Abstract
Objective: Nipple-areola reconstruction represents
the final stage of breast reconstruction. Many nipple reconstruction techniques
are available using either local flaps or free composite grafts. Maintenance of
nipple projection has always been the biggest problem with the various
techniques. We report our results with
nipple reconstruction using the modified double-opposing tab (MDOT) flap
technique as described by Kroll that we have been using for the past three years.
Methods: Because nipple
projection tends to decrease for several months after reconstruction with any
technique, only patients with a follow-up of at least three months after nipple
reconstruction were included in the analysis. Over the last three years 28 patients
underwent 31 nipple reconstructions using the modified double-opposing tab flap
technique (one bilateral and two revisions) at King Hussein Medical Centre and
King Hussein Cancer Centre. All 28 patients had previous breast reconstructions
by the authors at least three months prior to the nipple reconstruction; 12
patients had had immediate reconstruction and 16 patients had delayed reconstruction.
The outline of the areola was defined with a round
template in an appropriate location and the modified double-opposing tab flaps were raised within this circle. The axis of the
flaps varied with the location of the breast scars. Donor sites were
primarily closed and all resulting scars contained within the planned areola so
as to be completely camouflaged by later intradermal tattoo to be performed four months postoperatively. All but five
cases that required surgery on the other breast were done under local anesthesia.
Results: Age range was 28-55 years (mean 39.5 yrs). The duration of the procedure varied from 30-45 minutes. Three nipples in the series suffered partial necrosis from ischemia of which two needed revisions due to loss of projection. The third nipple healed spontaneously and maintained adequate projection. All three complications occurred in the first five patients and were due to inexperience with the technique. The average reduction of projection at three months was 48.3% of the original projection. All patients were satisfied with the final projection and symmetry.
Conclusion: The technique
is simple and permits freedom in choosing the height of the nipple, even in the
presence of scars. The dissection is straightforward and the technique is rapid
with few complications after a short learning curve.
Key words: Nipple, Breast, Reconstruction,
MDOT
JRMS
June 2010; 17(2): 53-57
Introduction
Although reconstruction of the nipple-areola complex
is an optional procedure, it significantly improves patients’ satisfaction with
breast reconstruction.(1,2) Nipple-areola reconstruction
represents the final stage of breast reconstruction and is usually performed
with a second operative procedure, although it can be deferred to a third
procedure.
Table I. Demographic data (n=28)
| Age (Years) |
Range
|
28-55
|
|
Median
|
39.6
|
|
Site
|
Left
: Right : Bilateral
|
14:13:1
|
|
Anaesthesia
|
Local:
General
|
23:
5
|
|
Contra lateral Nipple
Projection (Millimeters)
|
Range
|
3-15
|
|
Mean
|
7.1
|
Table II. Type of previous breast
reconstruction (n=28)
|
Type
of Reconstruction
|
Number
|
%
|
|
Immediate LDMCF* only
|
8
|
28.7
|
|
Immediate LDMCF* + implant
|
2
|
7
|
|
Immediate implant only
|
2
|
7
|
|
Delayed LDMCF* only
|
1
|
3.6
|
|
Delayed LDMCF* + implant
|
6
|
21.5
|
|
Delayed Free DIEAPF†
|
7
|
25
|
|
Delayed Free SGAPF•
|
1
|
3.6
|
|
Delayed Free SIEAF‡
|
1
|
3.6
|
*: Latismus Dorsi myocutaneous
flap. †: Deep Inferior
Epigastric Artery Perforator Flap.
•: Superior Gluteal
Artery Perforator Flap. ‡ :
Superficial Inferior Epigastric Artery Flap.
In our centre it is typically done at least three months after reconstruction of the breast mound.
Nipple reconstruction can be done with a variety of techniques, including
nipple sharing, in which a part of the nipple from the opposite breast is
grafted to the reconstructed breast, and the use of local flaps.(3,4)
Both can be done under local anesthesia as day case procedures. The areola is
now commonly reconstructed with intradermal tattooing.
Maintenance of nipple
projection has always been the biggest problem with the various techniques. In
this study we review our results of nipple reconstruction using our favored
method, the MDOT flap.
Methods
During the period
from May 2005 and June 2008 twenty eight female patients underwent 31 nipple
reconstruction procedures using the MDOT flap technique at King Hussein Medical
Centre (KHMC) and King Hussein Cancer Centre (KHCC). Because nipple projection
tends to decrease for several months after reconstruction with any technique,
only patients with a follow-up of at least three months after nipple
reconstruction were included in the analysis.
The
median age was 39.5 years (range 28-55 yrs). There were 14 right sided nipples,
13 left sided nipples and one patient with bilateral nipples. All but five
cases that required surgery on the other breast were done under local anaesthesia.
The existing (contra lateral) nipple projection was measured preoperatively and
recorded (Average 7.1mm, Range 3-15mm) (see Table I ).
All 28 patients
had previous breast reconstructions by the authors at least three months prior
to the nipple reconstruction. Eight patients (28.7%) had immediate Latismus
Dorsi myocutaneous flap (LDMCF) only, two patients (7%) had Immediate Latismus
Dorsi myocutaneous flap with implant, two patients (7%) had immediate implant
only reconstruction, one patient (3.6%) had delayed LDMCF only, six patients
(21.5%) had delayed LDMCF with implant, and nine patients (32.2%) had late
reconstruction using free tissue transfer (see Table II).
Surgical technique
The MDOT flap technique was carried as
originally described by Stephen Kroll in 1989 and its later modification in
1999.(5-8) The outline of the areola was defined
with a round template in an appropriate location and the MDOT flaps were raised
within this circle (Fig.1). The axis of the flaps varied with the location of
the breast scars. The width of the
flaps ranged from 18-22 mm and the thickness about 8mm to maximize blood
supply. The lengths of the flaps at the short limb varied from 20-30mm
depending on projection of contra lateral nipple. Donor sites were primarily
closed and all resulting scars contained within the planned areola so as to be
completely camouflaged by later intradermal tattoo to
be performed four months postoperatively (Fig.2).
Table III. Results of the reconstructed
nipple projection.
|
Projection created at
surgery (Millimeters)
|
Range
|
5-22
|
|
Mean
|
11.5
|
|
Projection at surgery
(Percentage of contra
lateral nipple)
|
Range
|
135%-250%
|
|
Mean
|
179%
|
|
Projection of new nipple
at three months (Millimeters)
|
Range
|
0-12
|
|
Mean
|
6.1
|
|
Percent reduction in nipple
Projection at three months
|
Range
|
26.6%-76.9%
|
|
Mean
|
45%
|
Fig. 1. Surgical Technique
A: The outline of the areola defined using a round template. B: MDOT
flaps were raised within the outlined circle.
C:
Primary closure of the donor site. D:
Final intra operative appearance after closure.
All patients were
operated upon by the same team of plastic and reconstructive surgeons at KHMC
and KHCC 3-18 months after breast reconstruction depending on extraneous
factors such as oncological aspects of the disease and patient’s
preference. Nipple projection was
measured intra-operatively and at three months post operatively, the reduction
in projection was recorded. Also patient and surgeon satisfaction was recorded
at three months.
Results
The duration of
the procedure varied from 30-45 minutes. The average new nipple projection at
time of surgery was 11.5mm (Range: 5-22mm). Nipple projection was made to be
around 180% of the contra lateral nipple (Range: 135%-250%). At three months
the average nipple projection was 6.1 mm (Range: 0-12mm), this reflects a 45% average reduction in the projection (Range: 26.6%-76.9%)
(see Table III).
Three nipples in
the series suffered partial necrosis from ischemia of which two needed
revisions due to loss of projection (Fig. 3). The third nipple healed
spontaneously and maintained adequate projection. All patients were satisfied
with the final projection and symmetry. Even those who underwent revision had
satisfactory projection (Fig. 4). There were no cases of nipple retraction in
this series.
Discussion
Historically many techniques
have evolved for nipple reconstruction.
Basically, those can be classified in three main categories:
1. Those that
utilize transferring tissues from distant areas such as the contra lateral
nipple or the toes.(9)
2.
Techniques that use local tissue flaps such as the
skate flap, star flap, C-V flap, top hat flap, double opposing pennant and tab
flap and others.(4,10-14)
3. Others that
combine the above mentioned techniques.(15-17)
Reconstruction of the nipple areola complex (NAC) is an integral component
of any type of breast reconstruction.
|

Fig. 2. All scars contained within the planned areola

|
|
Fig. 3. Surgical complications A: Partial nipple necrosis that resolved spontaneously. B: Complete nipple necrosis
that needed later revision.
|
|
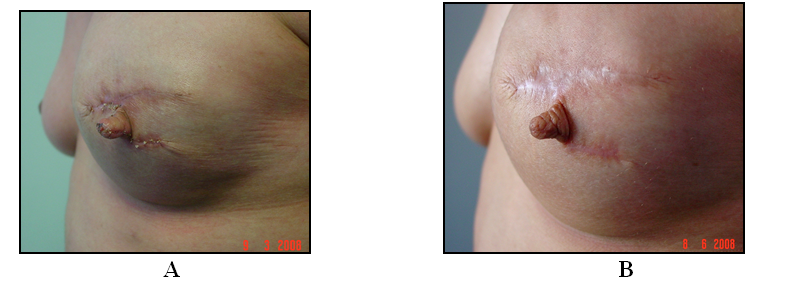
Fig. 4. Example of good projection
A: Projection
immediately postoperatively. B: Projection at three
months postoperatively

Fig. 5. Example of final
reconstruction result before tattoo.
A: Pre operatively. B: After full reconstruction and
contra lateral breast augmentation
|
|
|
It marks the end point of
breast reconstruction and, for many women, a final stage of their emotional
struggle with their body image (Fig. 5). Nonetheless many patients used to
refuse this step because they did not want any further scarring in other areas
that might further distort their body image.(2) This led to
the evolution of several local flap techniques for NAC reconstruction.
The MDOT flap technique for
nipple reconstruction offers several advantages over the other local flap
techniques; firstly the flaps in this method are thicker and wider at their
base and are tapered at their tip with preservation of the sub dermal plexus
there which would influence the viability of the flaps and hence the long term
projection. Furthermore the M shape created at the distal end of each flap
facilitates interdigitation of the two flaps when closed; this creates a natural
looking round nipple rather than a pointed tip nipple. Also in this technique
one can control the direction of the flaps according to the existing scars,
since the direction of the flaps should be parallel to the
scar.(5-7)
Timing of NAC reconstruction
is a very important issue. In all of our cases the procedure was delayed
till after the completion of breast mound reconstruction and contra lateral
breast surgery when needed. This aided in achieving better symmetry since the
position of the new NAC is usually a compromise between the position of the
contra lateral NAC and the position of the scars on the breast mound. Others
use immediate nipple reconstruction at the time of breast reconstruction, but
this has its drawbacks in achieving the required symmetry.(18-20)
Progressive loss of nipple
projection and nipple retraction are the two major drawbacks of most nipple
reconstruction techniques. In our series we had no cases of nipple retraction
and the average reduction in nipple projection was 45%. Since the projection at
time of surgery was originally made almost twice the contra lateral nipple then
the final symmetry was acceptable in almost all cases.
In our group of patients that
were followed up for more than one year (13 patients) we have noticed that
there was no dramatic drop in the projection over that occurring after three
months. This will need further follow up to study the long term maintenance of
nipple projection in this technique. Shestak and colleagues(21)
reported good projection at three months with the Skate flap and Modified Star
techniques; nonetheless there was dramatic decrease in projection at one year almost
double that at three months.
In his discussion on Kroll’s technique, Little(22) brought up a point that the MDOT flap technique works
perfectly for small or moderate-sized nipples, however when larger nipples
needed to be produced there will be undue tension when closing the donor sites
which will lead to gross loss of the projection. To overcome this Little(22) suggests that one should close the donor site with
minimal tension and then cover the rest with a narrow skin graft taken from
along the mastectomy scar.
Conclusion
In our series we had three
cases of nipple necrosis and this is a relatively high number, those three
complications occurred in the first five patients and in the last 28 nipples we
had no case of nipple necrosis. We assume that this was attributed to lack of
experience with the technique at the beginning.
References
1.
Cheng
MS, Ho CM, Cheung WY, Or A, Wong WM. Nipple-areola reconstruction in autologous breast reconstruction chinese
patients’ perspective. Ann Plast Surg. 2003; 53(4): 328.
2.
Losken
A, Carlson G, Hester R, et al. Factors that influence the completion of breast reconstruction. Ann
Plast Surg. 2004; 52(3): 258.
3.
Garramone
CE, Lam B. Use of alloderm in
primary nipple reconstruction to improve long-term nipple projection. Plast
Reconstr Surg 2007; 119:1663.
4.
Eo
S, Kim S, Da Lio A. Nipple reconstruction
with c-v flap using dermofat graft.
Ann Plast Surg 2007; 58(2): 137.
5.
Kroll
S, Hamilton S. Nipple reconstruction
with the double opposing tab flap. Plast Reconstr Surg 1989; 84(3):520.
6.
Kroll
S, Reece G, Miller M, et al. Comparison of nipple projection with the modified double-opposing tab
and star flaps. Plast Reconstr Surg. 1997; 99(6):1602.
7.
Kroll
S. Nipple reconstruction with
the double opposing tab flap (Follow up). Plast Reconstr Surg. 1999;
104(2):511.
8.
Bostwick
J. Nipple reconstruction with
the double-opposing tab flap (discussion). Plast Reconstr Surg 1989;
84(3):516.
9.
Liew
S, Disa J, Cordeiro PG. Nipple–areolar
reconstruction: a different approach to skin graft fixation and dressing. Ann
Plast Surg 2001; 47(6): 608.
10. Gamboa-Bobadilla G M. Nipple reconstruction: the top hat technique. Ann
Plast Surg. 2005; 54(3): 243.
11. Shestak KC, Gabriel A, Landecker A, et
al. Assessment of long-term
nipple projection: a comparison of three techniques. Plast Reconstr
Surg 2002; 110:780.
12. Tatlidede S, Yesilada A K, Egemen O,
Bas L. a new technique in
nipple reconstruction dome technique with double pedicle. Ann Plast Surg.
2008; 60(2): 141.
13. Shestak KC, Nguyen TD. The double opposing periareola flap: a novel concept
for nipple-areola reconstruction. Plast Reconstr Surg 2007; 119(2): 473.
14. Narra K. A new approach to nipple reconstruction: the modified
s-flap. Plast Reconstr Surg 2007; 122(2):89e.
15. Guerra A, Khoobehi K, Metzinger S,
Allen R. New technique for nipple
areola reconstruction: arrow flap and rib cartilage graft for long-lasting
nipple projection. Ann Plast Surg 2003; 50(1): 31.
16. Cheng M, Rodriguez E, Smartt J,
Cardenas-Mejia A. Nipple reconstruction
using the modified top hat flap with banked costal cartilage graft long-term
follow-up in 58 patients. Ann Plast Surg 2007; 59(6): 621.
17. Evans K, Rasko Y, Lenert J, Olding M. The use of calcium hydroxylapatite for nipple
projection after failed nipple-areolar reconstruction early results. Ann
Plast Surg 2005; 55(1):25.
18. Williams E, Rosenberg L, Kolm P, Torre
J, Fix R. Immediate nipple
reconstruction on a free tram flap breast reconstruction. Plast Reconstr
Surg.2007; 120(5):1115.
19. Oehlbauer M, Schoeller T, Piza-Katzer
H, Wechselberger G. One-stage
breast reduction and nipple–areolar reconstruction. Ann Plast Surg 2002;
49(5): 553.
20. Nahabedian M. Secondary nipple reconstruction using local flaps and
alloderm. Plast Reconstr Surg 2005; 115(7):2056.
21. Shestak KC, Gabriel A, Kim J, et al.
Assessment of long-term nipple projection:
a comparison of three techniques. Plast Reconstr Surg 2002; 110(3):780.
22. Little JW. Nipple reconstruction with the double-opposing tab
flap (Discussion). Plast Reconstr Surg 1999; 104(2):515.