Abstract
Objective: The aim of
this study was to record the incidence of endodontic treatment that had to be
done for vital abutment teeth during tooth preparation or immediately after the
completion of the prosthetic treatment.
Methods: The study group consisted of all patients who received
prosthodontic treatment at King
Hussein Medical
Center from December 2003
to May 2007. All the members of the study group received metal-ceramic restorations
with at least one of the abutment teeth that had not received any form of root
canal treatment prior to the construction of the restoration. The abutment
teeth were evaluated clinically and radiographically before preparation. The
teeth were prepared using rotary cutting instruments with air and water spray
coolant. Until the cementation of the final restorations, the prepared teeth
were covered with temporary restorations. Any case of pulp exposure or pulpitis
during preparation or immediately after cementation of the final restoration or
within one week after cementation was recorded.
Results: A total of 264 patients (101 female and 163 male) received
290 fixed partial dentures during the study period. The mean age of the
patients was 40 years ranging from 18 to 73 years. For the 290 fixed partial dentures, there were
616 abutments and 415 pontics with an abutment/pontic ratio of 1.48: 1. Five
hundred and seventy one of the abutment teeth (92.7%) were vital at the
time of preparation and 45 teeth (7.3%) were endodontically treated. Thirty-four
(6%) of the vital abutment teeth subsequently required endodontic treatment.
Conclusion: In this
study 6% of the vital abutment teeth required endodontic treatment during or
immediately after cementation of the fixed partial dentures. The mandibular
molars, maxillary molars and mandibular anteriors respectively (6.9%, 6.7%,
6.7%) were the most common teeth to develop symptoms of endodontic
complications
Key words: Abutment
teeth, Endodontic complications, Fixed partial dentures
JRMS
June 2010; 17(2): 36-41
Introduction
A fundamental principle in
replacing missing tooth structure or missing teeth is the restoration of
function and esthetics at minimal biological cost.(1)
Given their reliability and
durability, conventional complete-crown coverage preparations generally are the
treatment of choice.(2) But despite the emphasis on
conservative preparation methods and restorative procedures, undeniable threats
to pulpal integrity exist during the construction of fixed prosthetic
restorations.(3)
The literature demonstrated
that each step in the fabrication of a fixed prostheses is a source of
potential insult to the pulp.(4-6) Before being
prepared to receive fixed restorations some teeth are subjected to pin
placement, cement bases and amalgam or composite restorative materials. Tooth
build up materials can be irritating to the pulp.(5)
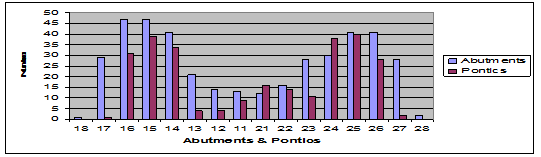
Fig. 1. Distribution of abutments and pontics of the
metal-ceramic fixed partial dentures (FPD) in the upper jaw
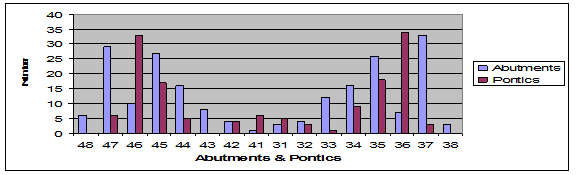
Fig. 2. Distribution
of abutments and pontics of the metal-ceramic FPDs in the lower jaw
Preparation of the tooth involves cutting dentin and
odontoblastic processes during which the pulp can be subjected to desiccation.(5)
Heat is also generated during tooth preparation.(5)
Impression techniques in current use necessitate drying the surface of the cut
dentin which may also desiccate dentine.(5) Polymerisation of resin materials used
for the fabrication of provisional restorations is associated with an
exothermic reaction.(4) This temperature rise may
present serious biological problem since it can cause iatrogenic thermal trauma
to the pulp.(7) Temporary and permanent restorations are held
in place with cements that may also irritate the pulp. Throughout the entire
process, bacteria are present from saliva and caries.(3)
Endodontic
complications have been observed in long term follow up studies.(8)
However, endodontic complications can occur during the preparation or shortly
after that and thus the clinical skills of the dentist are important. Therefore
the aim of this study was to record the incidence of endodontic treatment that
had to be done for vital abutment teeth during preparation or immediately after
the completion of the prosthetic treatment because of symptoms of acute
pulpitis or pulp exposure during preparation.
Methods
The study group consisted of
all the patients who received fixed prosthodontic treatment (Fixed Partial Dentures,
FPDs) at the fixed prosthodontic clinic at King Hussein
Medical Center
from December 2003 to May 2007. Data regarding gender and age were collected.
All the members of the study
group received metal-ceramic fixed partial dentures. The patients were selected
on the basis of having at least one vital abutment tooth that had not received
any root canal treatment before the construction of the restoration. A total of
290 FPDs fulfilled the inclusion criteria and were included in the study.
All the patients were evaluated
with a series of specific clinical procedures. The abutments were routinely
evaluated with preoperative periapical radiographs prior to tooth preparation.
Pre existing restorations were routinely removed and replaced before definitive
abutment preparation. Any tooth that was found to be non vital or with direct
pulp capping or with very deep caries was referred for endodontic treatment.
The teeth were prepared
using rotary cutting instruments (Diamond burs, Dentsply) with air and water
spray coolant in a high speed hand piece. One of the goals of tooth preparation
was to maintain maximum conservation of tooth tissue. All teeth were prepared
by the same dentist.
The prepared teeth were
temporized during the period between the preparation and the cementation of the
final restoration.
Table I. The
distribution of the abutments and pontics in the upper and the lower jaw
|
Teeth
|
Left side
|
Right side
|
|
Abutments
|
Pontics
|
Abutments
|
Pontics
|
|
Maxillary Central Incisors
|
12
|
16
|
13
|
9
|
|
Maxillary Lateral Incisors
|
16
|
14
|
14
|
4
|
|
Maxillary
Canine
|
28
|
11
|
21
|
4
|
|
Maxillary 1st Premolars
|
30
|
38
|
41
|
34
|
|
Maxillary 2nd Premolars
|
41
|
40
|
47
|
39
|
|
Maxillary 1st Molars
|
41
|
28
|
47
|
31
|
|
Maxillary 2nd Molars
|
28
|
2
|
29
|
1
|
|
Maxillary 3rd Molars
|
2
|
-
|
1
|
-
|
|
Mandibular Central Incisors
|
3
|
5
|
1
|
6
|
|
Mandibular Lateral Incisors
|
4
|
3
|
4
|
4
|
|
Mandibular Canines
|
12
|
1
|
8
|
-
|
|
Mandibular 1st Premolars
|
16
|
9
|
16
|
5
|
|
Mandibular 2nd Premolars
|
26
|
18
|
27
|
17
|
|
Mandibular 1st Molars
|
7
|
34
|
10
|
33
|
|
Mandibular 2nd Molars
|
33
|
3
|
29
|
6
|
|
Mandibular 3rd Molars
|
3
|
-
|
6
|
-
|
The temporary restorations
were constructed from poly methyl methacrylate (Temporyl, Dentra AG, Switzerland)
using the direct technique. The material was mixed according to the
manufacturer's instructions and poured in a polyvinyl siloxane molds (Elite HD,
Zhermach) and applied to the prepared teeth. Repeated removal and replacement
of the mold on the prepared teeth and air and water spray was used to minimize
heat increase during polymerization. The temporary restorations were cemented
using zinc oxide cement (Relay X Temp NE, 3M ESPE). The impression was taken by
polyvinyl siloxane impression material (Elite HD, Zhermach). The metal
frameworks of the fixed prostheses were casted in Nickel-Chromium alloy (Wiron
99, Wilhelm-Herbst-stra Be1, Germany).
For the final cementation, poly
carboxylate cement (Poly-F® Plus, Dentsply Detrey GmbH, Germany)
was used. The cement was mixed according to the manufacturers' instructions.
The abutment teeth were cleaned, isolated with cotton rolls and air dried, the
retainers were seated with finger pressure.
The pulpal status of the
prepared teeth relied on clinical symptomatology. In case of pulpitis (during
preparation or immediately after cementation of the final restoration or within
one week after cementation) the cases were recorded and referred for endodontic
treatment. In addition, all the abutments that suffered pulp exposure during
preparation were recorded and referred for endodontic treatment.
Results
A total of 264 patients (101
female and 163 male) were treated at the fixed prosthodontic clinic at King
Hussein Medical Center (KHMC) from December 2003 till May 2007. The mean age of
the patients was 40 years ranging from 18 to 73 years.
The patients received 290
FPD. All the prostheses were metal-ceramic restorations. For the 290 FPD there
were 616 abutments and 415 pontics with an abutment/pontic ratio of 1.48:1. The
distribution of the abutments and pontics in the upper and lower jaws is shown
in Table I and presented graphically in Fig. 1 and Fig. 2.
The anterior FPDs accounted for 12.1% (35 prostheses)
and the posterior FPDs accounted for 82.4% (239 prostheses) and 18 prostheses
(5.5%) were extending between anterior and posterior teeth.
From the 616 abutment teeth,
571 teeth (92.7%) were vital at the time of preparation and 45 teeth (7.3%)
were endodontically treated. Six percent of the vital abutment teeth (34 teeth)
subsequently required endodontic treatment either due to pulp exposure (4
teeth, 0.7%) or due to development of symptoms of acute pulpitis (30 teeth,
5.3%). Table II shows the frequency of tooth types and the number of teeth
required endodontic treatment. 6.9 % of the prepared mandibular molar abutment
teeth required endodontic treatment. The maxillary anterior teeth were the
least teeth that required endodontic treatment, 4.1% of the prepared maxillary
anterior teeth developed symptoms of acute pulpitis. The span length of the FPD prostheses is recorded in Table III. Three unit FPDs were the most common (163 prostheses) and accounted for 56.2% of all prostheses.
Table II: Frequency
of tooth types and the number of teeth required endodontic treatment.
|
Tooth type
|
No. of abutment teeth
|
No. of abutment teeth
that needed endodontic treatment due to
|
%
|
|
|
|
Pulpitis
|
Pulp exposure
|
|
|
Maxillary Anteriors
|
97
|
4
|
-
|
4.1
|
|
Maxillary Premolars
|
140
|
6
|
3
|
6.4
|
|
Maxillary Molars
|
135
|
8
|
1
|
6.7
|
|
Mandibular Anteriors
|
30
|
2
|
-
|
6.7
|
|
Mandibular Premolars
|
83
|
4
|
-
|
4.8
|
|
Mandibular Molars
|
86
|
6
|
-
|
6.9
|
|
Total
|
571
|
34
|
34
|
|
Table III: The
span length of the FPD prostheses
|
No. of units
|
No. of FPD prostheses
|
%
|
|
2 units FPD(cantilever)
|
18
|
6.2
|
|
3 units FPD
|
163
|
56.2
|
|
4 units FPD
|
76
|
26.2
|
|
5 units FPD
|
21
|
7.2
|
|
6 units FPD
|
10
|
3.4
|
|
7 units FPD
|
-
|
-
|
|
8 units FPD
|
1
|
0.4
|
|
9 units FPD
|
-
|
-
|
|
10 units FPD
|
1
|
0.4
|
|
Total
|
290
|
100
|
Discussion
In this study the endodontic
complications during the preparation phase or immediately after the completion
of the metal ceramic FPD (early or primary endodontic failures) were evaluated.
The literature revealed that 3-38% of teeth prepared for complete coverage
undergo pulpal necrosis.(8-11) But there is no clear picture
of the risk involved for pulpal breakdown in teeth subjected to fixed
prosthodontic therapy.
The incidence of early
pulpal deterioration in the present study was relatively low (6%) in consistence
with the results of Jackson et al.
who found that 5.7% of teeth crowned in a vital condition suffered irreversible
pulpal involvement.(3) Chenug et al. found that 33% of
vital abutment teeth developed signs of endodontic complications some time after
the cementation of the final restorations during a follow up period up to 15
years.(12) Table II shows that the mandibular molars, maxillary
molars and mandibular anteriors respectively (6.9%, 6.7%, 6.7%) were the most
common teeth to develop symptoms of endodontic complications. Cheung et al.
found that the upper maxillary anterior teeth are the most common to develop
endodontic complications (54.5%).(12) During teeth
preparation four teeth suffered pulpal exposure (3 maxillary premolars and 1
maxillary molar). The demand for necessary parallelism of the abutment teeth in
FPD sometimes can be difficult to perform and complications of this kind are
predictable. In this study most of the FPDs were constructed in the upper jaw
as has been noted in earlier studies by Meeuwissen and Eschen and Raustia et
al.(9,13) The most common used abutments in the maxilla
were the second premolars and first molars while in the mandible the most
common used abutments were the second premolars and the second molars. Meeuwissen
and Eschen found the upper left canine is the most frequently used abutment in
the maxilla while in the mandible it was the second left premolar.(9)
Raustia et al. found that the most usual abutments teeth were the
canines in the maxilla and molars in the mandible.(13) Wisdom
teeth were rarely used as abutments.
Maintenance of the vitality
of the dentinal substrate and minimization of pulpal damage are perhaps the
most important aspects of tooth preparation.(14) The response
of the pulp to restorative procedures is cumulative, each procedure adds to the
response engendered by the previous.(15) Several essential
procedures may contribute to pulpal damage during the construction of fixed
prostheses. These procedures include excessive tooth reduction, heat, desiccation,
pressure applied during tooth reduction, chemical injury, bacterial infection.(4-6)
Conventional metal- ceramic restorations require considerable reduction of
tooth structure.(16) A minimal reduction of 1.5mm is
routinely indicated for acceptable esthetic and function.(6)
Multiple important clinical criteria controlled the preparation design. Theses
criteria include the condition of the tooth, esthetic and functional aspects,
orientation of the tooth and retention.(1) Stanley and Swerdlow showed from histological studies that specimens
with dentine thickness greater than 2mm after preparation demonstrated little
or no pulpal response.(17) Therefore the use of minimal
preparation design may result in conservation of sound tooth structure and maintenance
of tooth vitality.(1,14) During tooth preparation
cooling is necessary to minimize heat generation. Lockard found that air alone
or air and water spray can be used successfully as coolant.(18)
Schuchard and Watkins stated that the low conductivity of dentin and
circulation in the pulp can dissipate the heat conducted to the pulp.(19)
Susuki et al. also reported that the use of high speed crown preparation
accompanied by water spray will not cause any disruption of the odontoblastic
layer.(14)
Temporary coverage of prepared teeth often
involves the use of self curing resin materials. Auto polymerising PMMA resin
in contact with dentine during polymerisation can cause injury to the pulp as a
result of the free monomer and the heat of the exothermic reaction.(4,7)
Michalakis et al. founded that the intra pulpal temperature increase
resulting from the polymerisation process of the provisional restorations can
reach up to 4.5ºC.(7) According to Zach and Cohen the intra
pulpal changes resulting from temperature increase during polymerisation ranged
from minimal to significant but the majority of the pulp tissue in their study
recovered.(20) Therefore these materials must be cooled
during polymerising.
The prepared teeth should
not be excessively dried, dentine is moist and it should remain moist during
all procedures.(4) Brännström reported that desiccation
of vital human dentine with air chip syringe causes aspiration of odontoblasts
and their nuclei.(21) Therefore removal of surface moisture
from prepared vital dentin must be carried out gently with air syringe used for
only short time periods.
It was reported that luting
cements are not irritating to the pulp.(21) In this study poly
carboxylate cement was used for the permanent cementation of the final restorations.
Poly carboxylate cement has a relatively long history as luting cement and it
has a reasonable track record.(22)
During the last years it has
been shown in numerous experiments that infection is the main cause of pulpal
damage under restorations.(23) Therefore the key for pulpal
recovery from preparation trauma is the prevention of leakage of bacteria and
bacterial by product. Prevention of bacterial leakage may be the reason for
successful use of temporary luting agents containing zinc oxide-eugenol.(24)
The low rate of pulpal
involvement in this study shows that the proper techniques that were used
during the construction of the FPDs caused little or no permanent injury to the
pulpal tissue. The techniques included comprehensive assessment of the pulpal
health before the restorative treatment. In addition, the conservative tooth
preparation with the proper air-water coolant, the proper consideration of the
cut dentine during impression taking, the fabrication of the provisional restorations
and sealing the provisional and the final restorations against bacterial
invasion appear to be important factors in maintaining pulpal vitality and
minimizing pulpal damage. If meticulous care is not taken, pulpal damage or
death can occur. Patients should be
warned that pulpal death and endodontic therapy can result from the
construction of fixed restorations.
Direct measurement of pulp
vitality in the clinic is only possible if irreversible test methods like
histological examinations are used. Therefore, pulp vitality is usually
diagnosed based on the patient anamnestic data and the evaluation of tooth
response to thermal or physiological stimulation. In this study, the diagnosis
of pulpal inflammation was based on the patients presenting history, clinical signs
and symptoms. It was possible that pulpal necrosis could have developed but
remained undetected in the present study due to absent clinical symptoms.
Although many histological studies have documented pulp and dentine reaction
after prosthodontic therapy, the incidence and the risk period of pulp deterioration
remain uncertain.(11) Therefore; more teeth may loose their
vitality with time. Follow up study with
longer time period is recommended to detect these failures.
The present study design is
not experimental, which limits the possibility to determine any cause-effect relationship
between the observed defects on the abutment teeth and the different clinical
variables. Therefore, it is difficult to determine which clinical factor or
material is the most effective means of preventing or causing pulpal
inflammation.
Conclusion
Six percent of the vital abutment
teeth subsequently required endodontic treatment during preparation or
immediately after the cementation of the final restorations. The mandibular
molars, maxillary molars and mandibular anteriors respectively (6.9%, 6.7%,
6.7%) were the most common teeth to develop endodontic complications.
References
1. Edelhoff
D, Sorensene JA. Tooth structure
removal associated with various preparation designs. J Prosthet Dent
2002; 87:503-509.
2. Creuger
NH, Kayser AF, van't Hof MA. A meta-analysis of durability data on conventional fixed bridges. Community
Dent Oral Epidemiology 1994;22:448-452.
3.
Jackson CR, Skidmore A.E, Ted Rice R. Pulpal evaluation of teeth restored with fixed
prostheses. J Prosthet Dent 1992; 67:323-325.
4.
Christensen
G J. Tooth preparation and
pulp degeneration. JADA 1997; 128:353-354.
5. Christensen
G J. Avoiding pulpal death
during fixed prosthodontic procedures. JADA 2002; 133:1563-1564.
6.
Christensen
G J. How to kill a tooth. JADA 2005;
136:1711-173.
7. Michalakis
K, Pissiotis A, Hirayama H, Kang K, Kafantaris N. Comparison of temperature increase in pulp chamber
during the polymerisation of materials used for the direct fabrication of
provisional restorations. J Prosthet Dent 2006; 96: 418-423
8.
Goodacre
Ch J, Bernal G, Rungcharassaeng K. Clinical complications in fixed prosthodontics. J Prosthet Dent
2003; 90:31-41.
9.
Meeuwissen
R, Eschen S. Prosthodontic
treatment and retreatment of 845 servicemen. J Prosthet Dent 1985;
53:425-427.
10. Jokstad A, Mjör A. Ten year clinical evaluation of three luting cements.
J Dent 1996; 24: 309-315.
11. Valderhaug A, Jokstad A, Ambjørnsen
E, Norheim PW. Assessment of the periapical and
clinical status of crowned teeth over 25 years. J Dent 1997; 25: 97-105.
12. Cheung GSP, Lai SCN, Ng RPY. Fate of vital pulps beneath a metal-ceramic crown or
a bridge retainer. Int Endo J 2005; 38: 521-530.
13. Raustia AM, Napankangas R, Salonen MAM. Complication and primary failures related to fixed
metal ceramic bridge prostheses made by dental students. J Oral
Rehabil 1998; 25: 677-680.
14. Suzuki Sh, Cox CF, White KC. Pulpal response after complete crown preparation,
dentinal sealing, and provisional restoration. Quintessence Int 1994;
25; 477- 485.
15. Collett HA. Protection of dental pulp in construction of fixed
partial denture prostheses. J
Prosthet Dent 1974; 31:637-645.
16. Shillinburg, Jr HT, Hobo S, Whitsett
LD, Jacobi R, Brackett SE.
Fundamentals of Fixed Prosthodontics. 3rd edition. Quintessence
publication Co, Inc. 1997; 139-154.
17. Stanley HR, Swerdlow H. Reaction
of the human pulp to cavity preparation: results produced by eight different
operative grinding techniques. JADA 1959; 58: 49-59.
18. Lockard MW. A retrospective study of pulpal response in vital
adult teeth prepared for complete coverage restorations at ultrahigh speed
using only air coolant. J Prosthet Dent 2002; 88: 473-478.
19. Schuchard A, Watkins C. Temperature response to increased rotational speed. J
Prosthet Dent 1961; 11: 313-317.
20. Zach L, Cohen G. Pulp response to externally applied heat. Oral Surg
Oral Med Oral Pathol 1965; 19: 515-530.
21. Brännström M. Reducing the risk of sensitivity and pulpal
complications after placement of crowns and fixed partial dentures. Quintessence
Int 1996; 27: 673-678.
22. Wassell RW, Barker D, Steele JG. Crowns and extra-coronal restorations: Try-in and
cementation of crowns. BDJ 2002; 193: 17-28.
23. Brännström M. Class II resin composite restorations: Reducing
sensitivity, pulpal damage, and secondary caries. Esthet Dent Update
1994; 5: 86-90.
24. Brännström M. Nordenvall K,
Torstenson B. Pulpal reaction
to IRM cement: An intermediate restorative material containing eugenol. J
Dent Child 1981; 48: 259-263.