ABSTRACT
Objective: In this study we present the use of
distally based adipofascial flaps from the calf for the reconstruction of soft
tissue defects of the lower third of the leg and proximal foot at
the Royal Jordanian Rehabilitation Center, King Hussein Medical Center over a
three-year period between 1998 and 2001.
Methods: Eleven
patients were treated and were analyzed with respect to age, gender, etiology
of defect, defect site, defects size, the adipofascial flap artery used and the
outcome with a follow up of 1-3 years at the Royal Jordanian Rehabilitation
Center, King Hussein Medical Center.
Results: There
were seven adults and four children. The etiologies of the soft tissue defects
were trauma in (8 patients), trophic ulcers (2 patients), and chronic
osteomyelitis in (one patient). All flaps survived completely, and stable
coverage of the soft tissue defects was achieved in all patients. One patient required repeat skin graft due to
partial loss of the graft.
Conclusion: The
simplicity of design and elevation of these flaps plus their extensive arc of
rotation makes the adipofascial flaps versatile and reliable in the
reconstruction of difficult defects of the lower limbs. We have found these
flaps to be safe, technically easy and with minimal donor site morbidity.
Key words: Flaps, Adipofascial, Lower limb
reconstruction.
JRMS
June 2004; 11(1): 38-43
Introduction
In 1976 distally based vascular pedicle flaps were
introduced to reconstructive surgery (1). Many studies
confirmed that reverse venous flow occurred in these distally based pedicles,
encouraged surgeons to develop various flaps in reconstructive surgery of the
limbs (2). For the reconstruction of soft tissue defects of
the lower leg and foot the peroneal arterial flaps (3),
anterior tibial arterial flaps (4) and the posterior
tibial arterial flaps (5) were used as
adipofascial flaps.
Soft
tissue defects of the lower third of the leg and foot with exposed bone present
difficult reconstructive challenges for plastic surgeons. As an alternative to
microvascular transfer in patients in whom local skin or
muscle flaps are not suitable, the fasciocutaneous system of the leg offers a
good alternative. Ponten (6) introduced the fasciocutaneous
flaps, which proved satisfactory for small and medium-sized defects.
Furthermore, the adipofascial flap, which is a fasciocutaneous flap without the
overlying skin, was developed (7).
In this study we present the use of distally based
adipofascial flaps from the calf for the reconstruction of soft tissue defects
of the lower third of the leg and proximal foot. The clinical results are
encouraging and the advantages are discussed.
Methods
This is a retrospective study of the distally based adipofascial
flaps in the reconstruction of the lower third of the leg and proximal foot
defects treated at the Royal Jordanian Rehabilitation Center, King Hussein
Medical Center, Jordan over a three-year period between 1998 and 2001. Eleven
patients were treated and were analyzed with respect to age, gender, etiology
of defect, defects site, defects size, the adipofascial flap artery used and
the outcome with a follow up of 1-3 years.Surgical Anatomy
The main nutrient vessels of the leg are the anterior tibial
artery, posterior tibial artery, and peroneal artery. Each artery supplies a
separate territory although some of the skin areas overlap (8).
The posterior tibial artery passes inferomedially on the posterior surface of
the tibialis posterior muscle and deep in the transverse facial septum, which
separates the soleus and gastrocnemius from the deep muscular compartment of
the posterior leg. Along its course, the posterior tibial artery gives off many
branches and intermuscular perforators to the underlying fascia and skin. In
its upper 2/3 the artery is deep. In the rest of its course it is superficial.
In the distal third the perforators are more numerous than in the proximal
third (9).
Also it is well known that the cutaneous veins have their
own accompanying arteries that have branches to the skin i.e. venocutaneous
perforators. Along with the neurocutaneous perforators of the cutaneous nerves
the concept of adipofascial fasciocutaneous flaps was proposed (10).
Prior to performing the operation, assessment of the artery
and the perforators should be carried out by palpation or Doppler. When in
doubt, an arteriogram of the leg and foot should be obtained. The flap is
marked on the skin with its pivot vascular pedicle 6-8 cm proximal to the
malleoli (Fig. 1a and Fig. 1b). A linear or zigzag skin incision is made along
the course of the artery. Then the dissection is
made subcutaneously over the area of the proposed adipofascial flap (Fig. 1c).
The flap is raised (Fig. 1d) and the vessels are
easily identified under the thin adipofascial layer (Fig. 1e) and a cuff of
subcutaneous tissue and fascia is left with the pedicle so that perforators can
be preserved to maintain the blood supply of the flap. Then the flap is turned
over to inset and fill the defect (Fig. 1f). The donor area is closed primarily
without tension (Fig. 1g). Then a split thickness skin graft is applied over
the flap (Fig. 1h and Fig. 1i).
The deep fascia is absent on the medial surface of the tibia
and lower exposed surface of fibula. Immediately after piercing the deep fascia
the intermuscular perforators ramify and anastomose with each other to form a
rich vascular plexus at the pre-and sub fascial levels (11).
After rotation of the flap to the recipient area then the
raw surface is covered with a skin graft and the donor area is closed
primarily. The dermal vascular network at the donor site is sufficient to let
the skin survive without its underlying subcutaneous vascular support although
it is wise to trim the edges before closure to avoid minor healing problems.
Occasionally we apply a skin graft over the turned over pedicle to avoid tight
primary closure over the pedicle.
The anterior tibial artery has 2-3 medial perforators
through the tibialis anterior along the anterior border of the tibia and 6
lateral perforators along the anterior peroneal septum. The peroneal artery has
5 perforators along the posterior peroneal septum and one perforator that
pierce interosseous membrane above the ankle and a lateral malleolar branch.
The posterior tibial artery has 4 perforators between the flexor digitorum
longus and the soleus muscle also has malleolar and calcaneal branches.
Results
There were 9 males and 2 females, seven adults and four
children ranging from 5 years to 63 years. The etiologies of the soft tissue
defects were trauma in 8 patients (72%), trophic ulcer in 2 patients (18%) and
chronic osteomyelitis in one patient (9%). The defect sites were divided into
three areas: lower third of the leg, dorsum of the foot and heel. There were four
patients in each of the first and second groups and three patients in the third
group. The defect size ranged from 3x2 cm to 8x6 cm. The arterial pedicle used
for these adipofascial flaps were: six peroneal artery perforators and five
posterior tibial artery perforators (Table I). All the flaps were covered with
split thickness skin grafts and the donor sites were closed primarily in all
cases. All flaps survived completely with stable coverage of the soft tissue
defects. One patient required repeat skin graft due to partial loss of the
graft. All the donor sites healed completely with cosmetically accepted scars
and the patients were satisfied with the scars.
None of the patients needed a debulking procedure for the flaps. Examples of
the results are shown in (Fig. 1j), (Fig. 1k), (Fig. 2a, b) and (Fig. 3a, b).
Discussion
In the reconstruction of lower leg defects, a problem arises
which is the lack of available and reliable local flaps. Microvascular tissue
transfer can provide ample tissue for reconstruction but a high incidence of
free flap failure occurs in this region (12). The flap maybe too bulky for the defect and a
secondary debulking operation may be necessary. High-energy trauma results in
tibial fractures as well as soft tissue and skin damage leading to skin
necrosis and tibial bone or plate exposure (13). Defects occurring in the proximal or middle
third of the leg may be covered by regional flaps such as soleus (14)
or gastrocnemius muscle flaps, musculocutaneous flaps and
proximally based fasciocutaneous flaps (6), however, scanty
soft tissue and poor blood supply renders reconstruction difficult when these
defects occur in the lower leg,
The fasciocutaneous flaps introduced by Ponten have no
definite vascular pedicle and thus need a wide base. In their experience Ponten
(6) and Barclay et al (15) found
that the fascial layer could survive a longer length of tissue than that of the
overlying cutaneous tissue after transplantation. Dickson et al (16)
found that in 14 out of 15 cases in which partial necrosis occurred, the
necrosis was limited to the skin, and the fascia was viable. Many studies
revealed that the deep fascia of the leg is a highly vascularized and reliable
tissue. A main artery of the leg can be dissected to support a large axial
flap. These island flaps have a large axis of rotation. In order not to
sacrifice a major artery, a distally based fasciocutaneous flap nourished by
lower perforators originating from the
posterior tibial artery can be used (5). If
the direction of the vascular pedicle is not changed the blood flow in the flap
is not retrograde in spite of the fact that its base was distal, therefore no
problem of venous congestion is encountered as can occur in a reversed vascular
pedicle flap. These flaps could be designed as island flaps and could be
transposed 90 or 180 degrees since their vascular pedicle can
supply a large
skin territory and
can provide a durable and
thin coverage of
the Achilles tendon (17, 18).
Each adipofascial flap was nourished by lower perforators
originating from the posterior tibial artery and these perforators were
identified in five cases in this series. Gumener et al (19)
reported a reverse fasciocutaneous flap in the calf area that was nourished by
both the lower perforators of the posterior tibial artery and peroneal
arteries. El-Khatib used the perforators
of the dorsalis pedis artery for the resurfacing of the forefoot defects (20).
Also these flaps were based on the saphenous artery to cover the soft tissue defects
around the knee and superior third of the leg (21). A large
flap could be used as a cross leg fasciocutaneous flap to cover the whole leg
defect (22) and a large base to accommodate the
two perforators but extensive dissection is needed for a successful
transplantation, which sometimes
causes transit edema
in the
leg. In our series the width of the flaps did not exceed 10 cm and the maximum
length was up to 10 cm below the level of the knee. The donor site scar was
satisfactory to our patients but a new technique to harvest these flaps using
the endoscopic assistance was done to decrease the donor site morbidity (23).
The requisites for adipofascial flap survival are:
Pre-operative Doppler assessment of perforators at proposed pivot point, good flap
design, adequate flap to base area and length to width ratio, dissection of
vessels at pivot point avoids kinks and noncompressive dressing. In our series
the patients were immobilized for one week and a light dressing was used
especially over the area of the pedicle. We had one case of partial loss of the
graft that needed repeat skin graft but we had no cases of a discharging sinus
as reported by others (24).
These flaps are gaining popularity in soft tissue coverage
of the extremities thus creating a new concept in reconstructive surgery within
the last decade (25, 26).
Conclusion
The simplicity of design and elevation plus their extensive
arc of rotation make the adipofascial flaps versatile and reliable in the
reconstruction of difficult defects of the lower limbs. We have found several
advantages of these flaps. They include (1) safety; (2) reliability,
longitudinally oriented axial- pattern flap; (3) technically easy and quick
dissection; (4) availability in either the fatty tissue side or the fascial
side; (5) single stage without microsurgery; (6) no sacrifice of skin or major
arteries or nerves at donor site; (7) potential for reinnervation with minimal
donor site morbidity; (8) softness and conformability, and the ability to
obliterate the dead space completely.
The addition of this technique to the armamentarium of
reconstructive surgeon has proved useful in repairing soft tissue defects.
Table
I. Demographic
characteristics, etiology and defect site, size
and the involved artery among the study group.
|
Patient No.
|
Age years
|
Gender
|
Etiology
|
Defect site
|
Defect size
|
Artery
|
|
|
1
|
28
|
Male
|
Trauma
|
Lower
1/3 leg
|
5x3
cm
|
Peroneal
|
|
|
2
|
6
|
Male
|
Trauma
|
Dorsum
foot
|
5x4
cm
|
Peroneal
|
Fig
2
|
|
3
|
5
|
Male
|
Trauma
|
Lower
1/3 leg
|
4x2
cm
|
Post.
tibial
|
|
|
4
|
11
|
Female
|
Trauma
|
Dorsum
foot
|
8x6
cm
|
Peroneal
|
|
|
5
|
35
|
Male
|
Trauma
|
Dorsum
foot
|
6x4
cm
|
Peroneal
|
|
|
6
|
19
|
Female
|
Trauma
|
Heel
|
3x3
cm
|
Post.
tibial
|
|
|
7
|
63
|
Male
|
Chronic
Osteomyelitis
|
Lower
1/3 leg
|
3x2
cm
|
Post.
tibial
|
|
|
8
|
27
|
Male
|
Trophic
ulcer
|
Heel
|
3x2
cm
|
Peroneal
|
|
|
9
|
32
|
Male
|
Trophic
ulcer
|
Heel
|
4x3
cm
|
Peroneal
|
|
|
10
|
12
|
Male
|
Trauma
|
Dorsum
foot
|
8x4
cm
|
Post.
tibial
|
Fig
1
|
|
11
|
45
|
Male
|
Trauma
(Bullet injury)
|
Lower
1/3 leg
|
5x3
cm
|
Post.
tibial
|
Fig
3
|

Fig.
1: A 12-year-old male with trauma
over the dorsum of the right foot that resulted in a defect of 8x4 cm in size.
The defect was closed using a posterior tibial artery adipofascial flap. a) Pre operative. b) Marking of skin incision and the
perforator. c) Dissection of the proposed adipofascial flap. d) Elevation of
the flap. e) Identification of the perforators. f) Inset of the flap. g) Donor
area closed primarily. h) Split thickness skin graft applied over the flap. i)
Immediate post operative. j) After 3 weeks. k) After 6 weeks.

a) Pre-operative b) Post-operative after one year
Fig.
2. A
6-year-old male with trauma to the dorsum of the left foot, which resulted in a
defect of 5x4 cm requiring flap coverage. The defect was closed using a
peroneal artery adipofascial flap.
a) Pre-operative b) Post-operative after 6 weeks.
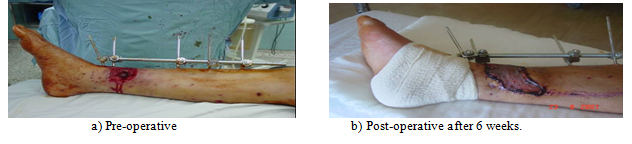
Fig.
3. A
45-year-old male with a bullet injury to the lower third of the right leg
that resulted in fracture of the tibia and a defect of 5x3 cm. The fracture was
fixed with external fixation. The defect was closed using a posterior tibial
artery adipofascial flap.
References
1. Bostwick J, Briedis J, Jurkiewicz, MJ. The reverse flow
temporal artery island flap. Clinics in Plastic Surgery 1976; 3:
441-445.
2. Timmons MJ. William Harvey
revisited: Reverse flow through the valves of forearm veins. Lancet
1984; 2: 394-397.
3. Yoshimura M, Imura S, Shimamura K, et
al. Peroneal flaps for reconstruction in the extremity:
Preliminary report. Plast Reconstr Surg 1984; 74: 402-407.
4. Rocha JFR, Gibert A, Masquelet A, et
al. The anterior tibial artery flap: Anatomy study and clinical
application. Plast Reconstr Surg 1987; 79: 396-401.
5. Amarante J, Costa H, Reis J, Soares R. A new distally
based fasciocutaneous flap of the leg. Br J Plast Surg 1986; 39:
338-342.
6. Ponten B. The
fasciocutaneous flap: its use in soft tissue defects of the lower leg. Br J Plast Surg 1981; 34: 215-220.
7. Lin SD, Lai CS, Chou CK, Tsai CW. The distally
based posterior tibial arterial adipofascial flap. Br J Plast Surg 1992;
45: 284-287.
8. Nakajima H, Minabe T, Imanishi N. Three
dimensional analysis and classification of arteries in the skin and
subcutaneous adipofascial tissue by computer graphics imaging. Plast
Reconstr Surg 1998; 102(3): 748-760.
9. Carriquiry C, Costa MA, Vasconez LO. An anatomic study of the septocutaneous
vessels of the leg. Plast Reconstr Surg 1985; 76: 354-358.
10. Nakajima
H, Imanishi N, Fukuzumi S, et al. Accompanying
arteries of the cutaneous veins and cutaneous nerves in the extremities:
Anatomical studyand
a concept of the venoadipofascial and/ or neuroadipofascial pedicled
fasciocutaneous flap. Plast Reconstr Surg 1998; 102(3):
779-791.
11.Cormack
GC, Lamberty BGH. A classification of fasciocutaneous flaps according to
their patterns of vascularisation. Br
J Plast Surg 1984; 37: 80-85.
12. Khouri
RK, Shaw WW. Reconstruction of the lower extremity with microvascular
free flaps: A 10- year experience with 304 consecutive cases. J Trauma
1989; 29: 1086-1090.
13. Byrd
HS, Spicer RE, Cierny G. Management of open tibial fractures. Plast
Reconstr Surg 1985; 76: 719-728.
14. Tobin
GR.
Hemisoleus and reversed hemisoleus flaps. Plast Reconstr Surg 1985; 76:
87-96.
15. Barclay
TL, Cardoso E, Sharp DT, Crockett DL. Repair of lower leg injuries
with fasciocutaneous flaps. Br J Plast Surg 1982; 35: 127-132.
16. Dickson
WA, Dickson MG, Robert AHN. The complications of fasciocutaneous
flaps. Ann Plast Surg 1987; 19: 234-238.
17. El-Khatib H.
Island adipofascial flap for resurfacing of the Achilles tendon. Plast
Reconstr Surg 1996; 98(6): 1034-1038.
18. Lin
SD, Lai CS, Chou CK, Tsai CW. The distally based posterior tibial
arterial adipofascial flap. Br J Plast Surg 1992; 45: 284-287.
19. Gumener
R, Zbrodowski A, Montandon D. The reversed fasciocutaneous flap in
the leg. Plast Reconstr Surg 1991; 88: 1034-1041.
20. El-Khatib
H.
Adipofascial turn over flap based on perforators of the dorsalis pedis for
resurfacing forefoot defects. An anatomic and clinical approach. Plast
Reconstr Surg 1998; 102(2): 393-397.
21. Lin
SD, Lai CS, Chiu YT, et al. Adipofascial flap of the lower
leg based on the saphenous artery. Br J Plast Surg 1996; 49: 390-395.
22. Kohli
JS, Pande S, Bajaj SP. Large transverse fasciocutaneous leg
flap: Whole leg flap. Br J Plast Surg 2000; 53: 495-498.
23. Hallock
GG. Adipofascial
flap harvest using endoscopic assistance. Ann Plast Surg 1997; 38(6):
649-652.
24. Lin
SD, Lai CS, Tsai CC, et al. Clinical application ofthe
distally based medial adipofascial flap for soft tissue defects on the lower
half of the leg. J Trauma 1995; 38(4): 623-629.
25. Lin
SD, Lai CS, Chou CK, Tsai CC.
Reconstruction of the soft tissue defects of the lower leg with a distally
based medial adipofascial flap. Br J Plast Surg 1994; 47: 132-137.
26. Sarhadi
NS, Quaba AA. Experience with the adipofascial turn over flap. Br J
Plast Surg 1993; 46: 307-313.