ABSTRACT
This is a report of a 28-year-old female patient
neither pregnant, nor lactating and was previously healthy, not known to be
immunocompromized who presented with a two month history of a painful lump in
her right breast associated with low-grade fever. A thorough physical
examination, laboratory and radiological investigations were done including
breast mammogram, breast ultrasound and excisional biopsy from breast mass for
histopathological study; that showed caseating epithelioid granulomas with
giant cell and the Ziehl-Neelsen stain was negative.
Key words: Tuberculosis, Primary, Mastitis
JRMS December 2008; 15(3): 50-52
Introduction
Acute secondary tuberculous
mastitis is a rare disease mainly affecting young women, most often during
pregnancy and/or lactation. This entity was first described by Sir Astley
Paston Cooper in 1829 as "scrofulous swelling in the bosoms of young women
most of whom suffered from tuberculous cervical adenitis" and further
elaborated by Cohen in 1977.(1-3) Approximately 550 cases
have been described in the English literature, as secondary tuberculous
mastitis, but primary tuberculous mastitis is extremely rare and till now a few
cases have been reported internationally using a Medline search since 1960.
Many pathologists and clinicians are still unaware of this disease entity.
Clinically, the condition may closely mimic carcinoma, and histopathologic
appearance, if not recognized as granulomatous disease, may be
misinterpreted as a carcinoma, often with disastrous consequences.(4)
Case Report
A 28-year-old woman,
previously healthy, non-smoker, neither pregnant, nor lactating, having
oligomenorrhea diagnosed as polycystic ovary syndrome and treated with Metformen
850mg twice daily was referred to the Internal Medicine Clinic at Prince Rashed
Bin Al-Hassan Hospital (PRHH), Jordan on 22nd of September 2005. She presented with a painful mass lesion in
the right breast, which has been present since 25th July 2005,
coinciding two weeks after the return of her healthy, asymptomatic and
thoroughly investigated husband from Eritrea. She complained of severe
itching in her right breast around the areola, hotness and spikes of fever. On
examination, she looked healthy, well built, well nourished but anxious about
her condition. Blood Pressure was 110/70mmHg, pulse rate 110 beats per minute,
oral temperature was 37.9oC.
Systemic
examination revealed no significant abnormalities. No cervical or axillary lymphadenopathy, chest and heart examination was normal. On breast examination the nipple was retracted, showing sinus formation, the skin was hot, red and edematous with a peau d'orange appearance (Fig. 1). A huge, firm and tender 10x10cm nodule was palpated in the upper outer quadrant of the right breast. Abdominal examination was normal; no ascitis or hepatosplenomegaly were found. Examination of upper and lower extremities was normal, skin examination was normal.

Fig. 1.
The nipple was retracted, showing sinus formation, the skin was hot, red and
edematous with a peau d'orange appearance
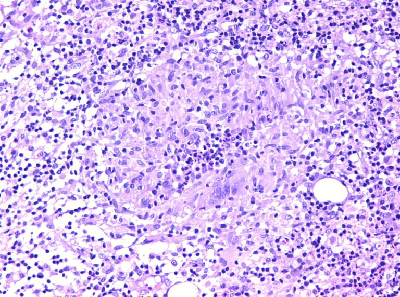
Fig. 2. Multiple caseating epitheliod granulomas with
Langhan's giant cells surrounded by sever acute and chronic inflammation
Complete
Blood Count, Prothrombin Time, activated Partial Thromboplastin Time, Liver
Function Tests (LFT), Kidney Function Tests (KFT), Electrocardiogram (ECG),
Chest-X-Ray (CXR), Urinalysis, Urine culture and abdominal ultrasound were
normal.
Tuberculin test, Human Immunodeficiency
Viral (HIV) and the Venereal Disease Research
Laboratory Slide (VDRL) tests were negative; also the Brucella test was
negative. IgG and IgM antibodies against both Toxoplasma and Cytomegalovirus
serology were negative as a remote possibility of this condition. Erythrocyte
Sedimentation Rate (ESR) was 56mm in the first hour. Mammogram showed focal
asymmetrical dense lesion in the upper outer quadrant of the right breast. Breast ultrasound showed an echogenic right
upper outer quadrant dense lesion with no collection. The provisional diagnosis
of breast abscess or malignancy was suggested and the patient was admitted to
hospital for fine needle aspiration (FNA) and excisional biopsy. FNA revealed
sheets of polymorphs and histiocytes in a hemorrhagic background showing
collection of epitheliod cells and multinucleated giant cells; the appearances were
those of an inflammatory granulomatous process. While the histopathological
study revealed multiple caseating epitheliod granulomas with Langhan's giant
cells surrounded by severe acute and chronic inflammation, the Ziehl-Neelsen
(ZN) stain for acid fast bacilli (AFB) was negative for
the time being, however the features were those of tuberculous mastitis (Fig. 2).
Pathological brownish fluid
was extracted on three occasions from the mass lesion and tested for
tuberculosis with the Polymerase Chain Reaction (PCR); the primers used were
AMS19 by amplification of IS6110 region, the amplification product is a 317bp
which codifies the IS6110 region and it is detected by electrophoresis on (pre-cast)
clearance gel containing ethidium bromide (a production of CLONIT S.r.l,
(Milan, Italy) and the last test was positive for tuberculosis.
The patient was started on
anti-tuberculosis therapy for 6 to 9 months. Also we investigated her husband; a
30-year-old soldier, smoker, healthy and asymptomatic, his physical examination
was unremarkable, chest X-Ray, CBC, KFT, LFT, urinalysis and urine culture were
normal. Tuberculin test was
positive, suggesting the "possibility" that her husband
could be the source of infection, but unfortunately we lost
his follow-up.
Discussion
Tuberculosis of the breast
is extremely rare and occurs in young, multiparous lactating women. Its
incidence in western countries is less than 0.1% of breast lesions examined
histologically and 3% to 4.4% of all breast diseases treated in the developing
world where TB is endemic.(5) On a clinical and pathological
bases five different patterns of tuberculous mastitis are described: acute
miliary tuberculosis mastitis, nodular tuberculosis mastitis, disseminated
tuberculosis mastitis, sclerosing tuberculosis mastitis and tuberculosis
mastitis obliterans.(6) Clinically, the above groups of
lesions can be mistaken for neoplasms. Nodular tuberculosis can be mistaken for
fibroadenoma or carcinoma while disseminated tuberculosis can be mistaken for
inflammatory carcinoma, and sclerosing tuberculosis can produce extensive
fibrosis and nipple retraction, being easily mistaken for scirrhous carcinoma.(4,7)
At present, mammographic
studies in addition to fine needle aspiration studies are not helpful for the
diagnosis of tuberculous mastitis. An
excisional biopsy is the most reliable for the definite diagnosis of
tuberculous mastitis.(8) The diagnosis, however, is very
difficult, especially in a number of pathologic processes such as
comedo-mastitis, which with its chronic inflammatory cells, is similar to
tuberculosis. In these situations, the demonstration of acid-fast bacilli is
mandatory for definite diagnosis. Overall, male breast tuberculosis is very
rare and only few male breast tuberculosis cases have been reported.(6)
In this case, many differential diagnoses were considered: breast abscess,
acute mastitis, sarcoidosis, fat necrosis, papilloma, fibroadenoma and
carcinoma. The excisional biopsy material revealed numerous caseating
epitheliod granulomas with Langhan's giant cells surrounded by severe acute and
chronic inflammation of the breast; those of tuberculous mastitis.(5)
There are three recognized
modes of spread of the tubercle bacilli to the breast: direct, lymphatic and
haematogenous. Rarely, infected sputum can reach the underlying breast through
superficial abrasions of the skin of the breast. In all cases bacilli infect
the ducts and spare the lobules. Dilated ducts of the breast in pregnant and
lactating women appear to be especially susceptible to infection. Retrograde
spread of infection from primary foci of disease in the lymph node (axillary, mediastinum, parasternal or cervical) to the
breast is also well recognized.(3,6)
The management of this case was
surgical and medical with anti-tuberculous therapy. A wedge resection was performed with a daily dressing but larger lesions should be treated with simple mastectomy.
Extra pulmonary TB is treated like pulmonary TB. A 6-month regimen is thought to be adequate;
in the first two months of therapy we start quadruple anti-tuberculous medication:
Isoniazide (INH) 300mg/d, Rifampicin (RMP) 600mg/d, Pyrazinamide (PZA) 500mg
twice/d and Streptomycin (STM) intramuscular injection 1g/d for the first two
weeks. After two months INH and RMP are given up to six months. Treatment of TB
mastitis is best achieved by conservative surgery supported with
anti-tuberculosis drugs.
Upon follow-up two months
later signs of recovery were noted. Her physical examination was unremarkable,
both breasts ultrasound was normal, FNA follow-up was also normal. Hence, the combination of drug therapy and
limited excision of diseased breast tissue is a method of choice.(8)
Conclusion
TB can affect virtually any
organ system in the body and can be devastating if left untreated. Uncommon
sites and ability to mimic other diseases clinically and radiographically leads
to diagnostic and therapeutic delay. A high level of suspicion is required
especially in high-risk populations and endemic areas.
References
1. Cooper
A. Illustrations of the
diseases of the breast. Part I.
London:
Longman, Orme, Brown and Green, 1829:73
2.
Mann
CV, Russell RCG, Wiliams NS. The breast. In: Man CV, et al editors, Baily and Love's: Short
Practice of Surgery. 22ed edition, Chapman and Hall Medical London,
1995: 548-549.
3.
Cohen
C. Tuberculous mastitis. A
review of 34 cases. S Afr Med J
1977; 52(1):12-14
4. Da
Silva B, Dos Santos LG, Costa CGP, Borges AS. Primary tuberculosis of the breast mimicking
carcinoma. Am J Trop Med Hyg 2005;
73: 975-976.
5. Bani-Hani
KE, Yaghan RJ, Matalka II, Mazahreh TS. Tuberculous mastitis: A disease not to be
forgotten. Int J Tuberc Lung Dis 2005;
9(8):920-925.
6.
Talei
A.R. Primary tuberculosis of
the male breast: A case report. Irn J
Med Sci 1999; 24(1&2):74-76.
7. Shinde
SR, Chandawarkar RY, Deshmukh SP.
Tuberculosis of the breast masquerading as carcinoma: A study of 100 patients. World
J Surg 1995; 19: 379-81.
8.
Al-Marri
MRHA, Almosleh A, Almoslmani Y.
Primary tuberculosis of the breast in Qatar: Ten year experience and review
of the literature. Eur. J of Surgery
2000; 166(9): 687-690.