Abstract
Objective:
To identify the pattern of glycemic, lipid and
blood pressure control among a cohort of diabetic patients referred to Queen
Alia Heart Institute for further evaluation of coronary artery disease.
Methods:
This is a descriptive study conducted at Queen Alia Heart Institute
between 1/12/2004
and 1/9/2005. All
newly referred diabetic patients (N=112) to Monday official referral clinic at
the centre during this period were enrolled. A specially designed record form
was completed including demographics, risk factors for coronary artery disease,
medications, diabetes care giver name and the type of culprit cardiovascular
event. Blood pressure was measured, and fasting lipid panel, blood sugar, and
HbA1c were drawn.
Results: Only about one fourth of the study population
had optimal glycemic and blood pressure control. Optimal body mass index was present in only 13.9% of patients
(lower in females 7.5%). Smoking was prevalent in our study population (41.1%).
Optimal low density lipoprotein, high density lipoprotein and triglyceride
levels were obtained only in 33%, 22% and 34% of patients, respectively. Usage of recommended medications for secondary
prevention was relatively low: aspirin
(52.7%), angiotensin converting enzyme inhibitors, angiotensin receptor blockers
(55.4%), beta blockers (59.8%) and HMG-coA
reductase inhibitors (statins) (79.5%). Over
half of the patients (51%) could not name their diabetes care-giver.
Conclusion: Diabetic patients referred to Queen Alia Heart
Institute for further evaluation of coronary artery disease have poor glycemic,
blood pressure and lipid control prior to their referral. More emphasis on
these issues at the level of primary as well as secondary health care levels is
imperative to delay the progression of atherosclerosis and reduce adverse cardiovascular
events in these patients.
Key words: Coronary artery disease, Diabetic patients, Glycemic
control
JRMS
March 2010; 17(1): 21-27
Introduction
Diabetes mellitus (DM) affected approximately 171
million patients worldwide in 2000 (2.8% of the population). The large majority
of these patients are type 2 diabetics (90-95%). By the year 2030, the diabetic
population is expected to reach 366 million (4.4%). The projected increase is
attributed to demographic changes as well as the increasing rate of obesity.(1-3)
The adult treatment panel of the National Cholesterol
Education Program (NCEP) considered type 2 diabetes
as a coronary artery disease (CAD) risk equivalent.(4,5) Both
accelerated atherosclerosis and the increased adverse outcomes after coronary
intervention have been attributed to various physiological mechanisms related
to diabetes.(6-8) A
growing body of evidence has demonstrated an association between tight glycemic
controls on macrovascular endpoints, although the effect was unclear in the United Kingdom
Prospective Diabetes Study.(9-13)
Moreover, recent studies have demonstrated that aggressive treatment of DM may
improve the clinical outcome after PCI.(14,15) In fact, the reduction of the increased
cardiovascular risk in diabetic population requires a multifactorial approach in
addition to glycemic control. There is substantial amount of evidence in the
literature demonstrating the beneficial effects of tight control of multiple
risk factors in them. These modifiable factors include: blood pressure, dyslipidemia, anti-platelet
therapy, obesity and smoking status.(16)
The objective of this study was to identify the pattern of glycemic, lipid
and blood pressure (BP) control among a cohort of diabetic patients referred to
Queen Alia Heart Institute (QAHI) for further evaluation of their CAD.
This study represents an essential step in evaluating and promoting the proficiency
of diabetic patient care among primary and secondary care physicians in Jordan.
Methods
This is an observational study conducted in Monday
referral cardiology clinic at QAHI –Amman
/Jordan. The study enrolled 112 consecutive diabetic patients (59 males, 53
females) referred for further evaluation of CAD who were seen d between
1/12/2004 and 1/9/2005 and evaluated by one consultant (OA) and three
cardiology specialists covering the mentioned clinic. Diabetic patients were identified as patients
undergoing treatment with diet, insulin or oral hypoglycemic medications. Exclusion
criteria include only patients who could not offer complete information and
those with uncertain diagnosis for DM.
Data collected included risk factors for CAD and
clinical characteristics (age, gender, history of hypertension, dyslipidemia,
smoking, family history of CAD and type of clinical presentation, previous
history of stroke or transient ischemic attack). Patients were also asked
whether they knew the name of their diabetes care-giver. The prior use of statins, β blockers, ACEI
and/or ARB, and aspirin were also
evaluated.
During clinical examination, measurement of blood
pressure (BP) was performed using a standard cuff technique using mercury
sphygmomanometer to the nearest 5mmHg for all subjects. Weight and height were
measured with ordinary scales to the nearest kilogram and centimeter, without
footwear and in standing position. Body mass index (BMI) was then
calculated using this formula (BMI= weight in Kg/height
in m2. Finally, blood was withdrawn for all patients regarding HBA1C
and fasting blood sugar (FBS) to assess glycemic control and for lipid panel to
assess control of dyslipidemia. The
following parameters were used to define optimal treatment in these patients
according to recent guidelines.(17,18)
- Optimal glycemic control: HBA1C≤7%.
- Optimal lipid control: LDL-C≤100
mg/dl, TG ≤ 150mg/dl, and HDL-C≥40
mg/dl (50mg/dl in women).
- Blood pressure ≤130/80mmHg in diabetic patients (≤120/80 after MI).
- Prophylactic daily therapy with aspirin for diabetic patients with CAD.
- BMI≤25 Kg/m2.
- Current non-smoking status.
Continuous variables were expressed as mean values ±
SD and discrete variables as absolute values and percentages.
Results
The percentages of those who achieve optimal as well
as suboptimal goals for various studied factors are shown in Fig. 1.
Demographic data (Table I) reveal the high frequency of many traditional risk
factors among our study population: hypertension (63.4%), smoking (41.1%),
overweight (36.6%) and obesity (50%). Positive family history for CAD was
present in one third of patients while previous history of stroke and TIAs was
infrequent (6.3%). Fifty seven patients (51%) were unaware of their diabetes
care-giver’s name.
The overall mean BMI
was 30.2 ± 5.6 Kg/m2 (29.1± 5.1 in males, 30.4 ± 6.1 in females).
Optimal BMI ≤ 25 were obtained
only in 13.4% of patients (18.6% in males, 7.5% in females), as demonstrated in
Table II.
Only about a quarter of the study population had optimal
glycemic control prior to presentation as clearly shown in Tables III and IV.
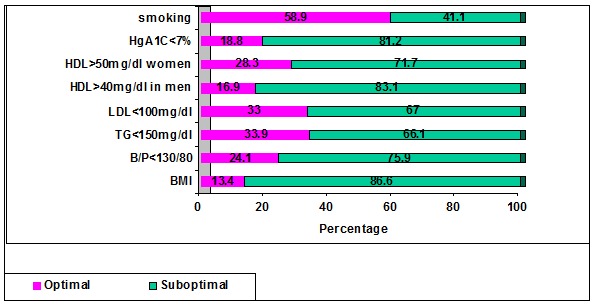
Fig. 1. The percentage of patients
who achieved optimal or suboptimal treatment goals
Table I. Risk factors and clinical
characteristics of our study population.
|
Item
|
Male
|
Female
|
Total
|
|
Total No. of patients
|
59
|
53
|
112 (100%)
|
|
Age (yrs)
|
59 ± 7.9
|
62 ± 9.1
|
60 ± 8.7
|
|
BMI (Kg/m2)
|
29 ± 5.1
|
30.4 ± 6.1
|
30.2 ± 5.6
|
|
Current smoking
|
38 (64.4%)
|
8 (15.1%)
|
46 (41.1%)
|
|
Family history of CAD
|
20 (33.9%)
|
16 (30.2%)
|
36 (32.1%)
|
|
Hypertension
|
34 (57.6%)
|
37 (69.8%)
|
71 (63.4%)
|
|
Previous stroke
|
5 (8.5%)
|
2 (3.8%)
|
7 (6.3%)
|
|
Angina
|
20 (33.9%)
|
25 (47.2%)
|
45 (40.2%)
|
|
Unstable angina
|
15 (25.4%)
|
10 (18.9%)
|
25 (22.3%)
|
|
Post-MI
|
15 (25.4%)
|
7 (13.2%)
|
22 (19.6%)
|
|
Other presentation
|
9 (15.3%)
|
11 (20.7%)
|
20 (17.9%)
|
|
Treatment with diet alone
|
3 (5%)
|
4 (7.5%)
|
7 (62.5%)
|
|
Insulin
|
14 (23.7%)
|
10 (18.9%)
|
24 (21.4%)
|
|
Oral agents
|
36 (61.0%)
|
29 (54.7%)
|
65 (58.0%)
|
|
Insulin and oral agents
|
6 (10.2%)
|
10 (18.9%)
|
16 (14.3%)
|
Very
bad control (A1C > 9.5%) was observed in around a third of the study population.
Table V shows that only 24.1% of patients had optimal
B/P control (less in females). The overall mean SBP
was 149 ± 24.8 mmHg and DBP 87 ± 11.3 mmHg. The mean values in previously known
hypertensive patients were 153 ± 25.5 mmHg for SBP
and 88.2 ± 12.7 mmHg for DBP ( males: 148.6 ± 29.2/ 86.1 ± 11.7, females :
157.0 ± 21.4 / 90.1 ± 12.7). Among the 24 patients who denied having
hypertension, 10 patients (40.2%) were hypertensive (BP ≥ 160/90) during
clinical examination.
Optimal LDL,
HDL and triglyceride levels were noted
in 37 patients (33%), 25 patients (22.3%) and 38 patients (33.9%) respectively.
See Tables IV, IIV, IIIV.
Many medications shown to decrease the total and cardiac
mortality in such a subset of patients were under-prescribed. Aspirin, ACE inhibitors, β blockers and statins were not
administered in 52.7%, 55.4%, 59.8% and 79.5% of patients, respectively (See Table
IX).
Discussion
Only around a quarter of the study population had
optimal glycemic control prior to presentation. Similar bad control was seen in
previously reported trials.(19-21)
A growing body of evidence has shown recently an
association between tight glycemic control and macrovascular endpoints.(9-13)
Table II. Values of body mass indices of our study population
|
Value
Kg/m2
|
< 25 Optimal (%)
|
25.1-29.9
Overweight
(%)
|
> 30
Obese (%)
|
Total (%)
|
|
Male
|
11(18.6)
|
25(42.4)
|
23 (39)
|
59 (100)
|
|
Female
|
4 (7.5)
|
16 (30.2)
|
33 (62.3)
|
53 (100)
|
|
Total
|
15 (13.4)
|
41 (36.6)
|
56 (50)
|
112 (100)
|
Table III. Level of hyperglycemic
control according to values of HBA1C
|
HbA1C
|
< 7%
Optimal Control (%)
|
>
7%-<8.5%
Good (%)
|
>8.5-<9.5%
Fair (%)
|
> 9.5
Uncontrolled (%)
|
Total(%)
|
|
Male
|
10 (16.9)
|
15 (25.4)
|
16 (27.1)
|
18 (30.5)
|
59 (52.7)
|
|
Female
|
11 (20.8)
|
15 (28.3)
|
10 (18.9)
|
17 (32.1)
|
35 (47.3)
|
|
Total
|
21 (18.8)
|
30 (26.8)
|
26 (23.2)
|
35 (31.3)
|
112 (100)
|
Table IV. Level of hyperglycemic
control according to values of fasting blood sugar
|
Total (%)
|
> 155 (%)
|
126-155 (%)
|
<126 (%)
|
FBS Mg/dl
|
|
59 (100)
|
33 (55.9)
|
15 (25.4)
|
11 (18.7)
|
Male
|
|
53 (100)
|
29 (54.7)
|
10 (18.9)
|
14 (26.4)
|
Female
|
|
112 (100)
|
62 (55.4)
|
25 (22.3)
|
25 (22.3)
|
Total |
Khaw and his colleagues(10) demonstrated that a 1%
increase in HbA1C was associated with 38% increase in cardiovascular mortality.
During 10 years of post United Kingdom Prospective Diabetes Study follow-up,
Holman and his colleagues(12) observed emergent risk
reductions for MI and death from any cause despite modest differences in
glycated hemoglobin. Moreover, recent studies showed that aggressive treatment
of diabetes to achieve HBA1C levels ≤ 7% has a significant role in reducing the
risk of restenosis and rates of target vessel revascularization and may improve
the clinical outcome after PCI.(14,15)
Demographic data clearly demonstrated the high
frequency of smoking habit among our male population (41.1% who were current
smokers). Multiple large prospective trials have demonstrated a two-fold
increase in the relative risk for all-cause mortality in the smoking versus
non-smoking diabetic population.(22-23)
Optimal BMI was found in only in 13.4% of patients.
This low percentage is an extremely important issue, as numerous studies have
demonstrated increased mortality rates in individuals with a BMI ≥ 30
Kg/m2.(19, 24,25)
To alter what is otherwise a fairly dismal prognosis,
out-patient education programs should be used as an integral part of
patient-care in DM, aiming at encouraging lifestyle modification (cessation of
smoking, weight reduction and promotion of physical activity), in addition to
coordination of nutritional therapy with dieticians.
Systemic hypertension was very frequent in our study
population (63.4%), far exceeding the previously reported prevalence rates of 39-42%.(26-28) The current antihypertensive treatment targets are
< 130/80 mmHg in diabetic patients and < 120/80 after myocardial
infarction.(29-32)
From the 24 patients who denied having
prior history of hypertension, 10 patients (40.2%) were found hypertensive (BP
≥ 160/90) during clinical examination. Only 24.1% of patients had optimal B/P
control (less in females). Current guidelines recommend the use of ACE inhibitors or ARB's
as first line therapy in hypertension treatment in diabetic patients.(17,18,33)
Unfortunately, more than half of the patients were neither on these medications
nor on β blockers upon referral.
Poor BP control demonstrated among our hypertensive
diabetic patients is similar to previously reported international and regional
studies.(19-21,34,35) Although we did not look for the
non-compliance rate which is the greatest obstacle to good BP in hypertensives(36)
our findings strongly suggest that referring physicians are underutilizing
appropriate medical therapies and therefore we recommend the implementation of
management guidelines in order to achieve the required objective.
There
is compelling evidence from literature that suggests that statins confer
cardiovascular risk reduction to both high and low-risk diabetic patients.(37)
The HPS (Heart Protection Study) demonstrated that cholesterol-lowering therapy
was beneficial for people with DM even if they did not already have a history
of CAD or high cholesterol concentrations.(38) Both the STEMI
and the NSTEMI/UA ACC/AHA guidelines consider statin drugs class I
recommendation regardless of baseline
Table V. Distribution of patients
according to blood pressure readings
|
B/P Range
|
< 130/80 (%)
|
130-160 /80-90 (%)
|
> 160/> 90
|
> 160/< 90
|
<160/>90
|
Total
|
|
Male
|
17 (28.8)
|
32 (54.2)
|
7 (11.9)
|
2 (3.4)
|
2 (1.7)
|
59
|
|
Female
|
10 (18.9)
|
23 (43.4)
|
13 (24.5)
|
3 (5.7)
|
4 (7.5)
|
53
|
|
Total
|
27 (24.1)
|
55 (49.1)
|
20 (17.8)
|
5 (4.5)
|
5 (4.5)
|
112
|
Table VI. Low density lipoprotein
levels in our study population
|
LDL level mg/dl
|
<
100 (%)
|
100-129
(%)
|
>130 (%)
|
Total (%)
|
|
Male
|
21 (35.6)
|
18 (30.5)
|
20 (33.9)
|
59 (100)
|
|
Female
|
16 (30.2)
|
10 (18.9)
|
27 (50.9)
|
53 (100)
|
|
Total
|
37 (33)
|
28 (25)
|
47 (42)
|
112 (100)
|
Table VII. High density lipoprotein levels
in our study population
|
LDL level mg/dl
|
> 40 males & > 50
females (%)
|
> 40 males & > 50
females (%)
|
Total (%)
|
|
Male
|
10 (16.9)
|
49 (83.1)
|
59 (100)
|
|
Female
|
15 (28.2)
|
38 (71.7)
|
35 (100)
|
|
Total
|
25 (22.3)
|
87 (77.7)
|
112 (100)
|
Table VIII. Triglyceride levels
|
TG level mg/dl
|
<150 (%)
|
> 150 (%)
|
Total
|
|
Male
|
22 (37.3)
|
37 (62.7)
|
59 (100)
|
|
Female
|
16 (30.2)
|
37 (69.8)
|
35 (100)
|
|
Total
|
38 (33.9)
|
74 (66.1)
|
112 (100)
|
Table IX. Underpresciption of medications
|
Item
|
Yes (%)
|
No (%)
|
|
ACEI intake
|
50 (44.6)
|
62 (55.4)
|
|
B-Blockers
|
45 (40.2)
|
67 (59.8)
|
|
Statins
|
23 (20.5)
|
89 (79.5)
|
|
Aspirin intake
|
53 (47.3)
|
59 (52.7)
|
LDL Cholesterol. LDL targets of less than 70 mg/dl are also
considered reasonable.(39-41) Unfortunately, despite the
effectiveness of statins in altering cardiovascular mortality, several prior
studies have documented low treatments rates in patients with established CAD.(19,
42-44)
In
our study statins were prescribed only to about one fifth of our patient
population. Only about one third of patients achieved the target LDL values (<100 mg/dl), a finding that is in other similar
studies.(21,37,45,46) Moreover, only 22 % and 34% of patients
met the existing guidelines for HDL
levels and TG levels respectively.
Contemporary guidelines recommend prophylactic therapy
with aspirin for diabetic patients with CAD(6, 17,18)
unfortunately, fewer than half of the patients with CAD in this study were
treated with aspirin suggesting, again, deficiencies in applying the
appropriate guidelines by referring physicians.
Our data suggest that both glycemic control as well as
numerous modifiable cardiovascular risk factors in diabetic patients referred
to our centre are not adequately treated according to current guidelines and
may highlight deficiencies in cardiovascular risk factor modification in the
diabetic population as a whole. The low level of control reported is a clear
signal that current paradigms of care delivery are inadequate.
Despite being a single centre observational study, we
feel that our findings are broadly applicable because our institution has a
very broad patient base. In this study, the patient
sample was drawn from out-patients of a tertiary care centre in a metropolitan
city of the country, where it may be expected that patients have access to
higher standards of care than the rest of the country, but many of the patients
were living outside the city and had attended
The
relatively small sample size is a limitation to generalize our results to the
community, but nevertheless we feel that important information is gathered from
this subset, which is fairly typical regarding the type of patients we come
across.
To promote patient-care in diabetic patients,
combining strategies to combat more effectively cardiovascular disease is
extremely essential.
We should encourage out-patient education programs that
aim at increasing patient knowledge about the disease, motivating the patient
to comply with complex treatment scheme, encouraging lifestyle modification and
better coordination with dieticians.
From physician standpoint, we should urge primary as
well as secondary care physicians to read and follow the guidelines that are
generally published after a body of evidence is present in the literature.
Lastly, the deficiencies in diabetic patient's care can be controlled by
introducing a checklist (flow sheet) or electronic medical records as reminders
to referring physicians.
Conclusion
Our efforts to face the current epidemic of DM and its
cardiovascular consequences must include improved compliance to lifestyle
measures and drug therapy through patient and community counselling as well as
sensibilization of the medical profession to the importance of primary and
secondary CAD prevention through appropriate long-term prescription of
evidence-based therapies.
References
1.
Sicree R, Shaw JE, Zimmet PZ. The global burden of diabetes.
In: Gan D., editor. Diabetes Atlas. 2nd ed. Brussels, Belgium:
International Diabetes Federation; 2003. pp. 15–71.
2.
Wild S, Roglic G, Green A, et al. Global prevalence of diabetes:
estimates for the year 2000 and projections for 2030. Diabetes Care
2004; 27:1047-53
3. Boyle JP,
Honeycutt AA, Narayan KMV, et al. Projection of diabetes burden through
2050: impact of changing demography and disease prevalence in the US. Diabetes
Care 2001 ; 24:1936-40.
4. Anon. Executive summary of the third report of
the National Cholesterol Education Program (NCEP) (Adult Treatment Panel 111
Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol
in Adults) JAMA 2001; 285:2486-97.
5. Haffner SM, Letho S, Ronnemaa T, et al. Mortality from coronary heart disease in subjects with type 2 diabetes
in non diabetic subjects with and without prior myocardial infarction. N
Engl J Med 1998; 339:229-34.
6.
Colwell JA, Nesto RW. The platelet in diabetes: focus
on prevention of ischemic events. Diabetes Care 2003; 26: 2181-8.
7.
Aronson D, Bloomgarden Z, Rayfield EJ.
Potential mechanisms promoting restenosis in diabetic patients. J Am
Coll Cardiol 1996; 27: 528-35.
8.
Abizaid A, Kornowski R, Mintz GS, et al. The influence of diabetes
mellitus on. Acute and late clinical outcomes following coronary stent
implantation. J Am Coll Cardiol 1998; 32: 584-9.
9.
Intensive blood-glucose control with sulphonylureas or insulin
compared with conventional treatment and risk of complications in patients with
type 2 diabetes (UKPDS 33): UK Prospective Diabetes Study Group. Lancet 1998; 352:837–853.
10. Khaw KT, Wareham N, Luben R, et al. Glycated haemoglobin, diabetes, and mortality in men in Norfolk cohort of European prospective investigation of cancer and nutrition (EPIC-Norfolk).BMJ. 2001; 322:15-8.
11.
Stettler C, Allemann S, Juni P, et al. Glycemic control and
macrovascular disease in types 1 1nd 2 Diabetes mellitus: Meatanalysis of randomized
trials. Am Heart J 2006; 152:27-38.
12. Holman RR, Paul
SK, Bethel MA, et al. 10 year follow-up of intensive glucose
control in type 2 diabetes. N Engl J Med 2008; 359:1577-1589.
13. Dormandy JA, Charbonnel B, Eckland DJ, et al. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised controlled trial. Lancet 2005; 366:1279-89.
14.
Corpus RA, George PB, House JA, et al.
Optimal
glycemic control is associated with a lower rate of target vessel
revascularization in treated type 2 diabetic patients undergoing elective
percutaneous coronary intervention. J Am Coll Cardiol 2004; 43:8-14.
15.
Mazeika Peter, Prasad Neeraj, Bui Sanh, et
al.
Predictors of angiographic restenosis after coronary intervention in patients
with diabetes mellitus. AHJ 2003; 145:1013-21.
16.
Gaede P, Vedel P, Larsen N, et al. Multifactorial intervention and
cardiovascular disease in patients with type 2 diabetes. N Engl J Med
2003; 348: 383-93.
17.
American Diabetic Association. Standards of medical care in diabetes. Diabetes
Care 2006; 29:S4-42.
18.
Canadian Diabetes Association. Clinical practice guidelines for the
prevention and management of diabetes in Canada. Can J Diabetes 2003; 27:S58-65.
19.
George PB, Tobin KJ, Corpus RA, et al.
Treatment
of cardiac risk factors in diabetic patients: how well do we follow the
guidelines? Am Heart J 2001; 142:875-63.
20.
Koro CE, Boialin SJ, Bourgeois N, Fedder
DO.
Glycemic control from 1988 to 2000 among U.S. adults diagnosed with type 2
diabetes: a preliminary report. Diabetes Care 2004; 27:17-20.
21.
Saydah SH, Fradkin J, Cowie CC. Poor control of risk factors
for vascular disease among adults with previously diagnosed diabetes. JAMA
2004; 291:335-42.
22.
Ford ES, De Stefano F. Risk factors for mortality from
all causes and from coronary heart disease among persons with diabetes:
Findings from the National Health and Nutrition Examination Survey ι.
Epidemiological follow-up study. Am J Epidemiol 1991; 133:1220-30.
23.
Stamler J, Vaccaro O, Neaton JD, et al.
Diabetes,
other risk factors, and 12 yr cardiovascular mortality for men screened in the
multiple risk factor intervention trial. Diabetes Care 1993; 16:434-44.
24. Troiano RP,
Frongillo EA Jr, Sobal J, et al. The relationship between body weight and
mortality: a quantitative analysis of combined information from existing
studies. Int J Obes 1996;20: 63-75.
25.
Manson JE, Stampfer MJ, Hennekens CH, et
al. Body weight and longevity: a reassessment. JAMA 1987;
257:353-8.
26.
Epstein M, Sowers JR. Diabetes mellitus and
hypertension. Hypertension 1992; 19:403-418.
27.
The Hypertension in Diabetes Study Group. Hypertension in Diabetes study
(HDS):1.Prevalence of hypertension in newly presenting type 2 diabetic patients
and the association with risk factors for cardiovascular and diabetic
complications; 2. Increased risk of cardiovascular complications in
hypertensive type 2 diabetic patient's. J Hypertens 1993; 11: 309-319.
28.
Wokoma FS. Hypertension in non-insulin
dependent diabetic Nigerians: a comparative analysis of normotensive and
hypertensive subgroups. Diabetes International 1999; 9: 57-58.
29.
Hansson L, Zanchetti A, Carruthers SG, et
al. For the HOT
Study Group. Effect of intensive blood pressure lowering and low dose aspirin
in patients with hypertension: principal results of the Hypertension Optimal
Treatment (HOT) randomized trial. Lancet
1998; 351:755-762.
30. Gerstein
HC, Yusuf S, Mann JFE, et al. Effects of ramipril on
cardiovascular and microvascular outcomes in people with diabetes mellitus:
Results of the HOPE and MICRO-HOPE substudy. Lancet 2000; 355:253-9.
31. Lindholm
LH, Ibsen H, Dahlof B, et al. For the Life Study Group.
Cardiovascular morbidity and mortality in patients with diabetes in the
losartan intervention for endpoint reduction in hypertension study (LIFE): a randomized trial against atenolol. Lancet
2002; 359:1004-10.
32. UK
Prospective Diabetes Study Group: Tight blood pressure control
and risk of macrovascular and microvascuar complications in type 2 diabetes
(UKPDS 38). BMJ 1998; 371: 703-713.
33. Chobanian
AV, bakris GL, black HR, et al. seventh report of the Joint
National Committee on prevention, detection, evaluation and treatment of high
blood pressure. Hypertension 2003; 42; 106-52.
34.
Konzem SL, Devore VS, Bauer DW.
Controlling hypertension in patients with Diabetes. Am Fam Physician
2002; 66:1209-1214.
35.
Akbar DH, Al-Ghamdi AA. Is hypertension well controlled
in hypertensive diabetics? Saudi Med J 2003; 24: 356-360.
36.
Chockalingam A, Backer M, Campbell N, et
al.
Adherence to management
of high blood pressure: recommendations of the Canadian
coalition for high blood pressure
prevention and control. Can J Public Health 1998; 89:15-31.
37.
Kearney PM, Blackwell L, Collins R, et
al.
Efficacy of cholesterol lowering therapy in 18,686 people with diabetes in 14
randomized trials of statins: a meatanalysis. Lancet 2008; 371:117-25.
38.
Colins R, Armitage J, Parish S, et al. MRC/BHF Heart protection study
of cholesterol-lowering with simvastatin in 5963 people with diabetes: a
randomized placebo-controlled trial. Lancet 2003; 361:2005-16.
39.
Antman EM,Hand M, Armstrong PW, et al. 2007 Focused update of the
ACC/AHA 2004 guidelines for the management of patients with ST-elevation
myocardial infarction: a report of the American College of Cardiology/ American
Heart association Tassk Force on Practice Guidelines. J Am Coll Cardiol 2008; 51:210-47.
40.
Anderson JL, Adams CD, Antman EM, et al. ACC/AHA guidelines for the
mangment of patients with unstable angina/ non-ST-elevation myocardial
infarcyion. J Am Coll Cardiol
2007; 50:e1-157.
41.
Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipid
lowering with statins after acute coronary syndromes. N Engl J Med 2004;
350:1495-504.
42.
Grundy SM, Benjamin IJ, Burke GL, et al. Diabetes and cardiovascular
disease: a statement for healthcare professionals from the American Heart
Association. Circulation 1999; 100:1134-46.
43.
Sueta CA, Chowdhury M, Boccuzzi SJ, et al. Analysis of the degree of
undertreatment of hyperlipidemia and congestive heart failure secondary to
coronary artery disease. Am J Cardiol1999; 83:1303-7.
44.
Frolkis JP, Zysanski SJ, Schwartz JM, Suhan
PS.
Physician noncompliance with the 1993 National Cholesterol Education Program
(NCEP-ATP I I) guidelines. Circulation
1998; 98:851-5.
I) guidelines. Circulation
1998; 98:851-5.
45.
Pearson TA, Laurora I, Chu
H, Kafonek S. The lipid treatment Assesment Project (L-TAP): multicenter survey to evaluate the
percentages of dyslipidemic, patients receiving lipid-lowering therapy and
achieving low-density lipoprotein cholesterol goals. Arch Inern Med 200;
160:459-67.
46.
Jabbar A, Hameed A, Chawla R, Akhter J. How well do Pakistani patients
and physicians adhere to standards of diabetes care? Int J Diab 2007;
27:93-6.