Abstract
Dental prosthesis may be swallowed as
well as aspirated that may result in acute medical or life threatening
emergencies. A case of asymptomatic
accidental swallowing of a four-unit anterior bridge is reported and the
attention is drown to the fact that, the patient was not sure if the bridge was
ingested or lost, while her main concern was esthetic as a result of the lost bridge. Patients with dental prosthesis should be
informed of this potential risk of swallowing.
JRMS
Dec 2004; 11(2): 44-46
Introduction
Swallowing of
dental materials and devices may be a serious complication during routine
dental treatment. In general, the
majority of foreign body ingestions occur in the pediatric population (1).
In adults, true foreign object ingestion occurs more commonly among those with
psychiatric disorders, mental retardation, or alcohol impairment, and those
seeking some secondary gain with access to a medical facility (2,3). The majority of foreign bodies that reach the
gastrointestinal tract will pass spontaneously, however, 10-20% may require
non-operative intervention, and 1%, or less may require surgery. Patients with
prior gastrointestinal tract surgery or congenital gut malformations are at
increased risk for obstruction or perforation (4). Once
passed through the esophagus, the majority of ingested foreign bodies pass
through the alimentary tract uneventfully. The risk of perforation is higher when sharp
or pointed metallic objects are ingested (5).
Swallowing incidents in dental environment are not
rare. Such incidents may occur during
dental treatment, as in case of swallowing an onlay when a patient attempted to
speak during the dental procedure (6); or a screwdriver
during oral implant treatment (7); or a gold cast crown
during orthodontic tooth separation (8); or a reamer during
endodontic therapy (9).
In order to prevent such occurrence, different measures have been
proposed such as using barriers (rubber dam, throat packs) and ligation of
objects to be used intra-orally if they carry some risk of ingestion. Swallowing of dental objects may also occur
away of the clinic. Impaction or
ingestion of removable prosthesis is not rare particularly uni-lateral ones (9)
or those replacing a single upper anterior tooth (10). The possibility of accidental ingestion
should be added to the factors considered when deciding whether a fixed or
removable replacement of anterior teeth is indicated. Bridges are a more secure mean for such
replacement than partial dentures.
However, fixed prosthesis
may also be
ingested if inadequately retained (11). This clinical report describes an accidental
swallowing of a four-unit-anterior bridge that pass the alimentary tract
without any complications and re-cemented in its place.
Clinical
Report
A 24-year-old
healthy female patient missed her appointment for final cementation of four
units porcelain fused to metal anterior bridge.
One month later she phoned the clinic to report the loss of the
bridge. She was not sure if she had
swallowed the bridge, but she noticed that the bridge was lost after eating a
big chunk of ice cream and experiencing a transient difficulty in
swallowing. The patient returned to the
clinic primarily due to esthetic concern (Fig. 1). She had no symptoms, but worried about the
possibility that she accidentally had swallowed the bridge. A temporary bridge was cemented and a plain
abdominal X-ray was taken. The presence
of the bridge in the lower abdomen was confirmed (Fig. 2). The general surgeon and the radiologist were
consulted and they suggested that the bridge might be excreted without any intervention. The patient was asked to observe her bowel
motions regularly looking for the bridge. The bridge was recovered in two
days. After being disinfected in 2%
glutaraldehyde overnight, the bridge was glazed, sandblasted, and re-cemented
temporary for one week (Fig. 3), and permanently one week later.
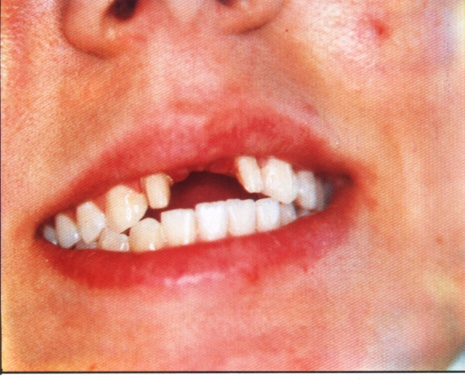
Fig. 1. The esthetic
concern of the patient as a result of the lost bridge. Noticing the prepared
laterals and the limited pontic space.
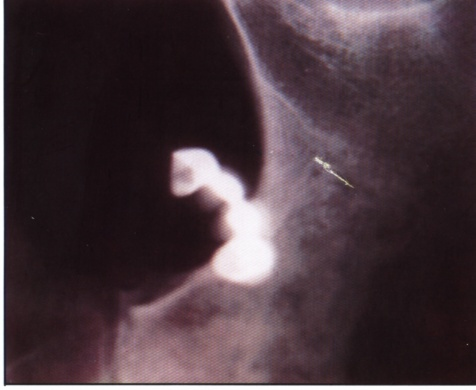
Fig. 2. The abdominal
X-ray shows the swallowed bridge at the lower end of the large intestine.

Fig. 3. The bridge in
place after permanent cementation.
Discussion
In the present
case, the design of the bridge was governed by the limited space available for
the two centrals and the size and inclination of the lateral incisors. According to Ante’s law (12),
it is contra-indicated to replace the upper central incisors using upper
laterals as the only abutments since their root surface area is less than that
of the centrals. The patient refused to
include the canines in the bridge. The
laterals were periodontally healthy and their crown-root ratio was close to the
ideal (1:2). The possible presence of a
premature contact of the bridge (which was confirmed during final cementation)
might caused breakdown of the temporary cement and led to its looseness since
articulating papers will not apparently indicate occlusal premature contacts on
glazed porcelain. The use of more adhesive temporary cement might have been
better in this case.
In general, ingested foreign bodies can be managed
by conservative approach (close observation), endoscopy, or surgery. Sharp
object (eg. dental bridges) ingestions may require different management from
other foreign body ingestions because of possible gastrointestinal tract perforation
(5). Cases of symptomatic foreign body ingestion are usually
presented in emergency department.
History, physical examination, and various radiographs are essential for
the emergency physician to confirm the diagnosis, identify the object’s
composition and shape and to determine its appropriate location in the tissues (13). Once the object is discovered, the clinician
must weigh the potential harm of the foreign body in its current location
against the risk of attempting removal.
Many studies
concluded that asymptomatic gastric and intestinal foreign bodies could be
managed with outpatient daily observation until the foreign body spontaneously
appeared in the feces (5,14).
Patients with prior gastrointestinal surgery or congenital gut
malformation are at increased risk for perforation or obstruction (4). In our case, the management decision was the
conservative approach because the patient was medically fit, the bridge was in
the lower abdomen, the condition was asymptomatic, and the only concern of the
patient was the esthetics.
Conclusion
Since foreign body ingestion may result in acute
medical or life-threatening emergency, prevention of such occurrence is
therefore the best approach. Knowledge
by the dental team of the signs and symptoms of a swallowed object,
documentation and proper medical follow-up are all essential for better
management of ingested objects. A
patient with a dental prosthesis should be informed of this potential risk of
swallowing. Fixed prosthesis should be
checked carefully for retention and premature occlusal contact before glazing
and temporary cementation. Finally such
prosthesis should be permanently cemented as soon as possible.
References
1. Webb WA. Management of
foreign bodies of the upper gastrointestinal tract. Gastroenterology
1988; 94:204-216.
2.Cooke LD, Baxter PW. Accidental
impaction of partial denture prosthesis in the upper gastrointestinal tract. Br
Dent J 1992; 172:457-452.
3. Hodges ED, Durham TM, Stanley RT. Management of
aspiration and swallowing incidents: A review of the literature and report of a
case. ASDC J Dent Child 1992; 59:
413-419.
4. Henderson
CT, Engel J, Schlesinger P. Foreign body
ingestion: Review and suggested guidelines for management. Endoscopy
1987; 19: 68-71.
5. American Society for Gastrointestinal
Endoscopy. Guideline for the management of ingested foreign bodies. Gastrointest
Endosc 1995; 42(6): 622-625.
6. Nelson JF. Ingesting an
onlay. A case report. J Am Dent Assoc 1992; 123: 73-74.
7. Worthington P. Ingested
foreign body associated with oral implant treatment: Report of a case. Int J
Oral Maxillofac Implants 1996; 11: 679-681.
8.Kharbanda OP, Varshney P, Dutta U. Accidental
swallowing of a
gold cast crown
during orthodontic tooth separation.
J Clin Pediatr Dent 1995; 19: 289-292.
9. Vinden GD. Swallowed
dental reamer. Br Med J 1968; 1(594): 769.
10. Rizzatti-Barbosa CM, Cunha FL,
Bianchini WA, et al. Accidental impaction of a unilateral
removable partial denture: A clinical report. J Prosth Dent 1999; 82:
270-271.
11. Beaumont RH. Retrieval of a
swallowed casting 6 weeks after ingestion. A case report. Oral Surg Oral Med
Oral Pathol 1987; 64(3): 287-288.
12. Ante IH. The fundamental
principles of abutments. Mitch
State Dent Soc Bul 1926;
8: 14-23.
13. Lammers RL, Magill T. Detection and
management of foreign bodies in soft tisses. Emerg Med Clin North Am
1992; 10(4): 767-781.
14. Clarkston WK.
Gastrointestinal foreign bodies. When to remove them, when to watch and wait.
Postgrad Med 1992; 92: 51-59.