ABSTRACT
Objective: Multilocular
cystic renal cell carcinoma appears to be uncommon subtype of renal cell
carcinoma with characteristic gross and microscopic features. This study
reports the presentation, diagnosis, and treatment of multilocular cystic renal
cell carcinoma, which is a rare entity and its true incidence and biologic
behavior are not well known in Jordan.
Methods:
We have identified two cases of multilocular
cystic renal cell carcinoma at Queen Rania
Urology Center
over the last three years. The clinical, radiological, and pathological
features were described and the surgical procedure and follow up outcome were
studied.
Results: The tumor was
an incidental finding in both cases. Ultrasound and computerized tomography
(CT) scans were performed prior to surgery but could not identify the
tumor. Nephrectomy was performed in both
cases. Tumor size was 5 cm in one case and 7 centimeters (cm) in the second.
Both cases were followed until the present time and last ultrasound and CT scan
proved to be negative for recurrence.
Conclusion:
Multilocular cystic renal cell carcinoma is
uncommon subtype of renal cell carcinoma, and it has a benign clinical course.
Nephrectomy is a curative procedure and there is no need for any other adjuvant
therapy.The Multilocular renal cell carcinoma must be distinguished from renal
cell carcinoma with cystic degeneration and multilocular cystic nephroma.
Key words: Multilocular cystic, renal tumors, nephrectomy.
JRMS
Dec 2004; 11(2): 47-51
Introduction
Multilocular cystic renal cell carcinoma (MCRCC) is a recently described variety of renal cell carcinoma with
characteristic pathologic and clinical features. It presents a diagnostic challenge
because they are malignant tumors with a benign course (1). MCRCC has characteristic histological
findings. It is a rare variant of
classic renal cell carcinoma, which carries an excellent prognosis and is
usually curative by surgery alone (2). In long-term studies, none of the MCRCC kidney
tumors showed a malignant behavior. If this type of renal neoplasm can be
identified preoperatively and confirmed intraoperatively, it can be managed by
more conservative surgery (3,4).
We present two cases in which the
preoperative differential diagnosis between benign hydatid cyst and malignant
mass was difficult.
Methods
Two cases
of MCRCC were
diagnosed at Queen
Rania Urology
Center over the last
three years. For these cases the clinical, radiological features, gross
appearance, pathological stage, and surgical procedures will be evaluated.
First Case
A 33-year-old lady, with no
previous medical or surgical illness, presented with chronic right loin pain.
Ultrasound and computerized tomographic scan reported a 7 x 9.5 cm septated
multiloculated cystic lesion containing flecks of calcification arising from
the upper pole of right kidney. There was some extension into the medial and
anterior perinephric space; which is most probably consistent with hydatid
disease of the right kidney. No lymph node enlargement was seen.
The patient was admitted on June 26th, 2002, and
exploration of the right kidney was performed via right subcostal incision the
following day.
Findings were a multicystic mass occupying the upper
pole of the right kidney with enlarged hilar lymph nodes. A frozen section was
performed and it revealed the presence of a cystic renal cell carcinoma. Right
nephrectomy and dissection of lymph nodes was performed and the patient was
discharged in good health on the
first of July 2002.
The histopathological report of the
whole specimen showed a multiloculated cystic tumor composed of variable sized
spaces lined by clear epithelial cells. The septa between the cysts contained
scattered islands of a nuclear grade I clear cell carcinoma. There was no extra
renal capsular spread and no invasion of the pelvis or renal vessels. All lymph
nodes were reactive. The appearance was in keeping with a multilocular cystic
variant of clear cell carcinoma of the kidney and in summary a multilocular
cystic renal cell carcinoma was completely excised. Tumor lymph node & metastasis (TNM) stage
T1N0Mx.
Follow up chest and abdomen CT scan
five months later was free of local recurrence and metastases. The left kidney
was normal, and no lymph node enlargement was detected.
Second Case
A
forty-five-year-old lady, with a history of lung tuberculosis that was treated
with partial left pneumonectomy, presented with long standing left loin pain
and chronic urinary tract infection. She was investigated as an outpatient and
found to have a left renal cystic mass about 2.7 cm in diameter. A CT scan was
performed which showed a septated cystic mass lesion arising from the posterior
aspect of the lower pole of the left kidney measuring 4 cm in diameter. The
lesion invaded the medulla and cortex and protruded beyond the renal outlines.
The appearance was that of a cystic tumor, however the possibility of hydatid
cyst could not be ruled out. There was no lymph node enlargement. She was
admitted on December 2000 for operation but she asked to postpone her surgery
and she was admitted again on July
19th 2001. Her case was discussed again and the
provisional diagnosis was hydatid cyst.
She underwent exploration of the kidney on August 8th, 2001
and the surgical finding appeared to be that of a hydatid cyst about 7 cm in
diameter, bulging from lateral surface and lower pole of the kidney. Enucleation of the cyst was performed. The patient was discharged on August 12th 2001.
Two weeks later, the histopathological report revealed an
intact cystic mass measuring 5cm in maximum dimension. The cut surface showed a
well-circumscribed small multilocular cystic mass containing gelatinous
material with a 1.2 cm rim of normal renal tissue.
Microscopically, the
sections showed a well-circumscribed renal tumor with features consistent with
a Grade I multilocular cystic clear cell renal cell carcinoma. The tumor was
completely excised.
The patient was readmitted and left nephrectomy was done on Sept. 9th 2001. Histopathological examination revealed no
evidence of residual or recurrent malignancy. She was discharged two days later
in good health.
Follow up ultrasound and CT scan on Dec. 2002 proved to be
free from recurrence or distant metastasis.
Results
In both cases of MCRCC the clinical and radiological
interpretation as well as surgical management were evaluated. The tumor size,
site, gross appearance, and pathological stage were recorded.
For tumor
staging and histological evaluation, representative sections were taken from
the tumor, its capsule, perinephric fat, and non-tumorous renal parenchyma,
surgical resection margins any lymph nodes were taken into consideration. The
same pathologist reviewed all slides in both cases.
The clinical presentation, treatment, and follow up data
were obtained from the patient charts and directly from the physicians. Stage
was assessed according to 1997 TNM classification, tumor nuclear grade was
evaluated according to the Fuhrman system
Clinical
Features
We identified two cases of MCRCC, both were females, 33 and 47 years of
age, respectively. The tumor was found incidentally and in both cases the
radiological evaluation showed the possibility of hydatid cyst as the most
likely diagnosis.
During surgery one case was diagnosed by frozen section and
nephrectomy was performed at the same session, but in the other case the cyst
was not suspicious, thus no frozen section was taken and the patient underwent
another surgical exploration after the histopathological report came with
diagnosis of MCRCC (Fig. 1,2).
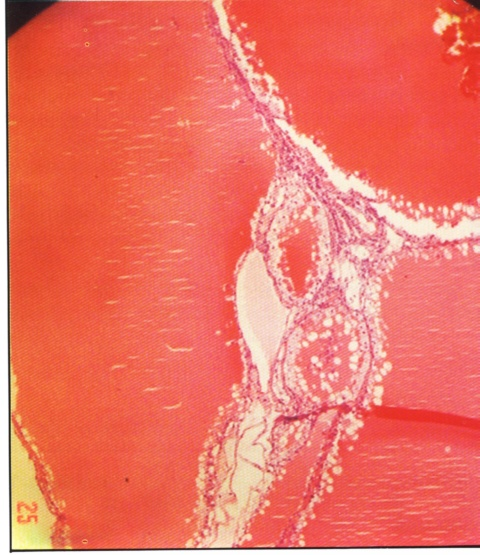
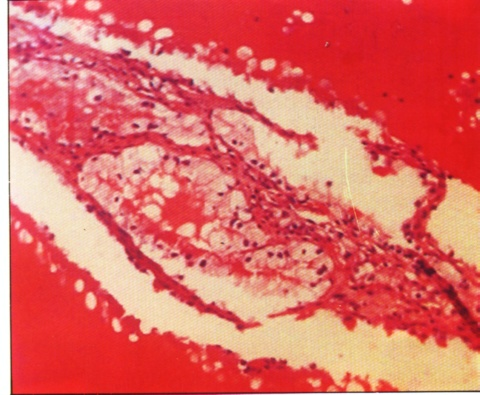
Fig. 1& 2. Histopathological diagnosis of MCRCC.
Imaging Studies
Renal ultrasound was performed in both cases, and
demonstrated cystic lesions. Renal computerized tomographic scans were then
arranged. In the first case a 7 x 9.5 cm septated multiloculated
cystic lesion containing flecks of calcification arising from the upper pole of
right kidney with some extension into the medial and anterior perinephric space
was reported (Fig. 3) consistent with hydatid disease of the right kidney. In the second case the renal CT scan showed a septated
cystic mass lesion arising from the posterior aspect of the lower pole of the
left kidney measuring 4cm in diameter (Fig. 4). The lesion invaded the medulla
and cortex and protruded beyond the renal outline. The appearance was concluded
to be due to a cystic tumor, however the possibility of hydatid cyst could not
be ruled out.
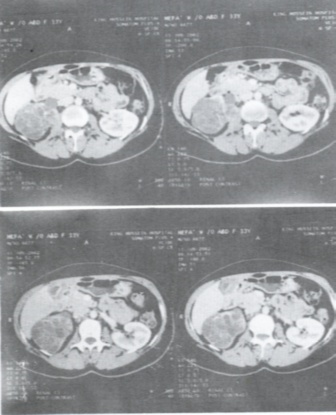
Fig. 3. CT scan in case 1- showing the
lesion.
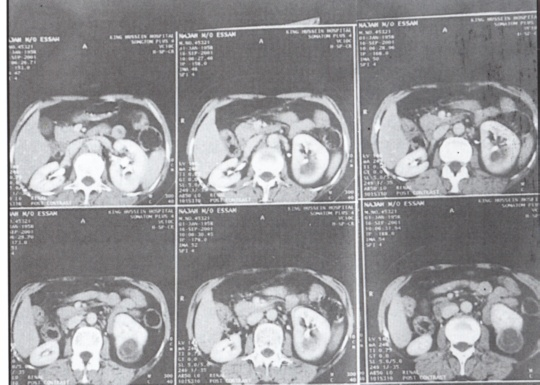
Fig. 4. CT scan
findings in case 2.
Discussion
Although description of multilocular
renal cysts date back to 1892 (5), the presence of small
clear cell population within their
wall was not
reported until 1928 (6),
the diagnosis of lymphangioma was entertained, but this was not supported in
later studies. The second case showing the presence of epithelial clear cells
lining the cystic spaces was reported in 1957 (7), these two
case reports appear to be the first descriptions of what today is classified as
MCRCC. Several earlier studies had reported MCRCC as Renal Cell Carcinoma (RCC)
arising in multilocular cystic nephroma. In 1982 (8) the term
multilocular cystic renal cell carcinoma was introduced and MCRCC became
accepted as a distinct entity.
Nowadays, many cases of MCRCC have
been reported worldwide.
MCRCC is rare having a reported
incidence between 1-4% of RCC. Because the etiology of RCC is not well
established it would be difficult to elucidate the etiology of the MCRCC
subtypes. More cases have been reported in
Japan
compared with the rest of the world; suggesting the importance of environmental
and/or genetic factors. Conversely, this may be a result of greater awareness
and reporting of MCRCC in Japan.
Genetic susceptibility probably plays an important role, MCRCC has been
associated with simultaneous primary tumors of other sites (endometrium),
Corica et al (9) found that 83% of MCRCC cases were
diagnosed incidentally. Tosaka et al (10) recognized
that asthenia, anorexia, and weight loss were significantly higher in patients
with non-cystic RCC compared with those with cystic RCC. Moreover, Fujii et al (11)
found that all their patients with solid RCC were symptomatic, and there with
solid RCC were not. Also MCRCC may be discovered incidentally while imaging the
abdomen for unrelated conditions than for tumor related symptoms. In both of the cases reported in this paper loin pain
was the presenting
symptoms.
Published reports suggested that
ultrasonography and CT scan are the most practical tools for investigating and
detecting MCRCC. Ultrasonography may only reveal septated cyst and may
downgrade higher Bosniak category (12). Adding color Doppler
may prove useful. CT scan is diagnostically more accurate and will demonstrate
malignant features such as contrast enhancement and increased attenuation; even
so, CT scan may not be able to differentiate MCRCC from necrotic RCC. Yamashita
et al (13) found MRI superior to CT scans for such
differentiation. Conversely, Eble (14)
and Bonsib (12) suggested that MCRCC should have no
expansible nodules in the septa rather than stipulating a percentage of solid
components.
Although the pathologic diagnosis of
MCRCC seems to be straight forward, controversy regarding the diagnostic
criteria continues. Murad et al (15) suggested 10% as
the maximal percentage of solid tumor components. Later, Corica et al (9)
expanded the definition to include lesions with a solid component occupying up
to 25% of the total tumor size. Murad et
al (15) suggested that Furhman nuclear grade I was a
defining criterion for MCRCC and in fact we favor this criterion and we used
it.
Because the term cystic renal cell
carcinoma CRCC refers to several lesions with differing histopathological
features and prognosis, it should be avoided unless clarified. CRCC can refer
to both necrotic RCC and MCRCC. Cystic degeneration can be either from tumor
regression or rapid growth. The later typically reflects an aggressive tumor
that may have a very different prognosis from that of MCRCC. Failure to
distinguish between cystic renal cell carcinoma as a general term and MCRCC can
limit the prognostic usefulness of this category. Also
bilateral cases of
MCRCC were reported (18).
Without sub categorization,
Gutierrez Banos et al (17) failed to show any
significant survival differences. Tosaka et al (10)
ascertained the outcome of 38 patients with MCRCC. Their 10-years survival rate
and non-recurrence rate was 97.3% and 90.3%, respectively.
In summary, MCRCC is a predominantly
cystic lesion with a small solid component
(25% or less). It is probably a subtype of conventional clear cell renal
cell carcinoma that because of its relatively low epithelial tumor volume has a
lower malignant potential.
We recommend using the term
multilocular cystic renal cell carcinoma (MCRCC) exclusively to identify a
cystic lesion with a small volume of neoplastic clear cells in the wall of the
cysts or within their septa. It is an uncommon histological subtype (3%) of
conventional (clear cell) RCC usually cured by resection. The benign clinical
course of these lesions suggests that patients may benefit from nephron-sparing
surgery, such as partial nephrectomy (18). In hand right, it was probably sufficient for
the second case to have been managed in this way thus avoiding nephrectomy.
Review of the published literature on MCRCC would support this approach. It was
not possible preoperatively to confidently diagnose MCRCC in either cases and a
high index of suspicious is necessary to concede this diagnosis given the
radiological findings so that more conservative surgery can be planned.
References
1. Kogo S,
Nishikido M, Hayashi T, et al. Outcome
of surgery in renal cell carcinoma. Urology 2000; 56(1): 67-70.
2. Nassir A, Jollimore J, Gupta R, et al. Multilocular cystic renal cell carcinoma: A
series of 12 cases and review of the literature. Urology 2002; 60(3):
421-427.
3. Weiss SG, Hafez RG, Uehling DT. Multilocular renal cell carcinoma:
Implications for nephron sparing surgery. Urology 1998; 51(4): 635-637.
4. Tsujihata M, Tsuboniwa N, Miyake O, et
al. Multilocular cystic renal cell carcinoma treated with tumor
enucleation: A case report. Hinyokika Kiyo 1995; 41: 541-543.[ Medline
].
5. Edmunds W. Cystic adenoma
of the kidney. Trans Path Soc Lond 1892; 43: 89-90.
6. Perlmann S. Ubereinen Fall
von Lymphangioma cysticum der Niere. Virchow Arch Pathol Anat Physiol Klin
Med 1928; 268: 524-535.
7. Robinson GL. Perlmann's
tumor of the kidney. Br J Surg 1957; 44: 620-623. [Medline].
8. Lewis RH, Clark MA, Dobson CL, et al. Multilocular
cystic renal adenocarcinoma arising in a solitary kidney. J Urol 1982;
127: 314-316. [Medline].
9. Corica FA, Iczkowski KA, Cheng L, et
al. Cystic renal cell carcinoma is cured by resection: A study
of 24 cases with long-term follow up. J Urol 1999; 161: 408-411.
10. Tosaka A, Yoshida K, Kobayashi N, et
al. A report of two cases of multilocular cystic renal cell
carcinoma: Review of 51 cases reported and the results of a prognostic survey. Hinyokika
Kiyo 1992; 38: 1045-1050.
11. Fujii Y, Ajima J, Tosaka A, et al. Asymptomatic
multilocular cystic renal cell carcinoma. Nippon
Hinyokika Gakkai Zasshi 1992; 83: 1270-1275.
12. Bosniak M. The use of the
Bosniak classification system for renal cysts and cystic tumors. J Urol
1997; 157: 1852-1853.
13. Yamashita Y, Miyazaki T, Ishii A, et
al. Multilocular cystic renal cell carcinoma presenting as a
solid mass: Radiologic evaluation. Abdom Imaging 1995; 20: 164-168.
14. Eble J.N. and Bonsib S.M. Extensively
cystic renal neoplasms: Cystic nephroma, cystic partially differentiated
nephroblastoma, multilocular cystic renal cell carcinoma, and cystic hamartoma
of renal pelvis. Semin Diagn Pathol 1998; 15: 2-20.
15. Murad T,Komaiko W,Oyasu R and Bauer K. Multiloclar
cystic renal cell carcinoma. Am J Clin Pathol 1991; 95: 633-637.
[Medline].
16. Yamamoto H, Maruyama T, Kuwae H, et
al. Bilateral multilocular cystic renal cell carcinoma: A case
report. Hinyokika Kiyo 1996; 42: 513-516 [Medline].
17. Gutierrez Banos JL, Martin Garcia B,
Hernandez Rodriguez R, et al. Cystic adenocarcinoma of the
kidney: Apropos of
18 cases. Arch Esp Urol
1996; 49: 573-579 [Medline].
18. Corica FA, Iczkowski KA, Cheng L, et
al. Cystic renal cell carcinoma is cured by resection: A study
of 24 cases with long-term follow up. J of Urol 1999; 161: 408–411.