Abstract
Objective: To
evaluate the mid-term results of balloon pulmonary valvuloplasty in children.
Methods: One hundred and thirty-two patients with a median age
of three years (range 3 days to 16 years), underwent balloon pulmonary
valvuloplasty between January 2000 and January 2007 at the Pediatric Cardiology
Department of Queen Alia Heart Institute, Amman-Jordan. We evaluated our patients
with regard to clinical symptoms, peak to peak pressure gradient across the
right ventricular outflow tract before and after balloon pulmonary
valvuloplasty. Thereafter, we followed them at our outpatient clinic regarding clinical
symptoms, the peak instantaneous pressure gradient, the presence of pulmonary
valve incompetence, right ventricular function based on echocardiographic
findings, and the need for repeat balloon pulmonary valvuloplasty.
Results: There was significant reduction in the peak to
peak gradient from 93.5 ± 32.3 mmHg to 26.1 ± 9.6 mmHg (P<0.001). Repeat balloon
pulmonary valvuloplasty was performed in 12% of cases. Surgical intervention performed
for dysplastic valve and fixed subpulmonic obstruction was done in 11.36% of
cases. Echo-Doppler data showed that residual peak instantaneous gradient
dropped with time from 24.4±3 to 19 ± 6 mmHg (P<0.001) on follow up range (5
months to 5.2 years). Mild to moderate pulmonary valve regurgitation was noticed
in 34 patients (27.8%) at one year and in 43 patients (38%) at midterm follow
up, but none had right ventricular dilatation or paradoxical interventricular
septal motion.
Conclusions:
The results of midterm follow up after balloon dilatation of the pulmonary
valve is encouraging. Restenosis occurred in 22% of cases. Children under two
years had statistically significant higher pressure gradient and more pulmonary
regurgitation. The degree of pulmonary regurgitation increased with time.
Longer term follow up studies should be undertaken to evaluate the significance
of residual pulmonary regurgitation.
Key
words: Balloon dilatation, Pulmonary
stenosis, Pulmonary regurgitation
JRMS
June 2010; 17(2): 47-52
Introduction
Pulmonary stenosis accounts for about 10-12% of all
cases of congenital heart diseases.(1) Since 1982, after the
first description of balloon dilatation of pulmonary valve by Kan et al.(2-5)
balloon pulmonary valvuloplasty (BPV) has become the treatment of choice for
moderate to severe pulmonary valve stenosis (PS) with
intact ventricular septum in all ages, and completely replaced surgical
valvotomy. Several studies reported excellent acute and intermediate results,(1-15)
but still the long term results are to be clarified.
We conducted our study to show our intermediate
results and experience in balloon pulmonary valvuloplasty in children at Queen
Alia Heart Institute (QAHI) in Jordan,
although the first BPV performed successfully in this institute was in November
1988.
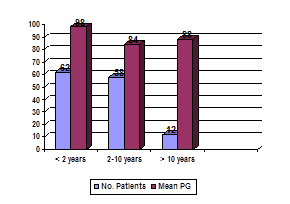
Fig.1.
Distribution of cases according to age
Fig. 2.
Right ventriculogram, in lateral projection showing thickening and doming of
the pulmonary valve with poststenotic dilatation
Fig. 3a.
The balloon catheter across the pulmonary valve is indented by the stenotic
valve
Fig. 3b.
The balloon catheter is fully inflated and the waist is abolished
ody
Fig. 4.
Right ventriculogram post balloon dilatation, the annulus of the pulmonary
valve is dilated, the blood flow is better and the right ventricle pressure
dropped
From
January 2000 to January 2007 at QAHI, 132 patients with a median age of three
years (range 1 day-16 years), and a median weight of 11 kg (range 3.5-51Kg) underwent
balloon pulmonary valvuloplasty. We
classified our cases according to age below two years, two to ten years and
those above ten years of age (Fig. 1). Fifty four cases were males (41%)
whereas 78 (59%) were females. They presented
with chief complaints of shortness of breath or exertional dyspnea, underwent
balloon dilatation of the pulmonary valve (BPV). Data were collected
retrospectively by reviewing their medical records, noninvasive studies and cardiac
angiograms to obtain acute and intermediate results. Inclusion criteria were those
patients with maximum instantaneous pressure gradient (PG) across the pulmonary
valve by Echo-Doppler was ≥ 50mmHg. Dysplastic pulmonary valve which was
defined as the presence of thick, immobile valve leaflets with the absence of
poststenotic pulmonary valve artery dilatation was noticed in 18 cases (13.6%).
Excluded cases were those with associated cardiac anomalies except those with
small hemodynamically insignificant secundum atrial septal defect which was
observed in 29 patients (22%) who were included. Two cases had Noonan syndrome.
Table I. Grading of pulmonary regurgitation by echo Doppler
studies
|
None
|
No
pulmonary regurgitation on Doppler study
|
|
Grade
I
|
Pulmonary
regurgitation jet width < 10% of pulmonary valve annulus
diameter in precordial short axis view
|
|
|
No
right ventricle volume overload
|
|
Grade
II
|
Pulmonary
regurgitation jet width 11-25% of pulmonary valve annulus diameter
|
|
|
No
right ventricle volume overload
|
|
Grade
III
|
Pulmonary
regurgitation jet width 26-50% of pulmonary valve annulus diameter
|
|
|
No
right ventricle volume overload but with or without flat septal motion
|
|
Grade
IV
|
Pulmonary
regurgitation jet width > 50% of pulmonary valve annulus
diameter
|
|
|
Right
ventricle volume overload present
|
Jet
width at the origin of regurgitation jet rather than jet length was used for
grading because the jet width is not influenced by pulmonary artery pressures.
Right ventricle volume overload is defined as enlarged
right ventricle (> 95 percentile) and flat to paradoxical septal
motion.
Informed consent was obtained from the parents of
each patient after fully describing the
technique
and the aim of the procedure.
After initial hemodynamic assessment right ventricular angiography was
performed, and maximum internal diameter of the pulmonary valve from hinge
point to hinge point during systole was measured from the lateral projection
cineangiogram and corrected for magnification. Our technique of balloon dilatation
of the pulmonary valve was similar to that described in details by others.(4,16-19)
(Fig. 2-4). The balloon size used was 1.2 to 1.4 times the size of the
measured pulmonary valve annulus on the lateral projection. We define the
success rate if peak to peak pressure gradient (PG) by pull back pressure
tracing post BPV was ≤ 35mmHg immediately after the procedure. All patients
were given heparin in a dose of 100 Units/Kg during the procedure. The patient
usually stayed in hospital for one day after the procedure, received
intravenous antibiotics and was discharged after performing 2D-Echo Doppler
evaluation.
Follow up evaluation as outpatient
included both clinical and 2D-Echo and Doppler examination at one, three and
six months and then yearly thereafter. The clinical evaluation focused on
clinical signs of stenosis. The 2D-Echo-Doppler evaluation assessed the maximum
instantaneous pressure gradient across the pulmonary valve, the presence of
pulmonary regurgitation (PR) if it was grade I, II, III or IV according to the
color jet width of regurgitant flow across the pulmonary valve as per RAO et
al.’s(4) (Table I) classification, which was performed in the
precordial short axis view and the right ventricular function as well and
finally the interventricular septal movement by the M-mode.
Statistical analysis:
All data were expressed as mean ± SD or median with
range. Paired t- test was used to compare the mean right ventricular
pressure and pressure gradient across the pulmonary valve before and after
balloon valvuloplasty. A P value less than 0.05 was considered significant.
Results
Immediately after the initial balloon
pulmonary valvuloplasty there was a
significant reduction in the peak to peak gradient from 93.5±32.3mmHg to
26.1±9.6mmHg (P value <0.001) (Fig. 5). There was also a significant
reduction in the right ventricular pressure (RVP) from 117.6±33.1mmHg to
50.7±9.9mmHg with a P value <0.001 (Fig. 6). Forty-five patients (34%) had re-stenosis and their
immediate peak to peak maximum PG post BPV was ≥ 35mmHg, making the early
success rate of 66%. Sixteen of them (12%) underwent repeat dilatation of the
pulmonary valve, in a mean period of 12±4months after the initial dilatation
with significant reduction of their peak to peak PG from 65±3.65 mmHg to
21±2.8mmHg (p<0.001) (Fig. 7) and their RVP dropped from 87.5±5.9mmHg to 41±3.8mmHg
(p<0.001) (Fig. 8) making the success rate rise to 78%. BPV was performed
for 18 cases with dysplastic pulmonary valve and was successful in seven cases making
their success rate of 38.9%. Eighteen patients (13.6%) with mild to moderate
infundibular stenosis of 33±18mmHg, four of them had subpulmonic obstruction before
BPV and persisted after balloon dilatation, whereas the other ten showed
improvement with the use of ß- Blockers (propranolol of a dose of 1mg/kg/dose
twice or thrice daily) which was given for two to three months. Fifteen patients (11.36%)
needed surgery after BPV, eleven due to dysplastic valve and four due to fixed
subvalvular obstruction. Patients below two years of age had their peak to peak
PG pre BPV significantly higher than those who were above two years (98±35.6
mmHg vs. 86±26.5 mmHg P=0.03) (Fig. 9) and has a higher rate of re-stenosis post
BPV (mean PG=75±2.2 mmHg for 27 patients below two years vs. 55±1.4mmHg for 18 patients
above two years; P<0.001) (Fig. 10). Eight
patients missed their follow up. During follow up, for those who came back 126
cases, the residual peak instantaneous gradient dropped further from 24.4± 3 to
19±6mmHg with P<0.001 (Fig 11).
Grade I-II pulmonary valve regurgitation
was noticed in 34 (27.8%) patients at
one year and in 43 (38%) patients, at mid term follow up range (range 5 months
to 5.2 years), 28 patients out of 43 had grade II regurgitation, their mean PG
was 75±2.2 before BPV, they had statistically significant more regurgitation (grade
II) than the 15 patients who had grade I
regurgitation with their mean PG being 55±1.4
and P<0.001 (Fig. 12), but neither right ventricle dilatation or impairment nor
paradoxical interventricular septum motion occurred. Mortality rate of those
who came back for follow up 124 (93.9%) cases was 0%, immediately and on
mid-term follow up.
Discussion
Pulmonary valve stenosis is one of the common
congenital heart diseases.(20) The traditional method of treatment was surgical valvotomy
until 1982, when Kan et al.(3) introduced the
technique of percutaneous balloon valvuloplasty.(2,4,20) Since that time, it replaced the
surgical option except for few exceptions: pulmonary valve hypoplasia or the
presence of concomitant intra cardiac defects which need to be addressed at the
same time.(21) Although the majority of our
patients with pulmonary valve stenosis were asymptomatic, our rationale for taking our
patients for BPV when their peak to peak maximum PG≥5OmmHg in order to prevent
and relieve the symptoms, to prevent the secondary changes in the right
ventricle and the pulmonary artery and to prevent the progression into more
severe degrees of obstruction.(6,22) We noticed also that re-stenosis rate was
higher in patients who were below two years of age and actually these cases had
their peak to peak PG before BPV significantly higher than those above two years
(P=0.001), this also was noticed by Ray et
al.,(27) and McCrindle
et al.(28) The subvalvular stenosis of the
right ventricle outflow tract was noticed immediately post BPV in 13.6% of patients. These patients
received propranolol for 2-3 months period with obvious regression of the
subpulmonic obstruction. B-blockers also were used by Fawzy et al.,(29)
Kassab et al.,(30) Moullaert et al.,(6)
Thapar et al.(31) and Fontes et al.,(32)
but we can't draw a conclusion if that regression
was due to B-blockers’ effect or was spontaneous due to time, as many studies
noticed that the infundibular hypertrophy is reversible in children.(1,20,23-24)
In the current study, over the six year period (range
5 months to 5.2 years) of following up our patients, we noticed also that the
residual peak instantaneous gradient had dropped significantly by time, even in those who
needed re-intervention. The regression
of residual gradient was noticed also by Mahnert et al.(33)
over a period shorter than two years in 10 out of 19 cases the PG dropped
significantly without any other additional intervention. Also we noticed that
the success rate for patients with dysplastic pulmonary valve was 38.8% in
comparison with patients with normal
pulmonary valve 78% but it was not of statistical significance (P=0.15), but
this may be explained by the small number of cases (n=18).
There were studies that indicated the occurrence of
pericardial effusion post valvotomy(1,16,18) but
this was not encountered in our patients. The incidence of pulmonary valve
regurgitation increased over the follow up period to 38% and it was near most
published series.(4,11,14,25,26) Possible
contributory factors of regurgitation are exacerbation of the anatomic
perturbations such as, irregular leaflet tears in the immature valves or
avulsions with time. The pulmonary regurgitation was significantly more in
cases with higher mean PG pre BPV and those below two years of age. Garty et al.(34) and
Rao(35) also noticed that children with small age at the time
of dilatation were more likely to develop moderate to severe PR during follow
up, but in our cases the pulmonary regurgitation was of mild degree, tolerated
by the patients and there was no evidence of right ventricle dilatation or
impairment. No immediate or late deaths
occurred.
Conclusion
The Balloon pulmonary valvotomy should be the
procedure of choice in the treatment of isolated pulmonary stenosis regardless
of the severity, because it is safe and effective in treating pulmonary valve
stenosis, improving their symptoms and saving the right ventrivular function, leaving
surgery for those with unsuccessful balloon valvuloplasty. The result of
balloon dilatation of dysplastic pulmonary valve was suboptimal. Subpulmonic
obstruction post BPV may be regressed spontaneously. The pulmonary
regurgitation was of mild degree, tolerated by the patients and there was no
evidence of right ventricle dilatation or impairment. Longer-term
follow up is needed to evaluate the significance of pulmonary valve regurgitation.
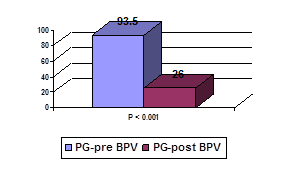
Fig. 5. Mean peak to peak PG mmHg pre and post BPV
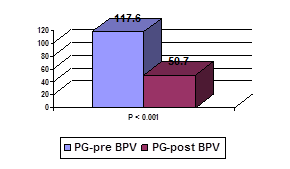
Fig. 6.
Mean RVP pre and post BPV in mmHg
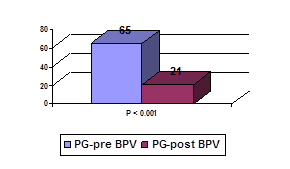
Fig.7.
Restenosis cases: Mean peak to peak PG in mmHg
Fig. 8. Restenosis cases: Mean PVR pre and post BPV in
mmHg
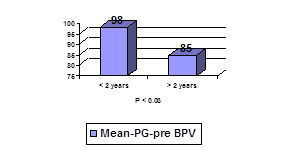
Fig. 9.
Mean PG-pre BPV
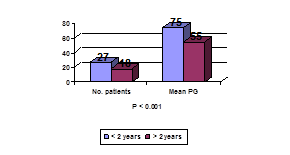
Fig.10.
Restenosis cases
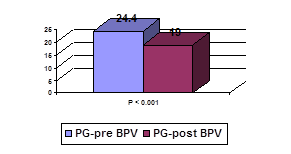
Fig. 11. At
six years follow-up-mean peak instantaneous PG in mmHg
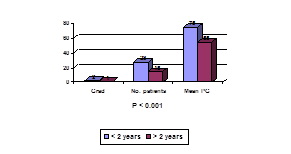
Fig. 12. Pulmonary
regurgitation
References
1.
Wang
JK, Wu MH, Lee WL, et al. Balloon
dilatation for critical pulmonary stenosis. Inter J Card 1999; 69: 27-32.
2.
Fawzy
ME, Awad M, Galal O, et al. Long-Term Results of Pulmonary Balloon Valvulotomy in Adult Patients. J
Heart Valv Dis 2001;10:
3.
Kan
JS, White RI Jr, Mitchell SE, et al. Percutaneous balloon valvuloplasty: A new method for
treating congenital pulmonary valve stenosis. N Engl J Med 1982; 307:540-542.
4.
Rao
PS, Galal O, Patnana M, et al. Results of three to 10 year follow up of balloon dilatation of the
pulmonary valve. Heart 1998; 80: 591-595.
5.
Rao
PS. Percutaneous balloon
pulmonary valvuloplasty: State of the art. Catheter cardiovasc. Interv 2007;
69(5):747-763
6.
McCrindle
BW, Kan JS. Long-term results after balloon pulmonary valvuloplasty.
Circulation 1991; 83:1915-1922.
7.
Stanger
P, Cassidy SC, Girod DA, et al. Balloon pulmonary valvuloplasty: results of the valvuloplasty and
angioplasty of congenital anomalies registry. Am J Cardiol 1990; 65: 775-783.
8.
Fontes
VF, Estwves CA, Sousa JEMR, et al. Regression of infundibular hypertrophy after pulmonary
valvuloplasty for pulmonic stenosis. Am J Cardiol 1988; 62: 977-979.
9.
Fontes
VF, Sousa JEMR, Esteves CA, et al. Pulmonary valvuloplasty- Experience of 100 cases. Int
J Cardiol 1988; 21:335-342.
10. Lee ML, Wang JK. Percutaneous transluminal pulmonary valvuloplasty for
severe to critical valvular pulmonary stenosis in neonates and infants. Acta
Paediatr Taiwan 2004 Jul- Aug; 45(4): 224-228
11. Hatem DM, Castro I, Haerrtel JC, et
al.
Short and long term results for
percutaneous balloon valvuloplasty in pulm. Valve stenosis. Arq Bras Cardiol 2004; 82(3): 221-227
12. Juarez RM, Alva EC, Ledesma VM, et al. Balloon
pulmonary valvuloplasty, 15 year experience at the Silgo XXI IMSS
National Medical
Center. Arch
Cardiol Mex 2003; 73(3):190-196
13. Echigo S. Balloon valvuloplasty for congenital heart disease:
Immediate and long-term results of multi-institutional study. Pediatr Int 2001 Oct; 43(5):542-547
14. Akcurin G, Kahramanyol O, Tatakan C. Intermediate –term follow –up results of pulm.balloon
valvuloplasty in children. Turk J Pediatr 2000; Apr- Jun;42 (2): 126-131
15. Cazzaniga M, Quero JC, Fernandez PL, et
al. Balloon pulmonary
valvuloplasty on the neonatal period. The clinical and echocardiograhic
effects. Rev Esp Cardiol 2000 Mar; 583(3): 327-336
16. Thanopoulos BD, Margetakis A,
Papadopoulos G, et al. Valvuloplasty with large trefoil balloons for the
treatment of congenital pulmonary stenosis. Acta Paediatr Scand 1989; 78:742-746.
17. Rao PS, Mardini MK. Pulmonary valvotomy without thoracotomy: The
experience with percutaneous balloon pulmonary valvuloplasty. Ann Saudi Med
1985; 5:149-155.
18. Rao PS. Balloon pulmonary valvuloplasty for isolated pulmonary
stenosis. In: Rao PS, ed. Transcatheter therapy in pediatric cardiology. New York: Wiley Liss,
1993:59-104.
19. Witsenburg M, Talsma M, Rohmer J, Hess
J. Balloon valvuloplasty for
valvular pulmonary stenosis in children over 6 months of age: initial results
and long term follow up. Eur H J
1993; 14:1657-1660.
20. Chen CR, Cheng TO, Huang T, et al. Percutaneous balloon valvuloplasty for pulmonic
stenosis in adolescsnts an adults. N Eng J Med 1996; 335:21-25.
21. Peterson C, Schilthuis JJ,
Dodge-Khatami A, et al.
Comparative long-term results of surgery versus balloon valvuloplasty for
pulmonary valve stenosis in infants and children. Ann Thorac Surg 2003; 76:1078-1083.
22. Nugent AS, Freedom RM, Nora JJ, et
al. Clinical course in
pulmonary stenosis. Circulation 1977; 56: 38-47.
23. Colli AM, Perry SB, Lock SE, Kean SF. Balloon dilatation of critical valvar stenosis in the
first month of life. Cathet Cardiovasc Diagn 1995; 34:23-28.
24. Gournay V, Piechaud SF, Delogu A, et
al. Balloon valvotomy for
critical stenosis or atresia of pulmonary valve in newborns. J Am Coll
Cardiol 1995; 29: 1725-1731.
25. Tabatabaei H, Boutin C, Nykanen DG, et
al. Morphologic and
hemodynamic consequences after percutaneous balloon valvotomy for neonatal
pulmonary stenosis:medium-term follow-up. J Am Coll Cardiol 1996; 27:473-478.
26. O’Connor BK, Beekman RH, Lindaur A, et
al. Intermediate-term
outcome after pulmonary balloon valvuloplasty: comparison with a matched
surgical group. J Am Coll Cardiol 1992; 20:169-173.
27. Ray DG, Subramanyan R, Titus T, et
al. Balloon pulmonary
valvuloplasty: factors determining short-and long-term results. Int J
Cardiol 1993; 40:17-25
28. Fawzy M, Awad M, Galal O, et al. Long term results of balloon valvulotomy in adults
patients. The Journal of Heart Valve Diseases 2001; 10: 100-105
29. Kasab S, Ribeiro PA, AL-Zaibag M, et
al. Percutaneous double balloon pulmonary
valvotomy in adults: one-to two- year-follow-up. Am J Cardiol 1988; 62: 822-824
30. Moulaert AJ, Buis-Lisem TN,
Geldof WC, et al. The
postvalvulotomy propranolo test to determine reversibility of thr esidual gradiwent
in pulmonary stenosis. J Thorac
Cardiovasc Surg 1976; 71: 865-8
31. Thapar MK, Rao PS. Significance of infundibular obstruction following
balloon valvuloplasty for valvar pulmonic stenosis. Am Heart J 118(1989):
pp.99-103
32. Fontes VF, Esteves CA, Sousa J, et
al. Regression of
infundibular hypertrophy after pulmonary valvuloplasty for pulmonic stenosis. Am J Cardiol 1988; 62: 977-979
33. Mahnert B, Paul TH, Luhmer I, et al. Medium-to long-term results after percutaneous balloon
pulmonary valvuloplasty in childhood. Z Kardiol 1996; 85:482-8
34. Garty y, Veldtman G, Lee K, et al. Late outcomes after pulmonary valve balloon dilatation
in neonates, infants and children. The Journal of Invasive Cardiology 2005;
17(6): 318-322
35. Rao PS. Balloon pulmonary valvuloplasty in children. The
Journal of Invasive Cardiology 2005; 17(6): 323-325