Abstract
Objective: Obstructive
pattern within hydronephrotic non-obstructed kidney is frequently encountered
during 99mTc-MAG3 diuretic renography. The
aim of this study was to assess the value of applying new protocol and criteria
on dual-time imaging in ruling out obstruction.
Methods: We
included 53 children (56 kidneys) in this study (28 boys and 25 girls with age
range three weeks to 12 years). All had
hydronephrosis, which was bilateral in three children. Eighteen children had
pyeloplasty, while 35 children had no previous surgical interventions. All children
were referred for assessment of renal outflow obstruction and kidney function.
All children underwent routine diuretic 99mTc-MAG3 renal renography.
All had obstructive patterns during diuretic 99mTc-MAG3 renography
and underwent a second dynamic study 30 minutes later for 10 minutes. Non obstructive
criteria were set as down sloping second time renogram with drop of kidney
counts by ≥ 30% during the 10 minute second time renogram, or flat renogram but
with drop of kidney counts by > 50% of peaked activity in first time
renogram. Obstructive criteria on dual-time imaging were set as progressive
rising second time renogram or flat second time renogram with drop of kidney
counts by less than 30% compared to first time study. Equivocal criteria were set
as flat renograms with drop of kidney activity by 30-50% or down sloping
renogram with drop of kidney counts by < 30% over 10 minutes.
Results: Non
obstructive patterns were noticed in 16 kidneys 15 (patients), with down
sloping curves during second time renograms in seven kidneys and flat second
time renogram with drop of activity by > 50% in 9 kidneys. Obstructive
patterns on dual time point 99mTc-MAG3
renography were noticed in 31 kidneys (29 patients). Eleven kidneys (six
patients) were false positive, since three patients had neurogenic bladder with
no obstruction, two patients had long standing severe hydronehrosis with no
obstruction and one patient had glomerulonephritis. Equivocal patterns were noticed in nine
patients, four of them were turned to have significant obstruction, while five
had no obstruction.
Conclusion: Dual-time 99mTc-MAG3 diuretic renography
can increase the efficiency in differentiating between obstructed and non-obstructed
hydronephrosis compared to routine single time study.
Key
words: 99mTc-MAG3,
Diuretic renograph, Hydronephrosis, Obstructive uropathy
JRMS
December 2009; 16(3): 47-54
Introduction
The distinction between renal outflow
mechanical obstruction and dilation not associated with obstruction
is critical to patient management.(1) 99mTc-MAG3 diuretic renography is an
established method for investigation of hydronephrosis. The renogram
pattern during 99mTc-MAG3 diuretic renography is
usually related to the degree of obstruction; an non-obstructed
system is easily assessed by prompt tracer washout, whereas in
cases of obstruction, washout after diuretic remains slow and there
will be prolonged retention of the radiopharmaceutical resulting in
raising curve.(1-3)
However, obstructive pattern in non-obstructed hydronephrotic kidney is
frequently encountered
during diuretic
renography,(1,4-8)
and early differentiation between non-obstructed and obstructed kidney without follow
up scanning can be considered a diagnostic challenge in a lot of cases.
We conducted this study
to assess the added information achieved by performing delayed (second time) renography.
Our aim was to try to differentiate between obstructed and non-obstructed
hydronephrotic kidneys, by setting new criteria depending on second time renography
findings.
Methods
This study was conducted in the nuclear
medicine division at King Hussein hospital, in the period between August 2006 and
October 2007. Fifty three children with 56 hydronephrotic kidneys were included
in this study (28 boys and 25 girls with age range three weeks to 12 years).
All children had hydronephrosis and three had bilateral hydronephrosis.
Eighteen children had pyeloplasty, while 35 had no previous surgical
interventions. All patients were referred for assessment of renal outflow
obstruction and function. All patients underwent routine 99mTc-MAG3 diuretic renography. All
patients had obstructive patterns (upsloping renogram) during routine diuretic 99mTc-MAG3 renography.
Routine 99mTc-MAG3 diuretic renography was
performed following the standardized protocol, and bladder
catheterization was not performed. All patients were hydrated by oral fluids
before the injection of 99mTc-MAG3. Furosemide (1mg/kg)
was intravenously administered 15 min before the injection of 99mTc-MAG3 radiopharmaceutical
(F-15 protocol). We administered about
1.85 MBq/kg (50 µCi/kg) 99mTc-MAG3 and a minimum
dosage of 37 MBq (1mCi) intravenously. All patients tolerated the
procedure well and all acquisitions were conducted without the use of sedation.
Movement was minimized by using ribbons in addition to the assurance effect of parents
near the child. Dynamic study was set as two second/frames for the first minute
followed by one min/frame for 20 minutes.
For measurement of
differential renal function and renogram generation, regions of
interest were drawn over the entire kidney and background on each
side. The kidney background was manually drawn on 1-2 minute images
in a crescent shape over the outer aspect of the kidney. All
patients underwent second time dynamic study, conducted 30 minutes later (50
minutes after radiotracer injection). This time was set to allow performing the
new study for new patients, and improve patients’ throughput in a busy
departments like ours. Second time study acquisition was conducted by the same
standard protocol except for the duration (without administration of new dose
of radiotracer or Furosemide). During the time interval between the two
studies, children were allowed to move, stand and walk according to the child’s
age.
For the purpose of this study, we set six
criteria for the diagnosis of significant renal outflow obstruction during
dual-time 99mTc-MAG3 diuretic renography. Non obstructive
kidney criteria were set as: (a) any down-sloping second time renogram with
rate of drop in counts by ≥ 30% /10 min (regardless of starting counts), or (b)
flat second time renogram but with drop of counts by more than 50% of peaked
counts on first time renogram.
Obstructive criteria were set as: (a)
progressively raising second time renogram with no drop of kidney counts, or
(b) flat second time renogram with drop of kidney counts by less than 30% of
peaked first time renogram counts. Equivocal criteria were set as: (a) flat second
time renogram with drop of counts by 30-50%, or (b) down sloping second time renogram
with drop of counts by < 30%/10 min.
All
patients were followed-up for 6-12 months, and the results of the dual-time 99mTc-MAG3 renography
were compared with the final diagnoses. All patients had clinical follow-up and
sonographic examinations performed at intervals of 3-6 months. Repeated
diuresis renography was performed if there was increasing dilatation on the
sonographic study.
The final
diagnoses were based on either surgical findings or conservative management
with repeated sonography and 99mTc-MAG3 examinations. Diagnosis of
obstruction was made if: (a) further impairment of renal function (>10%) or
hydronephrosis on follow up 99mTc-MAG3 scanning, or ultrasonography,
or (b) improved postoperative drainage and hydronephrosis were
found.
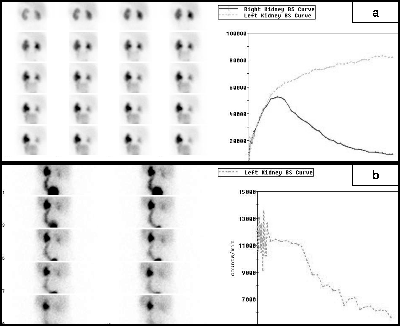
Fig.
1: Six years old boy with left kidney
hydronephrosis and hydroureter. First time renogram (a) shows obstructive
renogram pattern, while second time renogram (b) shows down sloping renogram
(non obstructive criterion).
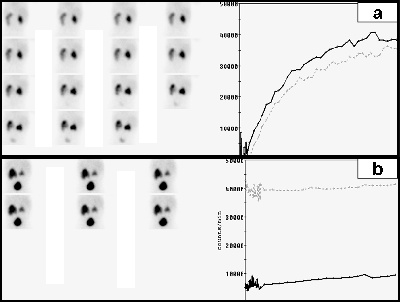
Fig. 2: Three
weeks old newborn with bilateral hydronephrosis. First time renogram (a)
shows bilateral obstructive renograms
pattern, while second time study (b) shows flat renograms for both kidneys,
with no drop of activity compared to first time renogram in the left (obstructive
criterion), and drop of activity by about 75% in the right kidney
(nonobstructive criterion)
Final diagnosis of non-obstructive
hydronephrosis was made when there was no change in differential renal
function on follow-up 99mTc-MAG3 diuretic renography and stationary
or improved hydronephrosis on ultrasonography at 6-12 months in
patients with presumed non obstructive hydronephrosis.
The
decision for surgical intervention or conservative management was determined
by the pediatric urologist, who considered the
results of the
diuresis
renography, including the relative function of the kidney, the child's clinical
findings and serial sonographic examination appearances before making the
management decision.
Results
Dual-time 9mTc-MAG3 diuretic renography revealed
non obstructive patterns in 16 kidneys (15 patients); with down sloping curves
during second time renograms and drop by ≥ 30%/10 min in seven
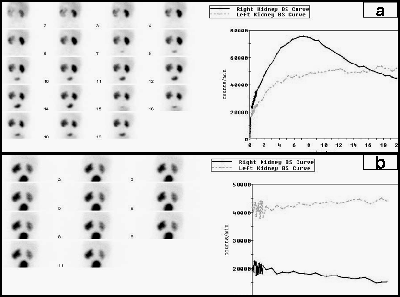
Fig. 3: Three
month neonate with left hydronephrosis. First time renogram (a) shows
obstructive renogram pattern. Second time renogram (b) shows progressively
raised left renogram (obstructive criterion)
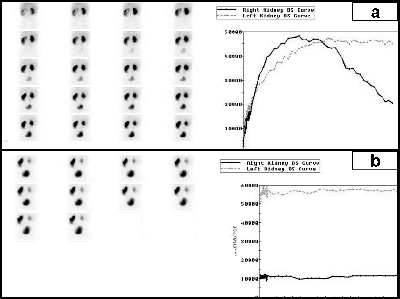
Fig. 4: Eight
years old boy with left hydronephrosis. First time renogram (a) shows
obstructive renogram pattern in the left kidney, while second time renogram (b)
shows flat renogram with no drop in renal counts (obstructive pattern)
kidneys (seven patients) (Fig.1). The second non obstructive
criteria with flat second time renogram but with drop of activity by ≥ 50% of
peaked counts on first time renogram, was noticed within nine kidneys in eight
patients (Fig. 2).
Obstructive patterns were noticed in 31
kidneys (29 patients); progressive raising renogram was noticed in 17 kidneys
(Fig. 3), 12 of them where obstructed while five where not. Second obstructive
criterion with flat renogram with drop by < 30% (Fig. 4) was noticed in 14
kidneys (12 patients), eight of them were obstructed and six were not. The six
kidneys (in four patients) were considered as false positive, since two
patients had long standing severe hydronephrosis with no obstruction (on follow
up), while two patients (four kidneys) had neurogenic bladder with no
obstruction (Fig. 5).
Equivocal patterns were noticed in nine patients, four
of them turned out to have significant obstruction, while five had no
obstruction. Table I and II show the distribution of patients and kidneys
according to dual-time 99mTc-MAG3 diuretic
renography
results and final diagnosis.
Discussion
The management of ureteropelvic junction
obstruction is difficult because the diagnosis of a significant obstruction cannot always be established
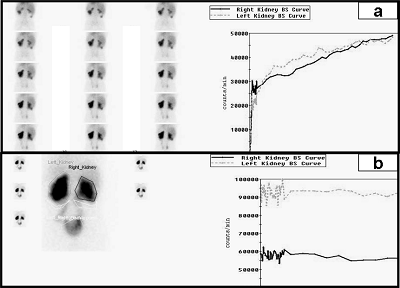
Fig. 5: Seven
years old boy with neurogenic bladder, bilateral hydronephrosis and
hydroureters. First time renogram (a) shows
bilateral obstructive renograms patterns, while second time renogram (b)
shows flat renograms with no drop of renal activity compared to first time
renogram (false positive obstructive patterns)
with certainty without a waiting period for the development
of measurable progressive renal injury.(1,9)
Diuretic renography was indicated in
situations of suspected renal obstruction. Several protocols for diuretic renography have
been described based on variation in timing of diuretic
administration relative to the radiopharmaceutical.(1,10-13) Accepted
protocols for Furosemide injection during renography are the
F+20 and F-15 methods described by O’Reilly et al.(12)
Several groups have reported the utility of early Furosemide administration,
either at F+ 0 (i.e. at the same time as radiopharmaceutical administration)(13,14)
or 2–3 minutes after radiopharmaceutical administration.(15,
16)
The maximal effect of Furosemide is 15-18 minutes
after intravenous injection,(1,2,17) which can justify using
F-15 variation of diuretic
renography in our
study. It has also been emphasized that use of the F-15
protocol would be better for avoiding false-negative or equivocal
results, particularly in cases of intermittent obstruction. Foda et
al,(18)
in a prospective randomized trial, studied 88 children according to
the F-15 or F+20 protocol (44 children in each group) and showed
that the number of positive results was significantly higher with
the F-15 protocol. Turkolmez et al.(19) found
that F+0 and F-15 protocols allow clarification in cases of
equivocal F+20 studies, although the F+0 and F-15 protocol were more
practical and shorter, makes them well
tolerated by most of the patients.(17,19)
The fundamental hypothesis underlying diuretic renography is
that increased urine flow, as produced by the diuretic, will result in
prompt washout of activity in a dilated nonobstructed system. In
cases of obstruction, washout after diuretic remains slow and there
will be prolonged retention of radiopharmaceutical proximal to the
obstruction.(1,3) The renogram pattern is usually related
to the degree of obstruction;(1,7)
an non-obstructed system is easily assessed by prompt tracer washout,
whereas a rising curve will be highly suggestive of true
obstruction. Simple parameters such as time to peak and time to
obtain a washout of 50% of tracer from the kidney allow one to
quantify the response.(1) However, equivocal and even obstructive patterns
on diuretic
renography
are frequently encountered during diuretic renograms for non-obstructed
hydronephrotic kidneys. Causes of such finding can be due to severe dilatation
of pelvicalyceal system, post pyeloplasty, dehydration, renal function impairment,
immature kidneys in neonates, vesicoureteric reflux, tubular necrosis, neurogenic bladder and full bladdereffect,(1,4-8) which are compatible with our experience in this regard.
Table
I. Age distribution, second time scan
patterns including: obstructive (O), non obstructive (N.O) or equivocal and
final diagnoses within our study group
|
No.
|
Age
|
Second time Scan
|
Final Diagnosis
|
No
|
Age
|
Second time
Scan
|
Final Diagnosis
|
|
1
|
3 Weeks
|
N.O(a)
|
N.O
|
28
|
3 years
|
O (a)
|
N.O
|
|
2
|
3 weeks
|
N.O (b)
|
N.O
|
29
|
3 years
|
O (b)
|
O
|
|
3
|
3 weeks
|
O (b)
|
O
|
30
|
3 years
|
N.O (a)
|
N.O
|
|
4
|
4 weeks
|
O (a)
|
N.O
|
31
|
3 years
|
O (b)
|
N.O
|
|
5
|
4 weeks
|
Equivocal (b)
|
O
|
32
|
4 years
|
O (a)
|
O
|
|
6
|
4 weeks
|
O (a)
|
N.O
|
33
|
4 years
|
Rt: O (b)
|
N.O
|
|
7
|
4 weeks
|
N.O (a)
|
N.O
|
Lt: O (b)
|
N.O
|
|
8
|
4 weeks
|
N.O (b)
|
N.O
|
34
|
4 years
|
Equivocal (a)
|
O
|
|
9
|
6 weeks
|
O (a)
|
N.O
|
35
|
5 years
|
O (b)
|
N.O
|
|
10
|
6 weeks
|
O (b)
|
O
|
36
|
5 years
|
Equivocal (a)
|
O
|
|
11
|
2 months
|
N.O (a)
|
N.O
|
37
|
5 years
|
N.O (a)
|
O
|
|
12
|
3 months
|
O (b)
|
O
|
38
|
5 years
|
O (b)
|
O
|
|
13
|
3 months
|
N.O (b)
|
N.O
|
39
|
5 years
|
O (a)
|
N.O
|
|
14
|
4 months
|
O (a)
|
N.O
|
40
|
6 years
|
O (b)
|
O
|
|
15
|
6 months
|
O (b)
|
O
|
41
|
7 years
|
E (a)
|
N.O
|
|
16
|
9 months
|
O (a)
|
O
|
42
|
7 years
|
Rt: N.O (b)
|
N.O
|
|
17
|
9 months
|
Rt: O (b)
|
N.O
|
Lt: N.O (b)
|
O
|
|
Lt: O (b)
|
N.O
|
43
|
7 years
|
O (b)
|
N.O
|
|
18
|
9 months
|
N.O (a)
|
N.O
|
44
|
8 years
|
Equivocal (a)
|
N.O
|
|
19
|
9 months
|
O (b)
|
O
|
45
|
8 years
|
O (b)
|
N.O
|
|
20
|
9 months
|
N.O (b)
|
N.O
|
46
|
8 years
|
N.O (a)
|
N.O
|
|
21
|
1 year
|
N.O (b)
|
N.O
|
47
|
10 years
|
O (b)
|
O
|
|
22
|
1 year
|
Equivocal (b)
|
N.O
|
48
|
10 years
|
Equivocal (b)
|
N.O
|
|
23
|
1 year
|
Equivocal (b)
|
O
|
49
|
10 years
|
O (a)
|
N.O
|
|
24
|
1 years
|
O (b)
|
O
|
50
|
11 years
|
O (b)
|
O
|
|
25
|
2 years
|
N.O (b)
|
N.O
|
51
|
11 years
|
N.O(b)
|
O
|
|
26
|
2 years
|
O (b)
|
O
|
52
|
12 years
|
O (b)
|
O
|
|
27
|
2 years
|
O (a)
|
N.O
|
53
|
12 years
|
Equivocal (a)
|
N.O
|
Table II. Distribution of patients according to
dual-time 99mTc-MAG3 diuretic renography results and clinical
outcome
|
Final diagnosis
|
Down sloping renogram with
drop in kidney counts by ≥30%/10 minutes
(Kidney)
|
Flat renogram with drop of activity by
≥ 50%
(Kidney)
|
Progressive raising renogram
(Kidney)
|
Flat renogram with drop of activity
By < 30%
(Kidney)
|
Equivocal patterns
(Kidney)
|
|
Non obstructed
|
6
|
7
|
3
|
8
|
5
|
|
Obstructed
|
1
|
2
|
7
|
13
|
4
|
|
Total
|
7
|
9
(8 patients)
|
10
|
21
(19 patients)
|
9
|
Gravity assisted drainage was recommended
to increase the accuracy of diuretic renography and to overcome
most diagnostic problems related to full bladder and its resultant back
pressure.(20,21)
During our study gravity assisted drainage was somehow not helpful since
15 kidneys did not show gravity assisted drainage and only six of them were
found to be obstructed.
Because renal
function, especially glomerular filtration, is immature at birth,
some authors recommend waiting until at least four
weeks after birth before performing diuretic renography,(12,14)
while there is still much debate over how hydronephrosis in neonates is
best managed. Some authors recommend
conservative management and close follow-up, whereas others prefer
early surgery.(22,23)
Our study group included eight neonates with obstructive patterns during
diuretic renography, and only two were found to have significant obstruction.
Our study included 56 kidneys with
variable degrees of hydronephrosis. All had obstructive patterns during routine
diuretic renography, while only 27 were found to have significant obstruction.
Excluding obstruction in such patients is critical to avoid unjustified
surgical interventions. Our study was able to rule out obstruction in 13 (43%)
of non obstructed kidneys. Although our new criteria on dual-time renography
misinterpreted three obstructed kidneys as non-obstructed, we still think that
patients with non-obstructed criteria according to dual-time renography can be
safely managed by follow up scan to avoid unjustified surgical interventions.
Our new protocol and criteria were of
clear benefit in ruling out obstruction, even in neonates with immature kidneys
and post pyeloplasty children who had obstructed or equivocal routine diuretic
renography. False positive results were noted in patients with neurogenic
bladder and severe hydronephrosis.
Although our new protocol would extend the
duration of diuretic renography study, which can affect patients’ throughput in
busy departments, still the improvement in the efficiency can justify this
modification. Also, gravity assisted static view will not be necessary and will
be replaced by the second time renogram. This can compensate for the duration
of second time renogram with further improvement in the efficiency.
Although this study was set up prospectively,
still our applied new criteria were set retrospectively depending on second
time imaging findings and final clinical diagnosis. This factor can be considered
a limitation in our study, and further prospective studies on larger number of
patients are necessary before establishing the diagnostic value of this
protocol.
Conclusion
Our data and results show the potential advantage
of dual-time 99mTc-MAG3 renography to differentiate between obstructed and
non-obstructed hydronephrosis. This method may reduce unjustified surgical
interventions and the need for frequent follow up scanning.
References
1. Boubaker A, Prior J, Meuwly JY, et al.Radionuclide investigations of the urinary
tract in the era of multimodality imaging. Journal of Nuclear Medicine
2006; 47(11): 1819-1836.
2. Rossleigh MA. Renal cortical scintigraphy and diuresis
renography in infants and children. J Nucl Med 2001; 42: 91-95.
3. Chrall H, Koff A, Keyes
Jr. Diuretic
radionuclide renography
and scintigraphy in the differential diagnosis of hydroureteronephrosis. Semin
Nucl Med 1981; 11: 89–104.
4. O’Reilly H, Testa J,
Lawson S, et al. Diuresis renography
in equivocal urinary tract obstruction. Br J Urol 1984; 56: 84.
5. O’Reilly H. Diuresis renography: recent advances and
recommended protocols. Br J Urol 1992; 69: 113-120.
6. English J, Testa J,
Lawson S, et al. Modified method of diuresis renography for the assessment of equivocal
pelviureteric junction obstruction. Br J Urol 1987; 59:10-14.
7. Society for Fetal Urology
and Pediatric Nuclear Medicine Council and the Society of Nuclear Medicine. The "well tempered" diuretic
renogram: a standard method to examine the asymptomatic neonate with
hydronephrosis or hydroureteronephrosis. J Nucl Med 1992; 33: 2047–2051.
8. Gordon I, Dhillon K,
Gatanash H, Peters M. Antenatal diagnosis of pelvic hydronephrosis: assessment of renal
function and drainage as a guide to management. J Nucl Med 1991; 32: 1649–1654.
9. Clautice-Engle T, Anderson G, Allan B,
Abbott D.
Diagnosis of obstructive hydronephrosis in infants: comparison sonograms
performed 6 days and 6 weeks after birth. AJR 1995; 164: 963-967.
10. Boubaker A, Prior J,
Antonscu C, et al. F+0 enography in neonates and infants younger than 6 months: an
accurate method to diagnose severe obstructive uropathy. Journal of Nuclear
Medicine 2006; 42(12): 1780-1788
11. Liu Y, Ghesani N,
Shurrnick J, et al. The F+0 protocol for diuretic renography results in fewer
interrupted studies due to voiding than F-15 protocol. Journal of Nuclear
Medicine 2005; 46(8): 1317-1320.
12. Wong C, Rossleigh A,
Farnsworth H. F+O
diuresis renography in infants and children. J Nucl Med 1999; 40: 1805-1811.
13. O’Reilly PO, Aurell M, Britton K, et al. Consensus on diuresis renography for
investigating the dilated upper urinary tract. J Nucl Med 1996; 37: 1872-1876.
14. Wong C, Rossleigh A,
Farnsworth H.
Utility of technetium-99m-MAG3 diuretic renography in the neonatal period. J
Nucl Med 1995; 36: 2214-2219.
15. Sfakianakis N, Heiba S,
Ganz W, et al. Diuretic renography with early injection of furosemide: a
reliable and cost effective approach. J Nucl Med 1989; 30: 841. [abstract]
16. Boubaker A, Meyrat B,
Frey P, et al. Diuresis renography with early (2-3') frusemide injection. Eur
J Nucl Med 1997; 24: 866. [abstract]
17. Mandell A, Cooper A, Leonard C, et al. Procedure guidelines for diuretic renography
in children. J Nucl Med 1997; 38: 1647-1650.
18. Foda R, Gatfield T,
Matzinger M, et al. A prospective randomized trial comparing 2 diuresis renography
techniques for evaluation of suspected upper urinary tract obstruction in
children. J Urol 1998; 159: 1691-1693.
19.Turkolmez S, Atasever T, Turkolmez K, et al. Comparison of three
different diuretic renal scintigraphy
protocols in patients with dilated upper urinary tracts. Clin Nucl Med 2004;
29:154-160.
20. Wong C, Rossleigh A,
Farnsworth H.
Diuretic renography with the addition of quantitative gravity-assisted drainage in infants and children.
J Nucl Med 2000; 41: 1030-1036.
20. Rossleigh A, Leighton M,
Farnsworth H.
Diuresis renography:
the need for an additional view after gravity-assisted drainage. Clin Nucl
Med 1993; 18: 210-213.
21. DiSandro J, Kogan A. Neonatal management: role for early
intervention. Urol Clin North Am 1998; 25:187–197.
22. Koff A. Neonatal management of unilateral
hydronephrosis: role for delayed intervention. Urol Clin North Am 1998; 25:
181-186.