ABSTRACT
Objectives: Ventriculoperitoneal shunt surgery is the most widely
used procedure in the treatment of hydrocephalus. However, this procedure has been associated
with several delayed unusual complications. This paper will discuss these cases,
their management and suggest ways on how to avoid these complications.
Methods: This prospective study was conducted in the
neurosurgical unit at King Hussein Medical Centre, and included the patients
between January 1996 - July 2007. The patients’ images and management were
reviewed.
Results: Sixteen
patients were included in the study (10 males and 6 females). Their age was between three months and 40
years. One case had rectal perforation
by ventriculoperitoneal shunt, seven cases had intraventricular migration of ventriculoperitoneal
shunt, one case had umbilical perforation, one case had chest wall perforation by
ventriculoperitoneal shunt, one case had liver perforation, four cases had
overdrainage with subdural hematoma, one case had bladder perforation and one
case had colon perforation by a ventriculoperitoneal shunt resulting in pneumocephalus.
The management of ventriculoperitoneal shunt complications is discussed in
detail in this study.
Conclusions: The information provided within this study provides
an analysis of our cases and the literature as it relates to the unusual
complication of ventriculoperitoneal shunt through symptomatic presentation,
diagnosis and management of these cases.
Key words: Hydrocephalus, Unusual complications, Ventriculoperitoneal
shunts
JRMS
December 2009; 16(3): 55-60
Introduction
The cerebrospinal fluid (CSF)
shunt devices are associated with a number of complications, which has tempered
the initial enthusiasm and, subsequently, the hope arisen by the introduction
of any newly designed CSF shunt apparatus. Actually, the overall analysis of
the results after treatment clearly indicates that the impact of CSF shunt
device improvements on the failure rates seems to be very limited. Prevention, early
identification and management of CSF shunt failures remain the main tools for
assuring the quality of patient's long term outcome.
Methods
A prospective study of patients
who developed unusual complications following ventriculoperi-toneal (VP) shunt
for hydrocephalus between January 1996 and July 2007 at the neurosurgical unit
at King Hussein Medical Centre was carried out.
There were 16 patients in this study, ten were males and six were
females. Their age ranged between three months and 40 years.
Our patients presented with
unusual ventriculoperitoneal (VP) shunt complications. It was easy to diagnose
them on the bases of clinical presentation especially when the VP shunt tip protruded
out of the anus or the penis. These
Table I. Management of CSF shunt infections
|
1. Prevention
|
§
Short operative time
§
Presence of only required staff in the operating room
§
Plastic isolators (sterile-drapes)
§
Small surgical wounds
§
Shunt components away from the incision line
§
Avoid direct manipulation of the shunt (use sterile gauzes and
forceps)
§ Perioperative antibiotics
|
|
2. Treatment
|
§
Remove the infected shunt and position an external ventricular
catheter through the existing burr hole.
§
Intrathecal antibiotics based on CSF cultures for 10-12 days
§
Combine IV antibiotics only in case of systemic manifestations
§
Three CSF negative cultures after discontinuing the antibiotic
treatment followed by new shunt placement
§
Consider systemic antibiotics and immediate shunt replacement
only in children with compromised general conditions (e.g. reduced immune
defenses during chemotherapy)
|
Table II. Management of post-shunting collections
|
1. Epidural hematoma
|
§
Craniotomy
§
Raise the valve pressure (mild symptoms)
§
No treatment (asymptomatic cases with thin collections: close
neuroradiological screening)
|
|
2. Acute subdural hematoma
|
§
Craniotomy
§
Temporary external subdural devices (mild symptoms; sub-acute collections)
§ Raise the valve pressure (thin collections;
asymptomatic patients)
|
|
3. Chronic subdural hematoma
|
§
Surgical treatment also in asymptomatic children (high rate of
hematoma calcification in the pediatric age group)
§
Burr holes and temporary external drainage and/or
§
Valve pressure raising
§
Craniotomy (fibrous membranes)
§
Subduro-peritoneal shunts (highly fluid collections)
|
|
4. Chronic subdural hygroma
|
§
Transient external subdural or subduro-peritoneal shunts
(unilateral also for bilateral collections) and/or
§
Raise the valve pressure
§ Implant a programmable
valve
|
Table III. Management of visceral perforation, shunt
disconnection and migration
|
Management of Visceral perforation
|
§
Remove the shunt and exclude (CSF samples) shunt infection. If
no shunt infection is detected
§
New site peritoneal catheter insertion or
§
Ventriculo-atrial shunt
|
|
Management of Disconnection and/or migration
|
§
Open viscus repair in selected cases (e.g. active enteritis;
infected pseudocysts)
§
One step repositioning of the shunt if no external communication
is detected (in alternative treat the shunt as an infected one)
§
Remove the migrated shunt only in case of recurrent CSF
infections
|
patients presented to us with headache, fever,
vomiting and signs of meningeal irritation.
Chest wall erythema and cerebrospinal fluid leak through the abdominal
wall is another presentation. Computed
tomography was helpful in the diagnoses of over drainage with subdural hematoma
and pneumocephalus.
Results
There are several precautions which should be taken during the ventriculoperitoneal shunt procedure
which minimize the risk of shunt infection. When infection occurred the mode of
treatment followed is summarized Table I. In cases of post-shunt collection the
management of different types of hematomas is discussed in Table II. The
perforation of the bowel was a very rare complication. In cases with this complication the shunt was
removed without complication and the patients remained asymptomatic (Table III).
|

Fig. 1. CT scan showing disconnected VP shunt
|

Fig. 2. Axial CT scan showing over drainage
with chronic subdural hematoma.
|
|

Fig. 3. Axial CT scan showing discrepancy between cranial and brain volumes | 
Fig. 4. VP shunt protruding through the liver
|
Discussion
Infection is the foremost type of CSF shunt
complication after mechanical malfunctions. Even though the incidence of this
complication may vary in the literature, most authors report infection rates
between 5% and 18%.(1)
The use of
one-piece shunts has decreased the incidence of disconnection complication. Disconnection is mainly seen as a consequence
of excessive strain on the pumping device.
Stretching at this level causes valve damage and with time may cause the
system to fracture. Multipiece shunts can disconnect at any attachment site (Fig
1); because of the continuous traction forces junctions at the neck or the
abdomen should always be avoided. The weakest points are the interface between
silicone and metallic components and the ligatures, which favor the tearing of
the plastic material.(1,2)
In cases
with cerebrospinal fluid over drainage, the amount of drained CSF from the
cerebral ventricular system is not directly related to the opening pressure of
the inserted valve, but to the pressure gradient existing between the
ventricles and the body cavities to where the CSF is diverted.(3)
Over drainage complications may be
divided into acute and chronic. Epidural hematomas (Fig. 2) are an unusual
complication of ventriculoperitoneal shunt placement and are much less common
than post-shunting subdural collections.(4) Young age and evidence of chronic
hydrocephalus are factors recognized to favor this condition; a discrepancy
between cranial and brain volumes may further contribute to this condition (Fig. 3). The rapid
reduction in intracranial pressure following CSF drainage, results in
separation of the dura mater from the skull and tearing of small dural vessels. It is known that the dura mater in
children and young adults is less adherent to the skull than in older patients,
which explains why most cases of postventriculostomy epidural hematomas occur in
children and young adults.
Prophylactic
measures include the careful evacuation/refilling of the ventricles during
surgery and the use of high-pressure opening valve systems in selected cases
with severe or long-standing hydrocephalus. Anti-siphon devices and
programmable valves have also been reported to reduce the incidence of subdural
collections.
Craniotomy and removal of
the clot is needed in patients with acute and/or rapid clinical worsening.
Short term application of subdural suction devices is an alternative option in
mildly symptomatic cases. Other therapeutic options are temporarily closing the
drainage and changing the drainage system to one with a higher opening pressure
valve.(3)
Visceral perforation
Visceral perforation is an
unusual but serious complication of ventriculoperitoneal shunting; the
incidence of mortality can be as high as 15%. The bowel is the most involved site (0.1%)
with theprotrusion of the ventriculoperitoneal shunt through the anus(5) (Fig. 4), the bladder (Fig. 5), the stomach, or the liver (Fig. 6). Early cases occur at the time of insertion because the surgeon mistakes a viscus wall for the peritoneum. Peritoneal adhesions and improper (too high for the liver and gallbladder; low for the bladder and vagina) skin incisions increase the risk. No definite cause has been recognized for later occurrences. It is speculated that local inflammation favors fibrous encasement of the tube; the following chronic friction slowly weakens the viscus wall leading to its breakdown. Complete lack of symptoms is possible and in almost all the cases of colonic perforation(6) signs of peritonitis are lacking On the contrary, abdominal pain and distention, fever and erithema of the abdominal wall may be evident in cases of bladder perforation, corresponding to the immediate occurrence of secondary peritonitis.(7) Leptomeningitis signs may complicate the clinical course and often are the first manifestation when rectal penetration by a disconnected ventriculoperitoneal shunt tube has happened.(8) Gram-negative bacteria are the main pathogenic agents, with E. Coli as the most frequently isolated organism in colonic cases.(9) Pneumocephalus, although rare, has also to be regarded as a typical onset in these patients. In an appropriate clinical setting, it helps to establish the origin of a meningeal infection.(10)
|
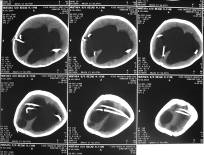
Fig. 5. Axial CT scan showed VP shunt
migration into the lateral ventricle
|
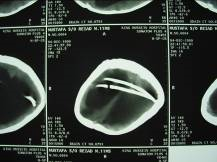
Fig. 6. Axial CT scan showed shunt migration into the lateral
ventricle
|
|
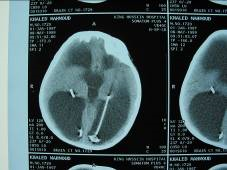
Fig. 7. Axial CT scan showed VP shunt
migration into the lateral ventricle
|

Fig. 8. VP shunt extrusion into the
chest
|
|

Fig. 9. VP shunt migration into the abdominal wall
|

Fig. 10. VP shunt protrusion through the
umbilicus |
|
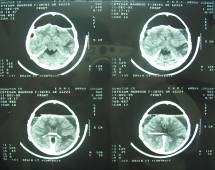
Fig. 11. Axial CT scan showed air penetration
into the skull
|
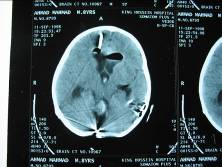
Fig. 12. Axial CT scan showed air inside the lateral ventricle
|
|

Fig. 13. Ventriculoperitoneal shunt protruding through
the anus
|

Fig. 14. Ventriculoperitoneal shunt protruding through
the urethra
|
Migration or Extrusion
Migration or extrusion of
the CSF implanted device is rare. Incidence is higher for VP shunts, favored by the high mobility of the peritoneal end inside the abdomen as well as by the anatomical
characteristics of the abdominal cavity itself.(11)
Various ways
of migration have been described such as into the lateral ventricle(12)
(Fig. 7 & Fig. 8), mediastinum, chest (Fig. 9), gastrointestinal
tract, abdominal wall (Fig. 10 & Fig. 11), bladder, vagina and scrotum. Spontaneous
extrusion through the umbilicus (Fig. 12), a very rare occurrence, probably
underlies two mechanisms: the patency of the umbilical end of the
vitello-intestinal duct and the intrinsic anatomical weakness of the umbilicus
region, acting as a centrally situated natural scar.(13)
Proximal migration is definitely unusual, but cases have been reported of
complete shunt settling into the subgaleal tissue, inside the ventricles, the subarachnoid
and subdural space and the brain parenchyma.(14) Various
hypotheses have been advanced. Scott et al. postulated that
flexion-extension movements of the patient's head may act as a windlass,
facilitating upward movement of the peritoneal catheter.(15)
Other mechanisms suggested by Abou el Nasr are negative suction from
intraventricular pressure and positive intra-abdominal pressure.(16).
A role of loose subcutaneous tissue has been suggested. "Memory" of the packaged coiling of
the shunt system may further mediate the process.(16)
Pneumocephalus
Even if this complication
cannot be regarded as a direct manifestation of CSF over drainage, air
penetrating into the skull in hydrocephalic patients (Fig. 13 % Fig. 14) may
correspond to the reduction in volume of the brain, due to the siphon effect of
the shunt.(3) Discontinuities of the cranial floor are
important.(17) Negative
pressures are developed in standing positions; CSF is displaced either through
the cranial base or through the shunt. The negative pressure and the displaced
volume of CSF flow allow the air to fill the vacuum. The air is then trapped by
brain plugs as a result of a ball-valve phenomenon.(17,18)
Treatment of patients with thinning of the cranial base would probably benefit
from high pressure shunt-valves or antisiphon devices. These might reduce the
high negative pressures and increase the margin of safety.(17)
Upon emergency, a burr hole
is indicated, to relieve tension air collections.(18) The
etiology and site of the skull base connection are crucial to therapy.
Treatment of choice is the closure of the fistula, with eventual temporary
removal (or conversion to an external drainage) of the CSF shunt. In patients
with pneumocephalus due to visceral perforation, the shunt should be removed,
the connection closed if necessary and a new shunt placed at a different site
after a temporary extraventricular drainage, to exclude CSF infections.(10)
Conclusion
As doctors we should be
aware of unusual complications of VP shunts, especially when patients present
with acute abdomen with signs of meningeal irritation in which we should keep
in our mind bowel or viscus perforation.
Long term follow up of patients with VP shunt is important for early
detection of rare complication.
References
1. Guillen A,
Costa JM, Castello I, Claramunt E, Cardona E. unusual abdominal
complication of ventriculoperitoneal shunt. Neurocirugia (Astur) 2002;
13(5):401-4
2. Di Rocco C, Iannelli A. Complications of CSF shunting. In C. Di Rocco: The
treatment of Infantile Hydrocephalus, CRC Press Inc. Boca Raton, FL., 1987; vol. II, pp. 79-153.
3. Aschoff A,
Kremer P, Benesch C, Fruh K, Klank A, Kunze S. Overdrainage and shunt
tehnology. Childs Nerve Syst 1995; 11(4):193-202.
4. Carmel PW,
Albright Al, Adelson PD, Canady A, Black P, et al. Incibence and management of
subdural hematoma/hygroma with variable- and fixed-pressure differential valves.
Neurosurg Focus 1999; 15: 7(4):e7.
5. Adeloye A. protrusion of ventriculo
peritoneal shunt through the anus. East Afr
Med J 1997; 74(5): 337-9.
6.
Sathyanarayana
S, Wylen EL, Baskaya MK, Nanda A. Spontaneous bowel perforation after ventriculoperitoneal shunt surgery:
case report and review of 45 cases. Surg
Neurol 2000; 54(5): 388-96
7.
Martinez HP, Barrera
RC, Villanueva
SE,
Zavala MJ. Colonic perforation
as a complication of ventriculoperitoneal shunt. Tech Coloproctol 2006; 10(4):353-5.
8. Chen HS. Rectal penetration by a disconnected
ventriculoperitoneal shunt tube. Chang Gung Med J 2000; 23(3):180-4.
9.
Ueda
Y, Kakino S, Hashimoto O, Imoto K. Perforation of the bladder by a peritoneal catheter: an unusual late
complication of ventriculo-peritoneal shunt. No Shinkei Geka 1998; 26(5):
413-6.
10. Karibe H, Ishibashi Y. A case of sigmoid colon perforation by a V-P shunt tube
resulting in pneumocephalus. No Shinkei Geka 1998; 26(1):79-82.
11. Dominguez CJ, Tyagi A, Hall G,
Timothy J, Chumas PD. Sub-galeal
coiling of the proximal and distal components of a ventriculo-peritoneal shunt.
An unusual complication and proposed mechanism. Child's Nerv Syst 2000; 16:
493-5.
12. Ammar A, Nasser M. Intraventricular migration of VP shunt. Neurosurg
Rev 1995; 18(4): 293-5.
13. Eser O, Dogru O, Aslan A, Kundak A. Umbilical perforation: an unusual complication of a
ventriculoperitoneal shunt. Child's Nervous System 2006; 22(11): 202-5
14. Nadkarni, Menon RK, Dange NN, Desal
KI, Goel A. Cranial migration
of complete ventriculo-peritoneal shunt assembly. J Clin Neurosci 2007; 4(1):
92-4.
15. Scott M, Wycis HT, Murtagh F, Reyes
V. Observations on ventricular
and lumbar subarachnoid peritoneal shunts in hydrocephalus infants. J
Neurosurg 1955; 12: 165-75.
16. Abou el Nasr HT. Modified method for prophylaxis against unishunt
system complications with presentation of total intraventricular migration of
unisystem ventriculoperitoneal shunt. Child's Nerv Syst 1988; 4: 116-8.
17. Villarejo F, Carceller F, Alvarez C,
Benscome J, et al.
Pneumocephalus after shunting for hydrocephalus. Child's Nerv Syst 1998;
14(7): 333-7.
18. Cantisani PL, Cancelliere M, Armenise B, Lupo F. Hypertensive pneumocephalus and nasal fistula in
ventriculo-peritoneal shunt: case report and review of the literature. J
Neurosurg Sci 1999; 43(2): 153-7.