/dl, or current use of cholesterol lowering treatment. Renal
dysfunction was defined as creatinine of > 1.5 mg/dl.
Perioperative β-blocker was defined as the use of β-blocker
preoperatively on admission that was continued post-op either intravenous or
orally upon the discretion of the treating surgeon up to hospital discharge.
Statistical methods included the use of Office Excel and Student t test
to calculate the various variables and statistical significance.
Results
We had a total of 916 patients. Four hundred and ten patients were on b-blockers (45%), while the rest were not (Fig. 1).
Table I shows patients' and disease characteristics based on
preoperative use of ß-blocker. The two groups did not differ in their
characteristics. The mean age was 60.0 ±
11 years, 59.0 ± 11.6 years for males and 63.1 ± 9.6 years for females (P =
0.001). Females accounted for 24% of our study population (Fig. 2). 31% had
previous MI, 40.8% had diabetes mellitus and the same percentage was hypertensive.
Almost two thirds (61%) were smokers.
Hypercholesterolemia
was present in 29.4% of patients. Fig 3 shows the prevalence of the various
risk factors for coronary artery disease. The prevalence of risk factors was
95% for at least one risk for CAD to be present. Two risk factors were present
in 28% and three risk factors were present in 20%. Three percent had renal
dysfunction. More than 85% had three vessel diseases and 12.5% had significant
left main disease. 3.8% had prior CABG surgery.
The mean ICU stay was significantly shorter for the β-blocker group at 1.8
± 0.5 days compared to 2.0 ± 0.6 days for the non-b-blockers group (P=0.001). Patients who had b-blockers had a rate of atrial or ventricular
arrhythmias of 26% compared to 38% in the non-b-blockers group (P=0.001).
The mean cross clamp time
was 45 minutes and a mean bypass time of 90 minutes, without a significant statistical
difference between the two groups. The mean post-operative hospital stay for
patients who received b-blockers was 7.2 ± 3 days compared to 8.4 ± 3.2 days in the non-b-blockers group (P<0.001).
In-hospital mortality was 4.2% in the b-blockers group and 5.3% in the non-b-blockers group, 20% reduction of hospital mortality (P=NS). Stroke was seen in 2.1% in the first group compared to 3.3% in the non-b-blockers group (P=NS). Ventilatory support for more than 24 hours was seen in 7.1% compared to 6.9% in the non-b-blockers group (P=NS). Intra-Aortic Balloon Pump (IABP) support was used in 4.9% compared to 5.2% in the non-b-blockers group (P=NS).

Fig. 1.
Percentage of patients using B blockers
Fig. 2. Gender distribution
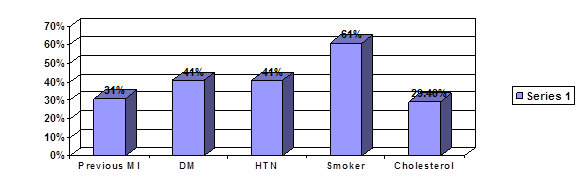
Fig. 3. The prevalence of the various risk factors for CAD
Discussion
Patients requiring CABG surgery
usually have severe coronary artery disease (CAD) and the perioperative course
is characterized by surgical stress and hemodynamic changes. Also, many of the
regular medications are discontinued or interrupted, thus exposing the patient
to their withdrawal effects.
The high prevalence of risk
factors reported here is similar to those reported by similar studies in Jordanian
patients and international studies.(15,16)
Recommendations
for a national campaign fo cessation of smoking and measures to reduce the prevalence
and control of diabetes and hypertension are warranted.
To our
knowledge this analysis is the first at our centre and nationally. To date,
there have been no randomized trials evaluating preoperative b-blockade in CABG surgery.
Table I. Patients' characteristics in the two groups
|
|
ß-Blocker group
|
Non-ß-Blocker group
|
P value
|
|
Age
|
60.3 ±10.9
|
59.8 ±11.1
|
NS
|
|
Female
gender %
|
24
|
|
|
|
Previous
MI %
|
31.7
|
30.6
|
NS
|
|
Current
smoker %
|
62
|
60
|
NS
|
|
Diabetes %
|
40
|
41.5
|
NS
|
|
Hypertension %
|
40.2
|
41.3
|
NS
|
|
Hypercholesterolemia
%
|
28.5
|
30
|
NS
|
|
Renal
dysfunction %
|
3.1
|
2.9
|
NS
|
|
Three
vessel disease %
|
85
|
86
|
NS
|
|
Left main
stenosis %
|
12
|
13
|
NS
|
|
Prior
cardiac surgery %
|
3.9
|
3.8
|
NS
|
|
Emergency
procedure %
|
2
|
2.2
|
NS
|
|
Number of
grafts per patient
|
3.5
|
3.4
|
NS
|
|
LIMA use %
|
90
|
89.5
|
NS
|
NS =
non-significant
Table
II. In-hospital outcome
|
|
ß-Blocker users
|
Non-ß-blocker users
|
P Value
|
|
Mean ICU
stay (days)
|
1.8 ± 0.5
|
2.0 ± 0.6
|
0.001
|
|
Post
operative arrhythmias %
|
26
|
38
|
0.001
|
|
Mean
hospital stay (days)
|
7.2 ± 3
|
8.4 ± 3.2
|
0.001
|
|
In-hospital
mortality
|
4.2
|
5.3
|
0.50
|
|
Stroke
(%)
|
2.1
|
3.3
|
0.371
|
|
Ventilation
>24 h (%)
|
7.1
|
6.9
|
0.50
|
|
IABP
support (%)
|
4.9
|
5.2
|
0.50 |
In our study 44.8% had preoperative b-blocker therapy that was continued postoperatively.
This figure is less than that quoted in international studies of 65%.(13)
We have shown the beneficial effect of preoperative b-blockers that is continued postoperatively, on ICU
stay, rate of atrial arrhythmias, postoperative hospital stay and a
statistically non significant reduction of hospital mortality (20%).
Investigators have suggested improved survival with the use of b-blockade perioperatively.
Ferguson et al.(13) have
looked at outcomes after cardiac surgery in a large multi-centre
observational study in North America.
Their analysis shows that preoperative ß-blockade improved operative
survival in all patients who underwent coronary artery surgery
except in those with poor left ventricular function (<30%). It
has also been shown that these patients also have significantly
lower rates of stroke, renal failure, and prolonged ventilation. The
literature reports a rate of 5-40% incidence of atrial arrhythmias post CABG
surgery.(17)
Several studies have shown that initiation of b-blocker therapy preoperatively reduces the incidence
of atrial fibrillation in CABG patients.(18,19) Lower stroke
rate is attributed to having a high lipid solubility, thus crossing the blood
brain barrier and reduction of ischemia by shifting the oxygen-haemoglobin
dissociation curve to the right resulting in increased oxygen dissociation to
brain tissues.(17) The high levels of circulating
catecholamines result in desensitization and reduction in the density of b-adrenoceptors. This leads to abnormal response to
epinephrine and norepinephrine and compounding ischemia.(20,21)
Other postulated mechanisms are membrane stabilization and local anaesthetic
effects of b-blockers.
Ferninger et
al.(22) identified a lower heart rate at the time of
anaesthesia induction for CABG to predict perioperative events and suggested
that the potential benefit of b-blocker therapy to be due to its autonomic effects. Chen et al.(23)
reported that elderly CABG patients discharged receiving b-blockers had improved one year adjusted survival
rates compared with those not receiving b-blockers.
Other postulated mechanisms suggest that catecholamines instigate and
perpetuate vascular injury by promoting endothelial dysfunction, platelet
aggregation, endovascular adhesion molecule release, hypercoaguability,
hypertension and direct myocyte toxicity. β-adrenergic blockade, experimentally
and epidemiologically, can reverse many of these effects.(24)
Conclusion
Our analysis provides evidence that use of b-blockers is safe and effective in CABG surgery patients.
Peri-operative b-blockers use is associated with significantly lower incidence of
arrhythmias, shorter hospital stay and non-significantly lower in-hospital
mortality. They had no significant effect on ventilatory support or the use of
IABP support.
References
1.
Ryan
TJ, Antman EM, Brooks NH, et al. 1999 update: ACC/AHA guidelines for the management of
patients with acute myocardial infarction. A report of the American College of
Cardiology/American Heart Association Task Force on Practice Guidelines
(Committee on Management of Acute Myocardial Infarction). J Am Coll Cardiol
1999; 34:890–911.
2.
Chen
J, Radford JM, Wang Y, et al. Are b-Blockers Effective in
Elderly Patients Who Undergo Coronary Revascularization After Acute Myocardial
Infarction? Arch Intern Med. 2000; 160:947-952.
3.
Packer
M, Coats AJ, Fowler MB, et al. Effect of carvedilol on survival in sever congestive heart failure. N
Engl J Med 2001; 344:1651-1658.
4.
Farrell
MH, Foody JM, Krumholz HM. ß-Blockers in heart failure. J Am Med Assoc
2002; 287:890–897.
5.
Wallace
A, Layug B, Tateo I, et al. Prophylactic atenolol reduces perioperative myocardial ischemia. Anesthesiology
1998; 88:7-17.
6.
Mangano
DT, Layug EL, Wallace A, Tateo I. Effect of atenolol on mortality and cardiovascular morbidity after
noncardiac surgery. N Engl J Med 1996;
335:1713-1720.
7.
Poldermans
D, Boersma E, Bax JJ, et al. The effect of bisoprolol on perioperative mortality and myocardial
infarction in high-risk patients undergoing vascular surgery. N Engl J Med 1999; 341:1789-1794.
8.
Lindenauer
PK, Pekow P, Wang K, et al. Perioperative Beta-Blocker Therapy and Mortality after Major Noncardiac
Surgery. N Engl J Med 2005; 353:349-61.
9.
Sharma SK, Kini A, Marmur JD, Fuster V. Cardioprotective effect of prior ß-blocker
therapy in reducing creatine kinase-MB elevation after
coronary intervention. Circulation 2000; 102:166–172.
10. Whorlow SL, Krum H. Meta-analysis of effect of ß-blocker therapy on
mortality in NYHA Class IV chronic heart failure patients. Am J Cardiol
2000; 86:886–889.
11. Gottleib SS, McCarter RJ, Vogel RA. Effect of beta-blockade on mortality among high risk
and low risk patients after myocardial infarction. N Engl J Med 1998; 339:489-497.
12. Weightman WM, Gibbs NM, Sheminant MR, et
al. Drug therapy before
coronary artery surgery: nitrates are independent predictors of mortality and
beta-adrenergic blockers predict survival. Anesth Analg 1999; 88:286–291.
13. Ferguson TB Jr., Coombs LP, Peterson
ED. Preoperative ß-blocker use
and mortality and morbidity following CABG surgery in North
America. J Am Med Assoc 2002; 287:2221–2227.
14. Hasdai D, Bear S, Wallentin L, et
al. A prospective survey of
characteristics, treatments and outcome of patients with acute coronary
syndromes in Europe and the Mediterranean basin.
The Euro Heart Survey of Acute Coronary Syndromes (Euro Heart Survey ACS). Euro
Heart J 2002; 23:1190-1201.
15. Hammoudeh A, AL-Tarawneh H, Elharasis
A, et al. Prevalence of
conventional risk factors in Jordanians with coronary heart disease: The Jordan
Hyperlipidemia and Related Targets Study (JoHARTS). International J Card
2006; 110: 179-183.
16. Magnus P, Beaglehole R. The real contribution of the major risk factors to the
coronary epidemics : time to end the "only 50 %" myth. Arch Intern
Med 2001; 161: 2657-2660.
17. Amory DW, Grigore A, Amory JK, et
al. Neuroprotection is
associated with beta-adrenergic receptor antagonists during cardiac surgery:
evidence from 2.575 patients. J Cardiothorac Vasc Anesth 2002; 16:270–277.
18. Andrews TC, Reimold
SC, Berlin
JA, Antman EM. Prevention of
supraventricular arrhythmias after coronary artery by pass surgery: a
meta-analysis of randomized control trials. Circulation 1991; 84 (Suppl
III):III236–III244.
19. Grigore AM, Armory DW, White WD. b-Blockade and neurological outcome in cardiac surgery. Anesth Analg
1999; 88: (Suppl 4S):89.
20. Schwinn DA, Leone BJ, Spahn DR, et
al. Desensitization of
myocardial beta-adrenergic receptors during cardiopulmonary bypass. Evidence
for early uncoupling and late down regulation. Circulation 1991; 84:2559-2567.
21. Selke FW, Wang SY, Stamler A, et al. Cardiopulmonary bypass,
myocardial management, and support techniques, changes in autonomic response of
cerebral circulation after normothermic extracorporeal circulation. J Thorac Cardiovasc Surg 1996; 112:450-461.
22. Ferninger M, Surgenor SD, Dodds TM, et
al. Treatment of
pre-induction tachycardia with beta-adrenergic blockade reduces mortality after
CABG. Anaesthesiology 2001; 95: A 2500.
23. Chen J, Radford MJ, Wang Y, et al. Are beta-blockers effective in elderly patients who
undergo coronary revascularization after acute myocardial infarction? Arch
Intern Med. 2000; 160:947-952.
24. Selzman CH, Miller SA, Zimmerman MA,
Harken AH. The case of β-adrenergic
blockade on prophylaxis against perioperative cardiovascular morbidity and
mortality. Arch Surg 2001; 136:286-290.