Abstract
Objectives: Syndactyly is one of the most common
congenital hand deformities. Web space reconstruction is an important component
of syndactyly treatment. Our objective is to evaluate the method of web space
defect closure in syndactyly repair, using a V-Y dorsal metacarpal advancement
flap, without using skin grafts.
Methods: Over the period of six years (May 2003 through
May 2009), a total of 20 patients (24 hands, 25 web spaces) with simple
syndactyly were operated upon using a dorsal metacarpal skin flap based on a
direct coetaneous branch of the dorsal metacarpal artery. This flap was
advanced in a V-Y fashion to aid in web space defect closure, without using
skin grafts. There were 15 males and five females. Four cases had bilateral, three
had right sided and the remaining 13 had left sided syndactyly. Fourteen cases
had complete type and six had incomplete type. The mean age at operation was
4.7 years (range 1-12). The web spaces affected were the thumb-index,
middle-ring, ring-little in one, 18, and six web spaces respectively. The mean
follow up period was 10 months (range 6-35 months).
Results: All
patients had uneventful postoperative period. There was no flap necrosis or
digital vascular compromise. One case showed hypertrophic scarring of the
repair but all patients had acceptable range of motion at follow up.
Conclusion:
Dorsal metacarpal skin flap
advancement is a good way of repairing the web space defect during syndactyly
release, eliminating the need for skin grafts.
Key
wards: Flaps, Syndactyly, without
skin graft
JRMS
December 2010; 17(4): 47-50
Introduction
Syndactyly is one of the most common congenital hand
deficiencies, with an incidence of one per 2,000 to 2,500 live births. There is
a strong familial tendency: 10% to 40% cases are inherited as a result of a
dominant gene with variable penetrance.(1) The objectives of
treatment are both functional and cosmetic. Current techniques of syndactyly
correction utilize a zigzag incision along the full length of the digit to
avoid contracture that might follow a straight line closure, the web space is
reconstructed in most of the techniques by a skin graft,(2-3)
alternative techniques utilize a local skin flap. We demonstrate our experience
in syndactyly treatment using a dorsal metacarpal flap.
Methods
This is a prospective study of 20 patients (24 hands,
25 web spaces) with simple syndactyly carried out in the Royal Rehabilitation
Center at King Hussein Medical Center over a six years period (May 2003 through
May 2009). There were 15 males and five females. Four cases had bilateral,
three had right sided and the remaining 13 had left sided syndactyly. Fourteen
cases had complete type and six had incomplete
type.
The mean age at operation was 4.7 years (range 1-12). The web spaces affected were the thumb-index, middle-ring, ring-little in one, 18, and six web spaces respectively. None of the patients had any other congenital deformity or had a positive family history.
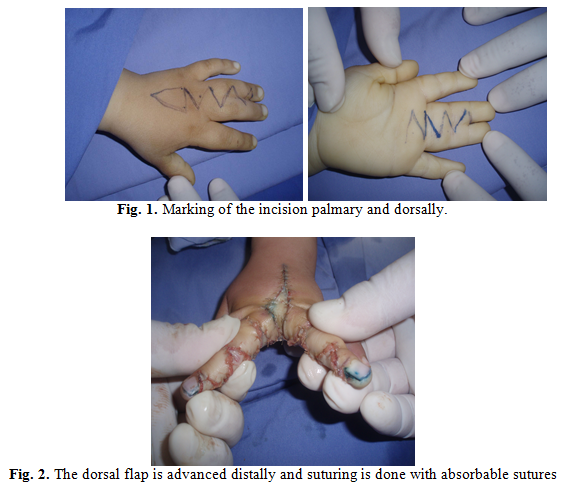
The operation was performed under general anesthesia
with the control of pneumatic tourniquet, marking of the incision was done (Fig
1), and the fingers were separated by the standard zigzag incision. The dorsal
metacarpal flap is designed over the dorsum of the hand at the intermetacarpal
space centered proximal to the metacarpophalangeal joint in a V (triangular)
shape. The length of the flap varies from 1-3cm and its width from 1-2cm,
according to the age of the patient. All dissection was done without complete
exsanguinations to help in the visualization of the neurovascular bundles of
the fingers, excess fat around the neurovascular bundles of the fingers was
excised to help closure of the defect without tension, the dorsal metacarpal flap
was dissected and mobilized without direct visualization of the perforator, the
flap was then advanced distally (Fig 2) and the defect closed directly using
absorbable sutures. A usual hand dressing was done with neomycin permeated
gauze on the suture line and fluffy gauze in between the fingers and a light
pressure bandage. The patients were admitted for one day postoperatively for
observation. The first dressing was done after one week under general
anesthesia.
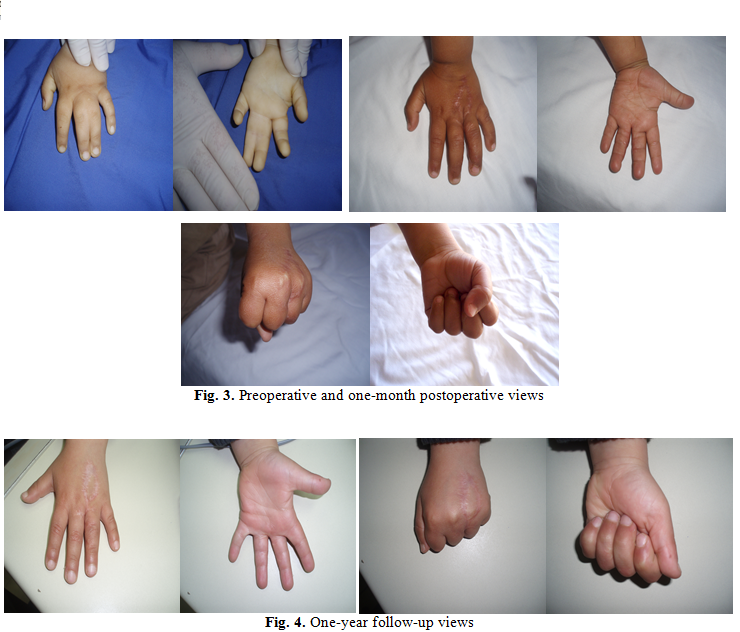
Results
All patients had an uneventful postoperative period.
There was no flap necrosis or digital vascular compromise. One case showed
hypertrophic scarring of the repair but all patients had acceptable range of
motion at follow up. The mean follow up period was 10 months (range 6-35 months).
(Figures 3 and 4)
Discussion
Syndactyly is classified descriptively on the basis of
the degree of skin bridging and according to the presence or absence of bony
fusion.(4) The history of syndactyly surgery dates from early
1800s.(5) The principles of syndactyly reconstruction are
well established: (A) to create both cosmetically acceptable and functionally
independent digits; and (B) to provide a normal web that is well adjusted
to other interdigital webs. The normal web is wider distally than proximally and slopes at a 35o to 45o angle from proximal-dorsal to distal-palmar direction. The base of the web is located at the mid-portion of the proximal phalanx on the lateral view.(6,7)
Several authors advocated that the
operation should be performed within the first years of life, and they consider
that the success of the operation would be reduced due to certain developmental
bone deformities and increased complication rate if the operation was performed
at a later age. It is reported that the average age at the time of surgery was
below four years.(8,9) In our study the average age of
surgery was 4.7 years and yet there was no bone deformity. The reconstruction
of syndactyly using dorsal skin flap and side grafts was the most noteworthy
method of choice,(1,3,10) however, complications like
hyperpigmentation, contracture, hair growth and morbidity of the donor site(9)
necessitate looking for another alternative. In the recent years, there has
been an increase in the surgical treatment techniques which do not need a free
skin graft for complete syndactyly treatment, rather requiring a skin flap. The
dorsal metacarpal V-Y advancement flap is a safe and reliable flap,(5)
utilizing the dorsum hand skin to cover the web area, as the size of the flap
is large enough to cover the web space without applying suture line in the web
area, so web contracture do not occur in these techniques. The new web had the
same skin color and texture of fingers,(11) and the resultant
scars in the web space are usually inconspicuous. The use of this flap instead
of skin graft has markedly shortened the operative time of syndactyly release.
No flap has been lost either from arterial or venous complication. The only
disadvantage for this flap is the presence of scar on the dorsum of the hand, which
tend to settle down well and become barely noticeable six months after the
operation.
Conclusion
Dorsal metacarpal skin flap advancement is a good way
of repairing the web space defect during syndactyly release, eliminating the
need for skin grafts.
References
1. Choi M, Sharma S, Louie O. Congenital hand abnormalities. In: Charles H. Thorne,
editor in chief. Grabb and Smith's Plastic Surgery, Sixth Edition. Philadelphia: Lippincott
Williams & Wilkins 2007. p. 856-863.
2. Bauer TB, Tondra JM, Trusler HM. Techniqal modification in repair of syndactylism. Plast
Reconstr Surg 1956; 17:385-392.
3. Zoltie N, Verlende P, Logan A. Full thickness grafts taken from the plantar instep
for syndactyly release. J Hand Surgery 1989; 14B:201-203.
4. Ezaki M. Congenital hand deformities. Operative Hand Surgery 4th
ed. 1999; 415.
5. Sherif M. V-Y Dorsal metacarpal flap: a new technique for the
correction of syndactyly without skin graft. Plast Reconstr Surg 1998;
101:1861-1866.
6. Tan O, Atik B, Ergen D. Versalite
use of the VM-plasy for reconstruction of the web space. Annals of Plastic
Surgery 2005; 55:623-628.
7. Aydin A, Ozden B. Dorsal metacarpal Island Flap in Syndactayly
Traeatment. Annals of Plastic Surgery 2004; 52:43-48.
8. Percival NJ, Sykes PJ.
Syndactyly: A review of the factors which influence surgical treatment. J Hand
Surgery 1989; 14B:196-200.
9. Ozgur Cetik, Baris K, Faith E,
et al. Contrary intermittent
skin release of complete syndactyly without skin graft in adults. Annals of
Plastic Surgery. 2005; 55:359-362.
10. Deunk J, Nicolai JP, Hamburg SM. Long-Term results of syndactyly correction:
full-thickness versus split-thickness skin grafts. J Hand Surg 2003;
28B:125-130.
11. Quaba A, Davison PM. The distally-based dorsal hand flap. British
Journal of Plastic Surgery 1990; 43:28-39.