Abstract
Objectives: To assess the efficacy and safety of posterior
subtenon triamcinolone acetonide injection for the treatment of diabetic
cystoid macular edema.
Methods: This
prospective, randomized comparative trial included diabetic patients with
cystoid macular edema involving 79 eyes. Forty one eyes were randomly given
posterior subtenon triamcinolone acetonide injection while the remaining 38
eyes served as a control group. The eligibility criteria for this study
included patients with clinically and angiographically detectable cystoid
macular edema during the past six months, glycosylated hemoglobin not more than
8.5% and history of previous laser treatment not earlier than three months. All
eyes of posterior subtenon triamcinolone acetonide injection group received
40mg of triamcinalone acetonide through a superotemporal approach in the
outpatient clinic. After injection, the visual and anatomical responses were
observed at weeks 1, 3, 6, 8, 12, 16, 20 and 24. Intraocular pressure, incidence
of reinjection and complications were also noted.
Results: At one week after injection, all injected eyes showed
significant visual acuity improvement from baseline measurements (p<0.001)
and 88% of them showed clinical serous macular edema regression. The most
significant improvement in logarithm of the minimum angle of resolution visual
acuity was noted at month two post injection. During the next four months a
gradual increase in logarithm of the minimum angle of resolution acuity was
noted. Comparison between the two groups, showed significant difference of mean
logarithm of the minimum angle of resolution acuity at one week after injection
and during the subsequent study visits. After injection, recurrence of cystoid
macular edema was noted in nine eyes (22%) at a mean time of 5.25±0.71 months. Two
eyes (4.9%) developed rise of intraocular pressure (>20mmHg) at the first
week post injection and were treated with antiglaucoma drugs for a mean time of
5.5±1.41 months. Another two eyes had localized subconjunctival hemorrhage at
the site of injection.
Conclusion: Posterior
subtenon triamcinolone acetonide injection of 40mg triamcinolone acetonide through
a superotemporal approach appears to be safe and effective for short-term
management of diabetic cystoid macular edema.
Key words: Cystoid
macular edema, Posterior subtenon injection, Triamcinalone acetonide.
JRMS
March 2010; 17(1): 62-66
Introduction
Macular edema is one of the leading causes of vision loss
in patients with diabetic retinopathy.(1,2) Cystoid macular edema
(CME) occurs by leakage from the perifoveal retinal capillaries. A variety of
approaches to the treatment of CME have been attempted with a variable degree
of success. These options have
included
topical and oral steroids, nonsteroidal anti-inflammatory agents, and laser
photocoagulation treatment.(3) In recent years, intravitreal injection of
triamcinalone acetonide (TA) has been reported to improve visual acuity and to
reduce the macular thickness in eyes with diffuse macular edema.(4-6) However, the risk of complications such as
elevation of intraocular pressure, endophthalmitis, intraocular hemorrhages,
and detachment of the retina was reported.(7-9) Posterior subtenon injection of steroids
proved to be effective in the treatment of diffuse diabetic macular edema.(10,11)
This approach is less invasive than intravitreal injection with a low risk of
complications and appears to deliver equivalent therapeutic quantities of TA to
the retina.(12-14) Bakri et al.,(15)
reported improvement of visual acuity of eyes with refractory diabetic macular
edema after posterior subtenon triamcinolone acetonide injection (PSTI) of TA. Other
researchers reported that eyes with refractory diabetic macular edema subjected
to PSTI did not show significant changes of visual acuity from the baseline measurements.(16,17)
The purpose of this study was to assess the efficacy and
safety of posterior subtenon triamcinolone acetonide injections for the
treatment of diabetic cystoid macular edema.
Methods
Seventy nine diabetic patients
(79 eyes) with cystoid macular edema were enrolled in a prospective, randomized
comparative trial between February 2005 and November 2007. They were 43 males
and 36 females, aged between 50 and 71 years (mean 61.16), with type two
diabetes mellitus. All patients were phakic with moderate to severe
nonproliferative diabetic retinopathy. Forty one eyes were randomly given PSTI while the remaining 38 eyes served as a
control group. In all studied eyes, the best corrected logarithm of the minimum
angle of resolution (logMAR) visual acuity was assessed using the Early
Treatment Diabetic Retinopathy Study (ETDRS) charts. CME
was defined by central thickening with intraretinal cystoid spaces revealed
with slit-lamp biomicroscopy using a 78-diopter non-contact lens and by
petaloid appearance of fluorescein leakage on fluorescein angiography. The
intraocular pressure was measured using Goldman applanation tonometer. Exclusion
criteria included eyes with history of CME
of more than 6 months, history of grid laser photocoagulation treatment up to three
months prior to the injection, pre-existing glaucoma and glycosylated hemoglobin
(HbA1c) of more than 8.5%. For the posterior subtenon injection, the patient was
placed in a semi setting position and after instillation of 0.4% oxybuprocaine
surface anesthesia eye drops the patient was directed to look in the extreme
inferonasal field of gaze. One milliliter of a 40 mg/ml of TA was given through
the superotemporal forniceal conjunctiva using a 25-gauge needle, 5/8 inch
length, on a 3ml syringe. The needle penetrated the conjunctiva and Tenon's
capsule with the bevel toward the globe and was advanced toward the macular
area, taking care to remain in contact with the globe until the hub was firmly
pressed against the conjunctival fornix and then the corticosteroid was slowly
injected. After initial examination and/or injection, all eyes were scheduled
for follow-up examination at weeks 1, 3, 6, 8, 12, 16, 20, and 24. Patients
were evaluated on basis of slit-lamp biomicroscopy, visual acuity, and Intraocular
pressure (IOP). In addition, fluorescein angiography was performed before the
treatment and after six months (final visit).
The significance of the
difference between the pre-treatment and post treatment data was assessed by
the two-tailed Student’s t test. The data
are presented as mean (SD). P< 0.05 was considered to be statistically
significant.
Results
The mean age of patients
(±SD) was 61.16±5.96 years for PSTI group and 59.58±5.19 years for control
group, with a range of 50 to 71 years. Patient’s characteristics are shown in
Table I.
The mean baseline visual
acuity was not significantly different between the two groups (P<0.1). The
change in mean (SD) visual acuity at studied groups during the observational
period is illustrated in Table II and Fig. 1.
The difference in mean
LogMAR best corrected visual acuity (BCVA) between the injected eyes and those
not injected becomes significant after the first week of observation
(p<0.001). In the next visits the difference in LogMAR acuity continues to
increase significantly between the studied groups and reaches its maximum on
the second month of observation (t=14, p<0.001). At the end of observation (month
6) the mean LogMAR acuity increases at PSTI eyes to 0.916± 0.25 and at control eyes to 1.168±0.17, the observed difference is statistically significant (P<0.001). Separate within-group analysis showed significant reduction in mean LogMAR acuity from baseline in the PSTI group throughout the study period visits. In the control group, a significant increase in mean LogMAR acuity from baseline was noted from the 2nd month till the 6th month of the observational period (table 2). Clinical examination after one week of PSTI revealed a decrease in macular edema and disappearance of cyst-like spaces in 88% of injected eyes. After three weeks the cyst-like spaces disappeared in all injected eyes. Recurrence of CME was noted in nine eyes (22%) of PSTI group at a mean time of 5.25±0.71 month. These eyes underwent reinjection and were observed for two months. The mean LogMAR acuity for this group was 1.275±0.15 and after two months of reinjection it decreases to 0.82±0.10. The difference was statistically significant (p<0.001). Figure 1 illustrates the changes in fluorescien angiography (FA) images of a representative patient in the PSTI group.
Table I. Baseline characteristics of studied patients
|
Variable
|
PSTI* group
|
Control group
|
|
Eyes No.
|
41
|
38
|
|
Mean age
|
61.16± 5.96
|
59.58±5.19
|
|
Gender (male/female)
|
23/18
|
20/18
|
|
Right/left
|
19/22
|
17/21
|
|
Status of DR No. (%)
Moderate NPDR
Severe NPDR
|
16 (39%)
25 (61%)
|
16 (42%)
22 (58%)
|
|
Mean HbA1c†
|
6.85±0.81
|
6.94±0.77
|
*PSTI, posterior subtenon injection; DR, diabetic
retinopathy; NPDR, nonproliferative diabetic retinopathy.
†HbA1c: glycosylated hemoglobin
Table II.
Mean visual acuity (Log MAR) by study visit
|
Visit time
|
PSTI* group
|
Control group
|
Between two groups
P value
|
|
Mean±SD
|
P value
|
Mean±SD
|
P value
|
|
Baseline
|
1.054± 0.19
|
|
1.038±0.16
|
|
>0.1
|
|
Week 1
|
0.680±0.13
|
0.001
|
1.039±0.16
|
0.328
|
<0.001
|
|
Week 3
|
0.588±0.13
|
0.001
|
1.044±0.16
|
0.183
|
<0.001
|
|
Week 6
|
0.528±0.12
|
0.001
|
1.048±0.16
|
0.097
|
<0.001
|
|
Week 8
|
0.505±0.13
|
0.001
|
1.064±0.16
|
0.018
|
<0.001
|
|
Week 12
|
0.612±0.13
|
0.001
|
1.069±0.16
|
0.009
|
<0.001
|
|
Week 16
|
0.696±0.15
|
0.001
|
1.106±0.16
|
0.001
|
<0.001
|
|
Week 20
|
0.787±0.19
|
0.001
|
1.147±0.17
|
0.001
|
<0.001
|
|
Week 24
|
0.916± 0.25
|
0.001
|
1.168±0.17
|
0.001
|
<0.001
|
*PSTI: posterior subtenon injection group
Baseline image (A) shows
fluorescien dye leakage in the foveal area with accumulation of the dye in the
cystic spaces around the foveola. At six months after injection (B) a mild
reduction in fluorescein dye accumulation is noted.
Two eyes (4.9%) of PSTI group developed a significant rise in IOP from
the baseline (mean 35mmHg) at the first week post-injection. Antiglaucoma drugs
were used to lower IOP of these two eyes for a mean time of 5.5 months. Figure
3 show insignificant rise of mean IOP (14.38± 1.72 to15.45± 5.37, P>0.05) at
the first week post-injection in PSTI
group. The difference between the two groups at this time point and subsequent
time points was not statistically significant. Another two (4.9%) had localized
subconjunctival hemorrhage at the site of injection. During the study
observation period we did not notice change in lens status or cataract
progression.
Discussion
This study demonstrates that
PSTI has a beneficial effect in reducing diabetic CME. On clinical examination
and after the first week of PSTI, 88% of the injected eyes show decrease in
macular edema with loss of cyst-like foveal formations. At the same time a significant increase in mean
visual acuity
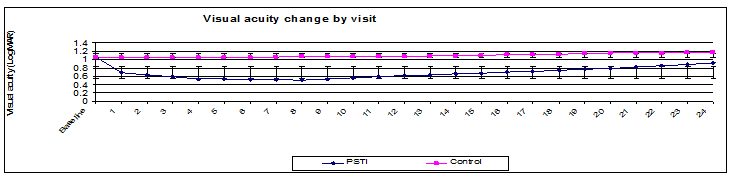
Fig. 1.
Dynamics of mean visual acuity in the PSTI and control eyes throughout the
study period
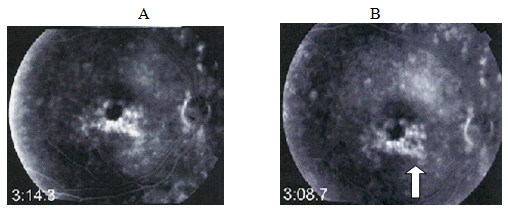

Fig. 2. Fluorescein
angiogram of right eye, before injection (A) the LogMAR acuity 1.0 and 6 months
after injection the LogMAR acuity 0.9. There is a mild reduction of dye leakage
after 6 months of injection (arrow)
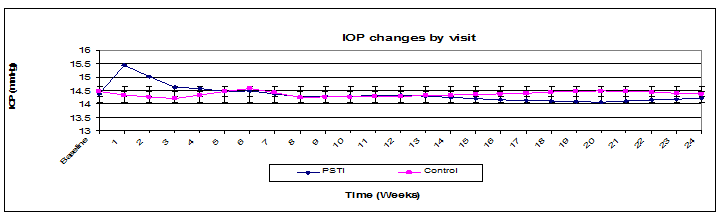
Fig. 3. Mean intraocular pressure in the PSTI and control
eyes throughout the study period.
from the baseline measurement was noted. Between
groups, analysis reveals a statistically significant difference in mean logMAR
visual acuity from the first week of observation. At the end of the second
month of observation the difference reached a plateau-like maximum. During the
next four months a gradual decrease in visual acuity of PSTI group was noted
and this could be related to steroid effect withdrawal. Accordingly, at week 24
(end of observation), the difference in LogMAR acuity between the two groups diminished,
but it was still significant (p<0.001). The recovered positive functional
and anatomical responses after PSTI were obtained by other researchers in the
treatment of diffuse diabetic macular edema.(18,19) Recurrence
of CME was noted in 22% of injected cases at a mean time of 5.25±0.71.
Reinjection of these eyes was associated with significant improvement in visual
acuity for the next two months.
Nussenblat(20) reported that
in cases of CME there was no significant relationship between the estimation of
visual acuity and the amount of fluorescein staining in the posterior pole. In
agreement with that report we noticed in our series that the changes in
fluorescein angiography were mild but functionally the vision was much better.
Cellini et al.(21)
used the inferior-temporal approach technique to inject the steroid. In our
study we found it easier to do the injection through a superior-temporal approach
as Young et al(13) performed, but without having to
create a surgical opening in the conjunctiva to access the subtenon. This
technique prevents reflux of TA after infusion, simplifies the procedure that
it could be performed in outpatient clinics and improves patient’s compliance
with this therapy.
Marco(17)
reported a significant rise in IOP from the baseline measurements in eyes with
diffuse diabetic macular edema after four weeks of PSTI. In our study, a significant
rise in IOP from the baseline was noted in two eyes after the first week of
PSTI. These eyes were treated with antiglaucoma drugs for a short time period
(5.5 month).
Other
possible complications of posterior subtenon corticosteroid injection include
ptosis, cataract formation, inadvertent globe perforation.(15)
Conclusion
PSTI of 40mg TA through a
superotemporal approach appears to be safe and effective for short-term
management of diabetic CME.
References
1.
Moss SE, Klein R, Klein BEK. The incidence of visual loss in a diabetic population.
Ophthalmology 1988; 95: 1340-8.
2. MacMeel
JW, Trempe CL, Franks EB. Diabetic
Maculopathy. Trans Am Acad Ophthalmol Otolaryngol 1977; 83: 476-87.
3. Quinn
CJ. Cystoid macular edema. Optom
Clin 1996; 5(1):111-30.
4.
Karacorlu M, Ozdemir H, Karacorlu S, et al. Intravitreal triamcinolone as a primary therapy in
diabetic macular oedema. Eye.
2005; 19:382–386.
5.
Massin P, Audren F, Haouchine B, et al. Intravitreal triamcinolone acetonide for diabetic
diffuse macular edema: preliminary results of a prospective controlled trial. Ophthalmology 2004; 111:218–224.
6.
Jonas
JB, Akkoyun I, Kreissig I, et al. Diffuse diabetic macular oedema treated by
intravitreal triamcinolone acetonide: a comparative, non-randomized study. Br J Ophthalmol 2005; 89:321-6.
7. Jonas
JB, Degenring RF, Kreissig I, et al. Intraocular pressure elevation after intravitreal
triamcinolone acetonide injection. Ophthalmology 2005; 112:593-8.
8.
Park
HY, Yi K, Kim HK. Intraocular
pressure elevation after intravitreal triamcinolone acetonide injection. Korean J Ophthalmol 2005; 19:122-7.
9. Moshfeghi
DM, Kaiser PK,
Scott IU, et al. Acute endophthalmitis
following intravitreal triamcinolone acetonide injection. Am J Ophthalmol 2003;
136:791-96.
10. Ohguro N, Okada AA, Tano Y. Trans-Tenon’s retrobulbar triamcinolone infusion for
diffuse macular edema. Graefes Arch Clin
Exp Ophthalmol 2004; 242:444–445.
11. Cardillo
JA, Melo LA Jr, Costa RA, et al. Comparison of intravitreal versus
posterior sub-Tenon's capsule injection of triamcinolone acetonide for diffuse
diabetic macular edema. Ophthalmology 2005 Sep; 112(9):1557-63.
12. Geroski DH, Edelhauser HF. Transscleral drug delivery for posterior segment
disease. Adv Drug Deliv Rev 2001; 52:37–48. doi: 10.1016/S0169-409X(01)00193-4.
13.
Choi
YJ, Oh IK, Oh JR, Huh K. Intravitreal versus posterior subtenon injection of triamcinalone
acetonide for diabetic macular edema. Korean J Ophthalmol 2006 Dec;
20(4):205-9.
14. Thomas ER, Wang J, Ege E, et al. Intravitreal triamcinolone acetonide concentration
after subtenon injection. Am J Ophthalmol 2006 Nov; 142(5):860-1.
15.
Bakri SJ, Kaiser PK.
Posterior subtenon triamcinolone acetonide for refractory diabetic macular
edema. Am J Ophthalmol
2005;139:290–294
16. Entezari
M, Ahmadieh H, Dehghan MH, et al. Posterior sub-tenon triamcinolone for refractory diabetic macular
edema: a randomized clinical trial. Eur J Ophthalmol
2005 Nov-Dec; 15(6):746-50.
17. Bonini-Filho
MA, Jorge R, Barbosa JC, et al. Intravitreal injection versus
sub-tenon’s infusion of triamcinolone acetonide for refractory diabetic macular
edema: A randomized clinical trial. Investigative Ophthalmology and
Visual Science 2005;
46:3845-3849
18. Toda J, Fukushima H, Kato S. Injection of triamcinalone acetonide into the posterior sub-tenon capsule for treatment of diabetic macular edema. Retina 2007 Jul-Aug; 27(6):764-9.
19. Wada M, Ogata N, Minamino K, et al. Trans-Tenon’s retrobulbar injection of triamcinalone acetonide for diffuse diabetic macular edema. Jpn J Ophthalmol 2005 Nov-Dec; 49(6):509-15.
20. Nussenblatt RB, Kaufman SC,
Palestine AG, et al. Macular thickening and visual acuity measurement in
patients with cystoid macular edema. Ophthalmology
1987 Sep; 94(9):1134-9.
21. Cellini
M, Pazzaglia A, Zamparini E, et al. Intravitreal vs. subtenon triamcinolone acetonide for the treatment of
diabetic cystoid macular edema. Ophthalmol
2008; 8: 1-7.