Abstract
Objective: Pilonidal sinus is a common disease in young adults
that carries high postoperative morbidity and patients’ discomfort. The aim of
our study was to present our experience with the Dufourmentel
flap technique in the management of pilonidal sinus disease and to evaluate the
morbidity and recurrence.
Methods: This study was conducted in the surgical department
of Prince Hashem Bin Al-Hussein Hospital in Zarqa between October 2006 and July
2008. Eleven patients were included, eight had previous surgical drainage of
multiple natal cleft abscesses, and three had acute disease at the time of
surgery. Nine patients had complex, recurrent pilonidal sinus. By using the Dufourmentel transposition flap, we were able to
excise the diseased area and close the defect. Operative time, hospital stay,
healing time, wound infection, wound breakdown, return to normal activity and
recurrence were assessed.
Results: There were 10 males and one female with a median age
of 23 years (range 17–32 years). Mean follow-up was 13.5 months (range 1–21
months). Mean operative time was 63.2 minutes (range 55-75 minutes). Hospital stay was 3.4 days (range 2-5). Postoperative morbidity involved superficial
wound infection in two patients, superficial gangrene of wound edges in one
patient and partial wound breakdown in one patient that settled with dressing
in the out-patient clinic. All wounds healed and
the median healing time was 15 days. There was no recurrence in our series.
Median time to return to normal activity was 17.8 (range 10-27) days.
Conclusion: Dufourmentel flap is a useful technique in the
treatment of advanced, difficult cases of pilonidal sinus disease. It has
relatively low morbidity, allows early return to full activity and does not
necessitate prolonged postoperative care. A larger series and longer follow up
time is needed to assess the recurrence rate more adequately.
Key words: Dufourmentel flap technique, Pilonidal sinus disease
JRMS
December 2010; 17(4): 35-40
Introduction
Pilonidal sinus
disease is a painful and chronic condition affecting males predominantly and
can lead to considerable discomfort and morbidity. It occurs in the
intergluteal region and is the result of shed hair shafts through the skin,
which ultimately leads to an acute or chronic infected site.(1)
In 1833, Mayo was the
first to report a hair-containing sinus and Hodges in 1880 suggested the term
pilonidal sinus (Latin: pilus = hair and nidus = nest), to
indicate a disease consisting of hair-containing sinus in the sacrococcygeal
area.(2) Buie(3)
described the condition as jeep disease, because it is believed that it
is caused by long periods of sitting in vehicles.
In 20% of cases, the disease is observed as an acute abscess, whereas in
the remaining cases it presents as a chronic sinus, in which there are draining
orifices.(4,5) Surgical
drainage of pilonidal abscess can be used occasionally as a definitive treatment of small pilonidal sinus with
abscess formation. However, advanced
disease with multiple pilonidal sinus openings, branching tracts, and overt
symptoms may require wide excision of the diseased region. The closure of the
defect can be either by simple approximation of the edges or by using flaps.(6)
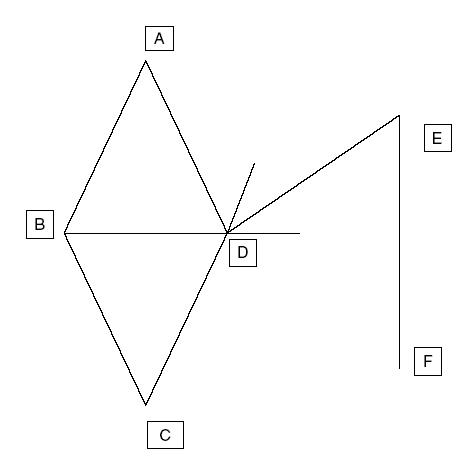
Fig. 1. The
Dufourmentel flap diagram

Fig. 2.
The Rhomboid flap

Fig. 3. Flap
marked on the skin and wide excision of the sinuses
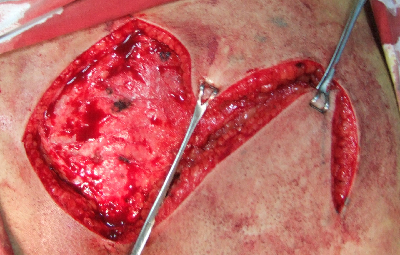
Fig. 4. Flap
being mobilized.
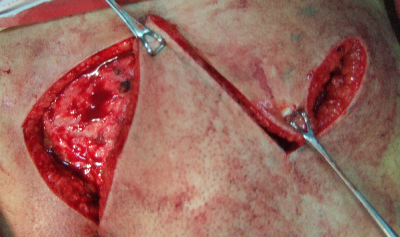
Fig. 5.
Flaps transported to flatten the natal cleft

Fig. 6. Completed
flap with a suction drain
A simple excision and open wound healing cause more
patient discomfort, longer hospitalization, require more time off work and
requires regular outpatient dressing, whereas primary wound closure is
associated with wound related complications, such as failure of primary wound
healing and late pilonidal recurrence. Thus, a large variety of flap techniques
for covering the wound cavity were introduced.(4,6–8)
In this study we
present our experience with one type of flap techniques for closure of the
defect after excision of the pilonidal sinus, i.e. Dufourmentel flap closure.
Methods
This study was
conducted in the surgical department of Prince Hashem
Hospital between October
2006 and July 2008. Eleven patients underwent the procedure. None of them had a
sedentary life. Eight patients had previous multiple abscess formation
requiring surgical drainage from their pilonidal disease and three had acute
disease with pus discharge at the time of surgery. Nine patients had complex,
recurrent pilonidal sinus. The procedure was explained to all patients and an
informed consent obtained.
Preparation
All patients were
admitted to the hospital one day before operation. All were operated on under general
anaesthesia. A single dose of Cephalexin 1g was administered on induction of
anaesthesia for prophylaxis against wound infection for all patients. Patients
were placed in the prone position, with buttocks strapped apart using adhesive
bands. The sacrococcygeal area was shaved and cleaned using povidine-iodine.
The extent of the sinuses was determined by inspection and palpation and all
diseased areas were included in the incision.
Surgical procedure
The area to be excised
(ABCD) is marked on the skin (Fig. 1) with the axis AC being along the natal
cleft, with the anus below C. Lines CD and BD are then extended and the angle
thus formed is bisected by lines having the same length as any one side of the
rhomboid (thus AB =BC =CD =AD =DE). Line EF is then drawn parallel to the long
axis, AC. The sinus (Fig. 2, 3) is excised down to the sacrococcygeal fascia
centrally and the gluteal fascia laterally, and haemostasis is secured using
diathermy. The rhomboid flap (Fig. 4,5) is mobilized from the gluteal fascia
and sutured without tension, with interrupted mattress sutures over a suction
drain (Fig. 6). When there was an abscess, it was included with all diseased
skin in the excised rhomboid.
Aftercare
After the operation, 500mg of Paracetamol and 50mg of
Diclofenac Sodium were administered as soon as oral feeding was resumed for
postoperative pain management for three days postoperatively.
Patients were advised
to lie on the lateral side until the wound healed. The dressing was changed on
the second postoperative day, the drain is removed and the patients are usually
discharged on the fourth day. The patients were advised on the importance of
regular shaving of the buttocks and hygienic measures. The sutures were removed
on the tenth postoperative day.
Patients were followed up weekly for the first six
weeks postoperatively, then monthly thereafter. During each follow up session,
bleeding, haematoma formation, infection, state of healing and recurrence were
evaluated.
Results
There were 10 males
and one female with a mean age of 23 years (range 17–32 years). Clinical
presentation included: local swelling (8 cases), pilonidal abscess (3 cases),
and multiple sinuses with chronic suppurative discharge (9 cases) (see Table I).
Mean operative time
was 63.2 minutes (range 55-75 minutes). The duration of hospital stay was two
to five days (mean 3.4 days). Primary
healing occurred in nine patients when reviewed at the time of suture removal
on the twelfth day. One patient developed partial wound breakdown and one patient
developed superficial gangrene of the wound edges, both were treated with
dressings at the out-patient clinic.
Postoperative
complications were superficial wound infection in two patients, which needed
daily dressing. All wounds
healed, and the mean healing
time was 15 days,
range (12-21 days). None of the patients developed flap necrosis. Mean time to
return to normal activity was 17.8 (range 10-27) days. Mean time off work was
21.4 days. Mean follow-up time was 13.5 months (range 1–21 months).
Discussion
Pilonidal sinus
disease occurs in the sacrococcygeal region. Hirsuteness, moderate
obesity, puberty, vacuum effect and deep
intergluteal sulcus are all factors that contribute to the development of the
disease.(1,9,10) The incidence rate of pilonidal
disease is approximately 700 per 100,000. The disease is found
predominantly in whites; it is rare in blacks and practically nonexistent in
Asians. It is now known that the pilonidal cyst is an acquired chronic disease
of foreign body type caused by penetration of short, stiff hairs into the
subcutaneous tissues.(2)
Pilonidal sinus predominantly affects patients in
their twenties and thirties and males more than females. In our
series, age distribution was similar to that reported in the literature,(7,11,12)
but with male predominance. Male
to female ratio was 10 : 1 while some authors reported a male to female
ratio of 1 : 2.(13)
In this study, location of the pilonidal disease was
in the natal cleft, nevertheless different locations for this condition have
been described, including penis, axilla, perineal and suprapubic area,
periumbilical zone, between the fingers of the hand (Barber's disease), and
even in the ends of amputated extremities.(14,15)
In
spite of high incidence of pilonidal disease affecting young population and the
prolonged disabling period caused by it, surgeons have not reached unanimity
about the best treatment for this condition. Low recurrence rate, minimal
inpatient stay, minimal cost, minimal operation time, minimal inconvenience,
and minimal time off work are important considerations. Nonsurgical and
surgical techniques were proposed.
Nonsurgical techniques have included: local hygiene and weekly shaving of the sacrococcygeal area,(16) laser epilation of the intergluteal hair(17) and phenolization of the sinus tracts, but the later carries considerable risk of chemical burn and seroma formation.(18)
Several surgical techniques
have been described to date: cutting seton,(19) cryosurgery,(20)
aspiration followed by
treatment with antibiotics, drainage
with or without curettage,(9) excision and primary closure,(21,22)
or excision and marsupialization,(23) vacuum assisted closure,(24) sinus excision and delayed closure.(25) Bascom et al.(26) reported that the most common cause of
failure of healing after surgery is the deep cleft, moist and rolling action of the buttocks. Flattening the natal cleft was proposed to prevent the macerating action induced by rolling the buttocks while walking. Hence techniques which involved the obliteration of the deep natal cleft, such as Z-plasty(4) V-Y advancement flap,(27) rhomboid flaps(9,13,28) and primary skin grafting,(29) have been developed.Among these procedures, our treatment of choice is the Dufourmentel rhomboid flap. We believe it is a very good plastic procedure for the treatment of pilonidal sinus however we try to use this technique only in cases of pilonidal sinus with multiple previous failed operations and when there is a large area which needs to be excised.
Table I. Clinical manifestations
|
Clinical
manifestation
|
Patients
|
Frequency (%)
|
|
Local
swelling
|
8
|
73
|
|
Acute
abscess
|
3
|
27
|
|
Chronic
suppurative discharge
|
9
|
81
|
Table
II. Summary of results of different
therapeutic procedures
|
Technique
|
Hospital stay (days)
|
Healing time (days)
|
Infection rate
|
Recurrence (%)
|
|
Phenol application(18)
|
0
|
--
|
--
|
8.3
|
|
Radiofrequency incision(25)
|
<1
|
42-75
|
0
|
0
|
|
Rhomboid flap(28)
|
3-10
|
14
|
0
|
7
|
|
Excision and
marsupialization(23)
|
1.3
|
44.4
|
--
|
10
|
|
Excision and primary closure(35)
|
< 1
|
12
|
2
|
6.3
|
|
Limberg flap(6,9,33)
|
5.6
|
---
|
0-23
|
4.7
|
|
V-Y flap(27,36)
|
3-5
|
---
|
0
|
0-5.9
|
|
Dufourmentel technique(13)
|
4
|
14
|
0
|
0
|
|
Present series
|
3.4
|
15
|
2
|
0
|
A comparison of our
results regarding hospital stay, healing time, infection rate and recurrence is
similar to those reported in the literature (see Table II). Galala et al.(30)
compared the rhomboid flap and the deep suturing techniques and showed
higher healing rates and lower recurrence rate for the former. Our rates of
healing and superficial wound infections are comparable to their findings.
There is a high
recurrence rate in most published series irrespective of the procedure. Edwards(31)
has reported a 46% recurrence rate for excision and healing by secondary
intention and a 38% recurrence rate is quoted for excision and primary closure.
Others(32) reported even higher recurrence rates for those
two techniques, whereas Manterola et al.(13) in a study on 25 cases that were treated by
Dufourmentel flap technique, reported zero recurrence rate after a mean of 3.4
years of follow-up. Other studies(6,33,34) give a
recurrence rate in the range of 2.5-4.8% for different periods of follow-up. We
had no recurrence of the pilonidal sinus disease, but a longer follow up time
will show the true results of this procedure.
The reported average
time lost from work was some 13 weeks of which 6–7 weeks were spent recovering
from an operation designed to cure the condition.(28) In our
study, the median time to return to normal activity was 17.8 days and off work
time was 21.4 days. This is
another advantage of this procedure, keeping in mind that more than 90% of our
patients are military personnel.
Conclusion
Dufourmentel flap is a
technique used for the treatment of advanced, difficult cases of pilonidal sinus
disease. The method is easy to use, has relatively low rate of wound infection,
requires short wound healing time, does not need prolonged postoperative
dressings, and allows early return to normal activities.
A larger series and
longer follow up is needed to give the true picture about the recurrence rates
of pilonidal sinus following this
procedure.
References
1. Bascom J.
Pilonidal Sinus. Curr Ther Colon Rectal Surg 1990; 1-8.
2. da Silva J. Pilonidal cyst:
cause and treatment. Dis Colon Rectum 2000; 43: 1146–1156.
3. Buie L. Jeep disease,
pilonidal disease of mechanized warfare. South
Med J. 1944; 37: 103-109.
4. Fazeli M, Adel
M, Lebaschi A. Comparison of
outcomes in Z-plasty and delayed healing by secondary intention of the
wound after excision of the sacral pilonidal sinus: results of a randomized,
clinical trial. Dis Colon Rectum 2006; 49: 1831-1836.
5. Petersen S, Koch R, Stelzner S, et al. Primary closure
techniques in chronic pilonidal sinus. A survey of the results of different
surgical approaches. Dis Colon Rectum 2002; 45: 1458-1467.
6. Kapan
M, Kapan S, Pekmezci S, et
al. Sacrococcygeal pilonidal sinus disease with Limberg
flap repair. Tech Coloproctol 2002;
6: 27–32.
7. Arumugam P, Chandrasekaran T,
Morgan A, et
al. The rhomboid flap for pilonidal
disease. Colorectal Dis 2003; 5:
218–221.
8. Mahdy T. Surgical treatment of the pilonidal disease: primary closure or flap reconstruction after excision. Dis Colon Rectum. 2008; 51: 1816-1822.
9. Cihan A, Ucan B, Comert M, et al. Superiority of asymmetric
modified limberg flap for surgical treatment of pilonidal disease. Dis Colon
Rectum 2006; 49: 244-249.
10. Chintapatla S, Safarani N, Kumar S. Sacrococcygeal pilonidal sinus: historical review, pathological insight
and surgical options. Tech Coloproctol
2003; 7: 3-8.
11. Branagan G, Thompson M, Senapati A. Cleft closure for the
treatment of unhealed perineal sinus. Colorectal
Dis 2006, 8, 314–317.
12. Cripps N, Evans J, Nordon I, et al. Sacrococcygeal pilonidal sinus disease. Colorectal Dis. 2009; 11: 105-106.
13. Manterola C, Barroso M, Araya J, et al. Pilonidal disease: 25
cases treated by the Dufourmentel technique. Dis Colon
Rectum 1991; 34: 649-652.
14. Jeffery M, Billingham N, Billingham R. Pilonidal Disease and Hidradenitis Suppurativa. In: Wolff B, Fleshman
J, Beck D, et al editors. The ASCRS Textbook of Colon and Rectal Surgery. 1st ed. New York: Springer 2007.
p. 228-239.
15. Efthimiadis C, Kosmidis C, Anthimidis G, et al. Barber's hair sinus in a female hairdresser: uncommon manifestation of an occupational disease: a case report. Cases J. 2008 6; 1: 214.
16. Golladay E. Outpatient
adolescent surgical problems. Adolesc Med
Clin 2004; 15: 503-520.
17. Lukish J, Kindelan T, Marmon L, et al. Laser epilation is a safe and effective therapy for teenagers with pilonidal disease. J Pediatr Surg. 2009; 44: 282-285.
18. Kaymakcioglu N, Yagci G,
Simsek A, et al. Treatment of pilonidal sinus by phenol application and factors
affecting the recurrence. Tech
Coloproctol 2005; 9: 21–24.
19. Rao A. Cutting seton for pilonidal disease: a
new approach. Tech Coloproctol 2006; 10: 242-244. (abstract)
20. Gage A, Dutta P. Cryosurgery
for pilonidal disease. Am J Surg
1977; 133: 249-254.
21. Aldean I, Shankar P, Mathew J,
et al. Simple excision and primary closure of pilonidal
sinus: a simple modification of conventional technique with excellent results. Colorectal Dis 2005; 7: 81–85.
22. Akinci O, Coskun A, Uzunkoy A. Simple and
Effective Surgical Treatment of
pilonidal sinus, asymmetric excision and primary closure using suction drain
and subcuticular skin closure. Dis
Colon Rectum
2000; 43: 701-707.
23. Oncel M, Kurt N, Kement M. Excision and marsupialization versus sinus excision
for the treatment of limited
chronic pilonidal disease: a prospective, randomized trial. Tech Coloproctol
2002; 6: 165–169.
24. Lynch J, Laing A, Regan P. Vacuum-assisted closure therapy: a new treatment
option for recurrent pilonidal sinus disease. Report of three cases. Dis Colon
Rectum 2004; 47: 929–932.
25. Gupta P. Radiofrequency
Incision and Lay Open Technique of Pilonidal Sinus Clinical Practice Paper on
Modified Technique. Kobe J Med Sci 2003; 49: 75-82.
26. Bascom J, Bascom T. Failed pilonidal surgery: new paradigm and new
operations leading to cure. Arch Surg
2002; 137: 1146-1151.
27. Berkem H, Topaloglu S, Ozel H, et al. V–Y advancement flap closures for complicated pilonidal sinus disease. Int J Colorectal Dis 2005; 20: 343–348.
28. Arumugam P, Chandrasekaran T,
Morgan A, et al. The rhomboid flap for pilonidal disease. Colorectal Disease 2003; 5: 218–221.
29. Guyuron B, Dinner M, Dowden R. Excision and grafting in treatment of recurrent
pilonidal sinus disease. Surg Gynecol
Obstet 1983; 156: 201–204.
30. Galala K, Salam I, Sim A, et al. Treatment of pilonidal sinus by
primary closure with a transposed rhomboid flap compared with deep suturing: a
prospective randomized clinical trial. Eur
J Surg 1999; 165: 468–472.
31. Edwards M. Pilonidal sinus. A
5 year appraisal of the Millar- Lord treatment. Br J Surg 1977; 64: 867–868.
32. Patel H, Lee M, Bloom I, et al. Prolonged delay in healing after surgical
treatment of pilonidal sinus is avoidable. Colorectal
Dis 1999; 1: 107-110.
33. Daphan C, Tekelioglu H, Sayilgan C. Limberg Flap Repair
for Pilonidal Sinus Disease. Dis Colon Rectum 2004;
47: 233–237.
34. Topgul K, O¨ zdemir E, Kilic K,
et al. Long-Term Results of
Limberg Flap Procedure for Treatment of Pilonidal Sinus. A Report of 200 Cases. Dis Colon Rectum 2003; 46:1545–1548.
35. Testini M, Piccinni G, Miniello S, et al. Treatment of chronic
pilonidal sinus with local anaesthesia: a randomized trial of closed
compared with open technique. Colorectal
Dis 2001; 3: 427-430.
36. Khatri V, Espinosa M, Amin A.
Management of recurrent pilonidal sinus by simple V-Y fasciocutaneous flap. Dis Colon
Rectum 1994; 37: 1232-1235.