ABSTRACT
Objective: To describe the functional independent recovery and to assess
compliance effect to rehabilitation therapy among acute stroke patients at King Hussein
Medical Center.
Methods: A total of 100 first time acute stroke (87
ischemic, 13 hemorrhagic) patients aged 60-70 years, who were
admitted to King Hussein Medical Centre between June 2006 and June 2007 with
acute stroke and at the same time were eligible for rehabilitative care were
included in this descriptive study. Data was collected using a specially
designed medical abstract form for demographic characteristics, risk factors,
functional independent recovery measure, follow-up for six months, and
compliance to rehabilitation therapy. Simple descriptive statistics were used
to analyze the data.
Results: The results were classified into three groups. Group I: patients who
were independent within the first 72 hours (12%). Group II: patients who were
independent after six months (53%). Group III: patients who were dependent with
variable degrees (28%). Four percent of
the patients died during the 6-month follow-up period, and 3% were lost to follow-up.
Compliance to rehabilitation therapy was highest among group II (84.9%) however
the lowest compliance percentage to rehabilitation therapy was among group III
(17.9%). The major causes of non-compliance to rehabilitation were financial, transportation
difficulties, and family misconception of the irreversibility of this disease
respectively.
Conclusion: A general health
care policy is needed in order to improve the compliance of stroke patients to
rehabilitation therapy.
Key words: Functional
independent measures, Stroke, Rehabilitation outcome
JRMS
June 2010; 17(2): 42-46
Introduction
Stroke is one of the leading causes of
disability(1) and the social and economic burden
of stroke is expected to expand. Despite some advances
in acute stroke intervention such as tissue plasminogen activator,
which had no large impact on stroke-related disability, primarily because this
treatment can be offered to only a minority of ischemic stroke survivors.(2) Greater levels of adherence to post acute stroke
rehabilitation have been associated with improved patient outcomes.(3,4) There is evidence from European studies,
indicating that stroke rehabilitation
programs in the post acute period reduce death or dependency.(5,6)
The Rehabilitation
Service at King Hussein Medical Center (KHMC) follows the most
recent clinical guides for best stroke rehabilitation
care.
This situation provides the opportunity
to assess the relationship between processes of stroke rehabilitation care and outcomes. We hypothesized that patients who received the best quality of care as measured by compliance with the stroke rehabilitation guidelines would have better functional outcomes. The purpose of this study was to describe the functional independent recovery and to assess compliance effect to rehabilitation therapy among acute stroke patients at King Hussein Medical Center.
Table I. The
functional independent recovery measure (FIM)
|
|
Admission
|
Discharge
|
Follow-Up
(6-Months)
|
|
Self-Care
|
|
|
|
|
A. Eating
|
|
|
|
|
B. Grooming
|
|
|
|
|
C. Bathing
|
|
|
|
|
D. Dressing-Upper body
|
|
|
|
|
E. Dressing-Lower body
|
|
|
|
|
F. Toileting
|
|
|
|
|
Sphinicter Control
|
|
|
|
|
G. Bladder Management
|
|
|
|
|
H. Bowel Management
|
|
|
|
|
Transfers
|
|
|
|
|
I. Bed, Chair, Wheelchair
|
|
|
|
|
J. Toilet
|
|
|
|
|
K. Tub, Shower
|
|
|
|
|
Locomotion
|
|
|
|
|
L. Walk/Wheelchair
|
|
|
|
|
M. Stairs
|
|
|
|
|
Motor Subtotal Score
|
|
|
|
|
Communication
|
|
|
|
|
N. Comprehension
|
|
|
|
|
O. Expression
|
|
|
|
|
Social Cognition
|
|
|
|
|
P. Social Interaction
|
|
|
|
|
Q. Problem Solving
|
|
|
|
|
R. Memory
|
|
|
|
|
Cognitive Subtotal Score
|
|
|
|
|
Total FIM score
|
|
|
|
N.B.
If the patient is not testable due to risk, a value of 1 is evaluated.
Methods
A total of 100 first time acute stroke
(87 ischemic, 13 hemorrhagic) patients aged 60-70 years who
were admitted to King Hussein Medical Centre between June 2006 and June 2007
with acute stroke and at the same time were eligible for rehabilitative care
were included in this descriptive study. Inpatient rehabilitation was performed
from admission day till discharge day, when outpatient rehabilitation commenced
for the following six months. Data was collected using a specially designed
medical abstract form for demographic characteristics, risk factors, functional
recovery independent recovery measure, follow-up for six months, and compliance
to rehabilitation therapy. Simple descriptive statistics in the form of means
and percentages were used to analyze the data.
During the study period, patients
considered candidates for rehabilitation were
screened by the treating physicians during their acute stroke
admission to confirm diagnosis of stroke
(defined as symptoms of rapid onset lasting more than 24 hours and
of presumed vascular origin reflecting a focal disturbance of
cerebral function, excluding isolated impairment of higher function).
The diagnosis was based on clinical assessment (side of hemi paresis, sensory loss, hemianopsia, dysphasia, dysphagia,
inattention,
impulsivity, or impaired problem solving) supported
by Computerized Tomography (CT) or Magnetic Resonance Imaging (MRI).
|
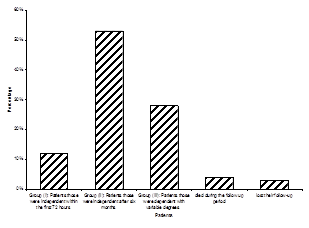
Fig. 1.
Stroke patient distribution during the study period
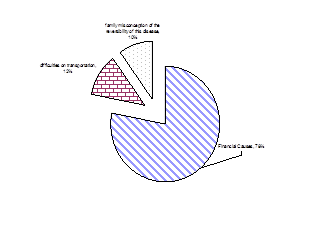
Fig. 2. Main causes of poor compliance to rehabilitation
|
|
|
Table II. Demographic and risk factors among the
study group
|
No.
of patients
|
100
|
|
Mean
Age
|
64 (SD±4)
|
|
Gender
|
|
|
Males
|
64
|
|
Females
|
36
|
|
Diabetes
mellitus
|
17
|
|
Hypertension
|
72
|
|
Smoking
|
67
|
|
Heart
disease
|
12
|
|
Our
primary outcome was the functional independent recovery at six months post stroke through physical examination of the patients. Functional
status was evaluated by means of the Functional Independence Measure (FIM). FIM scores as
shown in Table I was recorded by each patient’s treating therapists within 48
hours of admission and discharge. FIM is composed of six sections (self-care,
sphincter control, transfers, locomotion, communication, social cognition) with
a total of 18 items. The highest achievable score is seven for each item and
the maximum total score possible on the tool is 126. The higher the score, the
greater the functional independence is. An FIM value more than 110 was
considered completely independent in this study.
FIM scores can be represented in three different ways,
including a global score (full-scale), two domains (cognitive and motor), and six
subscales, including self-care, mobility, locomotion, sphincter, social cognition,
and communication. This study specifically used the six subscales scores.
Results
Out of the 100 acute stroke patients in
the current study, 93% of them were interviewed at six months post stroke
to obtain the study outcome measures. Demographic and risk factors
of the study group is presented in Table II.
The results were classified into three
groups as shown in Fig. 1. Group I patients were independent within the first
72 hours, and constituted 12% of the patients. Group II patients were
independent after six months, and constituted 53% of the patients. Group III
patients were dependent with variable degrees, and constituted 28% of the patients.
Four percent died during the follow up period, and 3% were lost to follow up.
Compliance to rehabilitation was studied among
patients during the physical examination and through interview with their
families. It was found that among group II, there were 45 patients (84.9%) who were
adherent to rehabilitation. On the other hand, among group III only five
patients (17.9%) were adherent to rehabilitation. The causes of poor compliance to
rehabilitation were studied. Fig. 2 shows the main causes of poor compliance with
rehabilitation.
Financial causes were the primary cause (78%)
and this was accompanied by lack of family caregivers. Difficulties in
transportation were the second most common cause (12%) mostly involving
patients who were living in a place more than 80 kilometers away from the
center with no direct transportation method available. Family misconceptions of
the irreversibility of the disease (10%) were the third most common cause of
poor compliance with rehabilitation.
Discussion
Despite this study’s limitation of its small
sample size, the percentages of patients observed in groups I and II were
comparable with other studies,(1,6) however a lower percentage rate of independent
recovery was demonstrated in the study conducted by Bagg and colleagues(2) for group III.
An evaluation of 11 published studies reporting
estimates of reliability for FIM scores reported acceptable reliability across
a wide variety of settings, raters, and patients, and an excellent level of
reliability has also been demonstrated. The FIM has good internal consistency
and better than average face validity.(2,7)
Stroke unit treatment reduced the relative
risk of death within five years after stroke.(8) In the United States, post stroke care in
hospitals was proved to be more efficient than rehabilitation in nursing homes.(9)
Therefore, the majority of stroke
survivors will need rehabilitation
services to enhance their recovery and to minimize disability.
In a previous study(3) the average
compliance scores in acute and post acute care settings were 68.2%
and 69.5%, respectively. After case-mix adjustment, level of
compliance with post acute rehabilitation guidelines was
significantly associated with FIM scores.(3)
Based on the results obtained in this study, a local health
care policy is suggested to be introduced. Previous studies(13)
have suggested recommendations such as the delivery of post stroke care in a
multidisciplinary rehabilitation setting or stroke unit, early patient
assessment via the NIH Stroke Scale, early initiation of rehabilitation therapies,
swallow screening testing for dysphagia, an active secondary stroke prevention
program, and proactive prevention of venous thrombi. Standardized assessment
tools should be used to develop a comprehensive treatment plan appropriate to
each patient’s deficits and needs. Medical therapy for depression or emotional
liability is strongly recommended. A speech and language pathologist should
evaluate communication and related cognitive disorders and provide treatment
when indicated. The patient, caregiver, and family are essential members of the
rehabilitation team and should be involved in all phases of the rehabilitation
process.(13)
Stroke is the third leading cause of death and a
leading cause of disability in the United States. Globally, it is the second
leading cause of death with about 5.7 million deaths world wide, equivalent to
9.9% of all deaths.(14) Therefore, follow up for stroke
patients should be done on a routine basis. This, to be successful, will
require special emphasis on the importance of rehabilitation to the family
caregivers, and offering transportation facilities for each patient.
Conclusion
The majority of the patients were
independent within the first six months. Compliance to rehabilitation showed
improvement among stroke patients. A general health care policy is needed in
order to improve the compliance of stroke patients to rehabilitation therapy.
Further analytical studies with larger
numbers of acute stroke patients are needed which consider the use of
multivariate analysis for risk factors including diabetes mellitus,
hypertension, smoking, and cardiovascular diseases.
References
1. Kasper DL, Branwald E. Cerbrovascular
diseases: Wade S. Smith, S. Claiborne Johnson, J. Donald Etson. Harrison’s principles of internal medicine. 16th
ed. Mc Graw Hill 2005; p. 2372-2393.
2. Bagg S, Pobmbo AP, Hopman
W. Effect of
age on functional outcomes after stroke rehabilitation. Stroke 2002;
33: 179-185.
3. Duncan PW, Horner RD, Reker DM, et al. Adherence to Postacute rehabilitation guidelines is associated
with functional recovery in stroke. Stroke 2002; 33; 167-178.
4. Bode RK, Heinemann
AW, Semik P, et al. Relative importance of
rehabilitation therapy characteristics on functional outcomes for persons with
stroke. Stroke 2004; 35: 2537-2542.
5. Wit LD, Putman K, Lincoln N, et al. Stroke rehabilitation in Europe:
what do physiotherapists and occupational therapists actually do?. Stroke
2006; 37:1483-1489.
6. Wit LD, Putman K, Dejaeger E, et
al. Use of time by stroke
patients: a comparison of four Europian rehabilitation centers. Stroke
2005; 36: 1977-1983.
7. Kelly PJ, Stein J, Shafqat S, et
al. Functional recovery
after rehabilitation for Cerebellar stroke. Stroke 2001; 32;
530-534.
8. Jorgensen HS, Kammersgaard LP,
Nakayama H, et al. Treatment
and rehabilitation on a stroke unit improves 5-year survival: A community-based
study. Stroke 1999; 30; 930-933.
9. Kramer AM, Steiner JF, et al. Outcomes and costs after hip fracture and stroke: a
comparison of rehabilitation settings. JAMA 1997; 277:396-404.
10. Jorgensen HS, Kammersgaard LS, Houth
J, et al. Who benefits
from treatment and rehabilitation in a stroke unit? A common-based study. Stroke 2000; 31; 434-439.
11. Anderson C, Rubenach S, Mhurchu CN, et
al. Home or hospital for
stroke rehabilitation? Results of a randomized controlled trial: Health outcomes
at 6months. Stroke 2000; 31; 1024-1031.
12. Grant JS, Elliott TR, Weaver M, et
al. Telephone intervention
with family caregivers of stroke survivors after rehabilitation, Stroke 2002;
33; 2060-2065.
13. Bates B, Choi JY, Duncan PW, et al. Veterans affairs/ department of defense clinical
practice guideline for the management of adult stroke rehabilitation care. Stroke 2005; 36: 2049–2056.
14. Jurkowski JM, Maniccia DM, Dennison
BA, et al. Awareness of
necessity to call 911 for stroke symptoms, Upstate New York. Preventing
Chronic Diseases 2008; 7: 1-14.