ABSTRACT
Objectives: To study whether skeletonization of the internal thoracic artery has any beneficial effects on the rate of sternal wound Infection after Coronary Artery Bypass Surgery and to compare this with the results of the classical pedicled form.
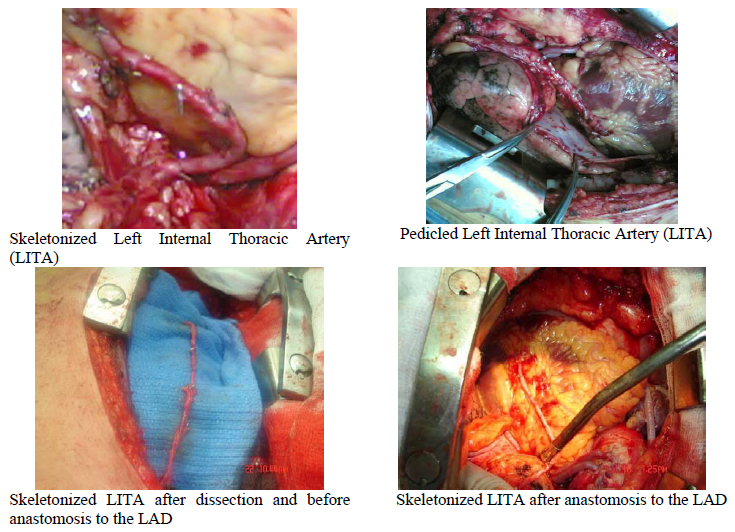
Methods: A total of 212 patients were reviewed between October 2005 and February 2006 and divided into 2 groups according to the method of harvesting the left internal thoracic artery. Group I with 158 patients, 102 males and 56 females with a mean age of 59±2 Years. Group II with 54 patients, 41 males and 13 females with a mean age of 57±2 Years. In group I, the Left Internal Thoracic Artery was harvested in the classical pedicle form (preserving the vasa vasorum, venous drainage) using the cautery and clips. In group II another method of harvesting was adopted using forceps and scissors and depriving the Left Internal Thoracic Artery from all the accompanying structures.
Results: The overall rate of sternal wound infection was 9.5% in Group I and 3.7% in group II (P value<0.05).In Group I, 10 males and 5 females were infected (males 9.8% and females8.9%) while in group II only 2 male patients were infected.
Conclusion: Harvesting the Left Internal Thoracic Artery in the skeletonised form takes longer time and is more difficult to do due to our developing learning curve; nonetheless it has a beneficial effect on decreasing the rate of sternal wound infection. The overall outcome was improved but other issues such as the overall patency and post operative pain should be studied more thoroughly.
Key words: Coronary Artery Bypass Surgery (CABG), Left Internal Thoracic Artery (LITA), Skeletonization.
JRMS December 2008; 15(3): 41-45
Introduction
Skeletonization of the internal thoracic artery (ITA) involves mobilization of the arterial trunk from the satellite veins and surrounding tissues. Advocates of skeletonization of the ITA cite the preservation of sternal blood flow reduces the incidence of complications, gives longer graft length and larger caliber.
Arterial grafting during coronary bypass surgery is routinely performed as a result of the success of left ITA grafting of the left anterior descending coronary artery (LAD).(1) Compared with saphenous vein bypass grafting, patients who receive an ITA to the left anterior descending artery survive longer and experience less hospitalization for cardiac events, lower rates of cardiac re-operation, and less frequent myocardial infarction. In fact, skeletonization of the ITA grafts seems to preserve substantial collateral flow to the sternum by sparing some of the sternal and intercostal branches that arise from the ITA as a common trunk.(2-4) It has been previously demonstrated that patients who develop deep sternal infection have a 3-fold increase in intensive care unit and hospital length of stay, as well as a 3-fold increase in mortality.(4)
Substantial collateral blood flow to the sternum can be maintained in the absence of the ITA, provided the sternal-anterior intercostal trunk is left intact. Skeletonization of the ITA often results in preservation of this common trunk, particularly if meticulous dissection is performed. We therefore hypothesized that skeletonization would lower the risk of sternal infection, particularly in high-risk patients.(5)
Methods
This study was conducted in the Department of Cardiovascular surgery at Queen Alia Heart Institute (QAHI) by a single operator. We simply elected to compare another method of harvesting the left internal thoracic artery (LITA); namely skeletonised method with our standard technique of pedicle harvesting. In contrast to pedicled harvesting; where cautery is performed, skeletonization involves sharp dissection of the internal thoracic artery away from its accompanying veins and surrounding tissue. The branches are doubly clipped and divided with scissors.
We performed this technique in 54 patients and compared the outcome with previous cases of 158 patients. We looked at the rates of wound infection (superficial and deep), re-opening for bleeding, pre-op low ejection fraction and presence of Diabetes Mellitus (DM). We have included all forms of wound infection from simple superficial infection to major sternal wound dehiscence.
We have excluded urgent cases and cases where an Intra Aortic Balloon Pump (IABP) was inserted pre-operatively.
Table I illustrates the demographics of the two groups. They are comparable in terms of age; gender and pre-operative ejection fraction. However, we had more diabetics in group I.
Table I. Demographics characteristics and results
|
P value
|
Group II
|
Group I
|
|
|
N/A
|
54
|
158
|
No. of Patients
|
|
P>0.05
|
57±2 Yrs
|
59±2 Yrs
|
Mean age± Standard deviation
|
|
N/A
|
41/13
|
102/56
|
Male/Female
|
|
P<0.05
|
10)18.5%)
|
40 (25%)
|
DM
|
|
P>0.05
|
8 (14.8%
|
36)22.8%)
|
Low EF
|
|
P>0.05
|
2 (3.7%)
|
5 (3.1%)
|
Re-opening
|
|
P<0.05
|
2 (3.7%)
|
15 (9.5%)
|
Wound infection
|
Results
Group I represents the classical method of LITA harvesting as a pedicled form included 158 patients; 102 males, with a mean age of 59±2 years. Wound infection occurred in 15 patients, representing a wound infection rate of 9.5%.
Group II representing the other technique of LITA skeletonization was performed in 54 patients; 41 males with wound infection occurring in 2 male patients; representing a wound infection rate of 3.7%.
Re-opening for bleeding was 5 patients in group I (3.1% re-opening rate) and 2 patients in group II (3.7% re-opening rate).
Patients with low ejection fraction (Estimated Left Ventricular Ejection Fraction LV EF ≤ 35%) were 36 patients (22.8%) in group I compared with 8 patients in group II (14.8%).
DM was found in 40 patients in group 1 (25%) and 10 patients in group 2 (18.5%).
Our study suggest that skeletonization of the LITA is associated with lower wound infection.
Discussion
Sternal wound infection is a devastating complication after Coronary Artery Bypass surgery. Factors that increase the rate of sternal wound infection include; DM, peripheral arteriopathy, re-sternotomy for bleeding, female gender and the use of both internal thoracic arteries compared with single artery.(4,5)
Re-opening for bleeding is an independent and powerful risk factor (more than nine fold increase) for deep sternal infection. The reason lies in the added tissue injury and ischemia at a time when sternal blood flow is most critical for early healing and consequent sternal stabilization.(6-8) In fact, exploration for excessive postoperative bleeding (>200 mL/h for 4 hours) after chest closure has been shown to carry a significantly higher incidence of wound dehiscence and infection.(9,10) It is therefore not surprising that re-opening is more often in patients receiving bilateral ITA grafting who already have a greater acute reduction in sternal blood flow.
Although skeletonization is associated with a decreased risk of wound infection, some potential drawbacks should be addressed. First, skeletonization may be more technically difficult than pedicled ITA harvesting and may increase the risk of conduit injury. In the current study, we found a significant (15-20minutes) increase in operating time for patients undergoing skeletonization. However, we believe that skeletonization can be safely performed, and that the risk of ITA injury is small. Experimental studies revealed that skeletonization does not result in more histological or endothelial damage than pedicled ITA harvesting.(11,12) Furthermore, skeletonised ITA conduits have better intra operative blood flow than pedicled conduits, as well as increased length.(5,12,13) The latter finding may be important for patients with distal coronary targets.
Another potential drawback of skeletonization is that it is a relatively less used surgical technique, thus current data are lacking on long-term patency rates. Early and midterm patency studies have yielded very encouraging(14,15) although further studies are required, it is unlikely that long-term patency rates will be worse than for pedicled ITA grafts
Some concerns have been raised about the possibility that the technique of artery skeletonization might somehow damage the endothelium of the harvested ITA and consequently impair its long-term patency. Although studies are lacking on the long-term follow-up of patency and outcome after artery skeletonization, a recent review of the available literature(4,16) on this subject did not report any substantial evidence that skeletonization causes damage to the harvested ITAs or that the levels of patency were different from those of patients receiving pedicled ITAs.
Another potential benefit of skeletonization is decreased postoperative chest wall pain. Intercostal nerve damage occurs frequently after pedicled ITA harvesting.(17) It has been previously demonstrated that three quarters of patients who underwent coronary bypass showed evidence of intercostal nerve damage after pedicled harvesting, and that 15% of these patients experienced persistent postoperative pain.(18)
It should be noted that patients who received skeletonised grafts fared better than patients who received pedicled grafts for outcomes other than sternal infection(5,12,13) Skeletonization was associated with a lower prevalence of low cardiac output syndrome and intra-aortic balloon use. Improvement in early cardiac output may relate to the increased conduit diameter and blood flow reported in skeletonised compared with pedicled grafts(12,13)
Several investigators looked at the effect of skeletonization on post operative parameters including wound infection. De Paulis and colleagues demonstrated a reduction in deep and superficial sternal wound infection; from 11.1% for bilateral internal thoracic arteries to 2.5% when skeletonization was performed.(4) This was also mirrored from Petersen and colleagues’ report of a reduction of all forms of wound infection from 11% to 1.3% when skeletonization was employed.(5) Others have demonstrated the benefits of reduction in sternal wound infection for patients undergoing bilateral internal thoracic artery harvest.(4,5,12,13,18)
The flow characteristics of skeletonised internal thoracic arteries is not adversely affected by skeletonization, Wendler(19) suggests the opposite; he compared 40 pedicled LITAs with 40 skeletonised, while no difference was initially seen after harvest, skeletonised LITAs demonstrated 25% more flow after papaverine injection.(19,20) There is consensus that skeletonization increases conduit length by about 3cm and may also increase flow and conduit diameter.(14,20)
Limitations of the study are that our study included only a small number of patients in whom this technique of skeletonization was performed. Also this study is not randomized we simply compared another technique of internal thoracic artery harvest with our classical pedicled technique.
Conclusion
Harvesting the LITA in the skeletonized form takes longer time and more difficult to do because of our developing learning curve. Still It was obvious that It has a beneficial effect on decreasing the rate of sternal wound infection in both males and females .The overall outcome was improved but other issues such as the overall patency and post operative pain should be studied more thoroughly.
References
1.Loop FD, Lytle BW, Cosgrove DM, et al. Influence of the internal-mammary-artery graft on 10-year survival and other cardiac events. N Engl J Med 1986; 314(1):1–6
2.Henriquez-Pino JA, Gomes WJ, Prate JC, Buffalo E. Surgical anatomy of the internal thoracic artery. Ann Thorac Surg 1997; 64:1041-1045.
3.De Jesus RA, Acland RD. Anatomic study of the collateral blood supply of the sternum. Ann Thorac Surg 1995;59:163-168
4.De Paulis R, de Notaris S, Scaffa R, et al. The effect of bilateral internal thoracic artery harvesting on superficial and deep sternal infection:
The role of skeletonization. J Thorac Cardiovascular Surg 2005;129:536-543
5.Peterson M, Borger M, Rao V. Skeletonization of bilateral internal thoracic artery grafts lowers the risk of sternal infection in patients with diabetes. J Thorac Cardiovasc Surg 2003;126:1314-1319
6.Ottino G, De Paulis R, Pansini S, et al. Major sternal wound infection after open-heart surgery: a multivariate analysis of risk factors in 2,579 consecutive operative procedures. Ann Thorac Surg. 1987;44:173-179
7.Loop FD, Lytle BW, Cosgrove DM, et al. Sternal wound complication after isolated coronary artery bypass grafting: Early and late mortality, morbidity and cost of care. Ann Thorac Surg 1990;49:179-187
8.Lu JC, Grayson AD, Jha P, et al. Risk factors for sternal wound infection and mid-term survival following coronary artery bypass surgery. Eur J Cardiothorac Surg 2003;23:943-949
9.Talamonti MS, LoCicero III J, Hoyne WP, et al. Early re exploration for excessive postoperative bleeding lowers wound complication rates in open heart surgery. Am Surg 1987;53:102-104
10.Boeken U, Eisner J, Feindt P, et al. Does the time of re sternotomy for bleeding have any influence on the incidence of sternal infections, septic courses or further complications? Thorac Cardiovasc Surg 2001; 49:45-48.
11.Gaudino M, Toesca A, Nori SL, et al. Effect of skeletonization of the internal thoracic artery on vessel wall integrity. Ann Thorac Surg 1999; 68:1623–1627.
12.Deja MA, Wos S, Golba KS, et al. Intraoperative and laboratory evaluation of skeletonized versus pedicled internal thoracic artery. Ann Thorac Surg 1999; 68:2164–2168.
13.Takami Y, Ina H. Effects of skeletonization on intra operative flow and anastomosis diameter of internal thoracic arteries in coronary artery bypass grafting. Ann Thorac Surg 2002; 73:1441–1445.
14.Calafiore AM, Vitolla G, Iaco AL, et al. Bilateral internal mammary artery grafting: midterm results of pedicled versus skeletonized conduits. Ann Thorac Surg 1999; 67:1637–1642.
15.Bical O, Braunberger E, Fischer M, et al. Bilateral skeletonized mammary artery grafting: experience with 560 consecutive patients. Eur J Cardiothorac Surg 1996; 10:971–975.
16.Athanasiou T, Crossman MC, Asimakopoulos G, et al. Should the internal thoracic artery be skeletonized? Ann Thorac Surg 2004; 77:2238-2246.
17.Mailis A, Chan J, Basinski A, et al. Chest wall pain after Aorto coronary bypass surgery using internal mammary artery graft: a new pain syndrome? Heart Lung 1989;18:553–558
18.Mailis A, Umana M, Feindel CM. Anterior intercostal nerve damage after coronary artery bypass graft surgery with use of internal thoracic artery graft. Ann Thorac Surg 2000;69:1455–1458
19.Wendler O, Tscholl D, Huang Q, et al. Free flow capacity of Skeletonised pedicled internal thoracic artery grafts in coronary artery bypass grafts. Eur J Cardiothorac Surg 1999; 15(3):247-250.
20.Behranwala A, Raja S, Dunning J. Is Skeletonised internal mammary artery harvest better than pedicle internal mammary harvest for patients undergoing coronary artery bypass grafting? ICVTS 2005.