Abstract
Objectives: This study was conducted to
evaluate the extent and efficacy of combining infraclavicular and axillary
brachial plexus block for arteriovenous shunt using graft versus performing
each mentioned block alone.
Methods: Eighty-two ASA III and IV
patients were allocated randomly to receive either true axillary block
(Hirshels’ technique) (group I, 26 patients), or Infraclavicular block (group
II, 28 patients), or combined Infraclavicular and Hirshels’ axillary block (group
III, 28 patients). All patients received 40-50ml bupivacaine 0.375%. The extent
and efficacy of anesthesia (nerve gaps) complications and duration of analgesia
of all groups were recorded and analyzed.
Results: The three groups were comparable
according to age, gender and weight. The duration of operations was 105±15 minutes,
and 18-20 minutes after the completion of block all patients in the three groups
demonstrated sufficient surgical anesthesia.
Five patients from group I, three patients from group II and two patients
from group III needed supplementation with xylocaine subcutaneously or with
intravenous analgesics and sedatives (fentanyl 50mcg, ketamine 10-50mg with
midazolam 1-2mg) during incisions of lateral aspect of arm or forearm (musculocutaneous
and radial nerve distribution or intercostobrachial nerves distribution). Blood
taps were recorded in three patients from group I. However, the combined group
showed superior anesthesia regarding the three previously mentioned nerves
compared with the single site blocks.
Conclusion:
Combined infraclavicular and axillary block
anesthesia demonstrates an extensive sensory and motor block in comparison with
performing the same blocks individually.
Key words:
Axillary block, Brachial
plexus block, Combined infraclavicular block
JRMS
December 17(4): 51-55
Introduction
Operations
performed for arteriovenous shunting using grafts take place at the inner
aspect of the arm, elbow, forearm and axillary region. The sensory supply of these regions is
provided from the intercostobrachial nerves (T1-T3) and medial cutaneous nerves
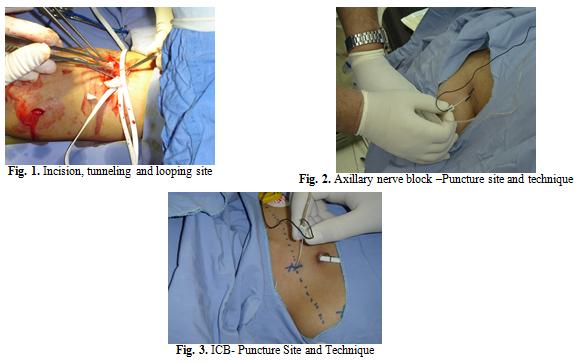
of the arm and forearm. Graft insertion,
looping and tunneling are carried out with small incisions at the mediolateral
aspect of the arm and forearm (Fig. 1).
This region is supplied entirely by branches of the musculocutaneous and
radial nerves. Numerous techniques are
now available to block the brachial plexus along its course. Infraclavicular
and axillary approach would block brachial plexus where all cords and most of
its branches are at close proximity.
Several studies have been performed in the recent years to investigate and
compare the efficacy of different single site blocking procedures but success
rate varies widely.(1-20) A major way to improve the success rate has
been to locate and separately block each nerve along its course which is time
consuming in a busy day case surgery department.(1,5,10)
Infraclavicular
brachial plexus block (ICB) has been shown to be frequently successful while
using a single–stimulation technique.(2-4) The stimulation
should be targeted to the musculocutaneous, median or radial nerve at the level
of the cord before these nerves leave the brachial plexus, however, the
incidence of complete paralysis and complete anesthesia of the upper limb was
low in some studies(3) and good in other studies.(4) Whereas, true axillary approach is more successful
in blocking the intercostobrachial nerves and medial cutaneous nerves, it requires
3-4 stimulations to obtain a high success rate.(5,6) The
block needle should be inserted high enough in the axilla (in close proximity
to musculocutaneous nerve), to block the musculocutaneous nerve which
frequently is missed.(7)
We
hypothesized that combining ICB and true axillary block together would have
equally efficient dissemination of the anesthesia (radial and musculocutaneous
nerves, medial cutaneous nerves and intercostobrachial nerves) and better block
effectiveness.
Methods
Institutional
approval and informed written consent was been obtained from 82 patients (ASA
II, III and IV) who were scheduled for arteriovenous shunt (AVF) using graft
under brachial plexus block anesthesia. Patients with coagulation profile
abnormalities, previous clavicular fractures or chest abnormalities, venous
dilatation and hypertension of the upper arm, and those who refused to
participate were excluded from the study.
The
study patients were randomly divided into three groups: Group I (n=26)
was scheduled to receive true axillary approach for brachial plexus block
according to Hirshels’ method, group II (n=28) was scheduled to receive infraclavicular
block and group III (n=28) was scheduled to receive both blocks as
described previously. The volume of the
local anesthetics was halved between the two blocks.
During Hirshels’
method the patient lies in supine position, the arm to be blocked is abducted 90° at the most and is positioned on a cushioned surface (e.g. arm
table) in a relaxed manner.
The course of the axillary artery of the medial upper arm can be palpated
dorsal from the medial bicipital groove. The puncture site is located slightly
above the axillary artery, at the highest point in axilla and slightly beneath
the pectoralis major muscle, which borders the axilla ventrally. After disinfection
and local anaesthesia of the puncture site with 1% xylocaine, the stimulation
needle is inserted parallel to the axillary artery at a 30° angle to the skin.
Contractions are sought in the area of the median nerve, or even better, of the
radial nerve. Once the threshold current is reached, 40-50 ml of the local
anesthetic (bupivacaine 0.375%) is injected (Fig. 2). During injection, pressure distal to the
injection point helps the local anesthetic to cephalad migrate up in the axilla.
In
the infraclavicular approach the patient is positioned in supine position, with
the hand of the side to be blocked positioned on the abdomen. The puncture site
is located at the halfway point between the ventral apophysis of the acromion
and the jugular fossa. After disinfection and local anaesthesia of the puncture
site with 1% xylocaine, the stimulation needle is inserted directly beneath the
clavicle and in a strictly vertical direction. Usually, at this site, after
reaching a desired depth, the primary segments of the lateral cord
(contractions of the biceps brachii muscle) are stimulated, then the needle is redirected
until the desired motor response (the peripheral contractions of the finger
muscles: extensors or flexors D I-III, i.e., muscles supplied by the
radial or median nerve) is achieved. Once the threshold current is reached,
40-50 ml (up to 3mg/kg of maximum dose) of local anesthetic (bupivacaine
0.375%) is injected (Fig. 3).
All
blocks were performed using contiplex insulated needles, 50mm, 22 gauge and
nerve stimulator (Digistem 3 Plus, Organon Teknika). The local anesthetic was
injected after we sought a distal and clear motor response in the hand or wrist
with stimulating intensity ranging between 0.5 and 0.3 mA. The procedure
duration was measured from the needle insertion to withdrawal. Disinfection, toweling and other preparations
were not considered as part of procedure duration. The same senior anesthetist
performed all blocks.
Another senior anesthetist, tested the
patients for sensory and motor block, the test was carried out every five minutes for 25 minutes, a successful block was defined as the absence of cold and pinprick response in the distribution of the musculocutaneous, radial, medial cutaneous nerves,median and ulnar nerves (0 = no sensation to 2 = normal sensation).
|
|
|
|
Table I. Patients
and Surgical Data
|
|
Group I (Axillary block)
|
Group II ( ICB)
|
Group III (Combined block)
|
|
Gender (M/F)
|
10/16
|
12/16
|
12/16
|
|
ASA (II/III/IV)
|
5/12/7
|
8/11/9
|
8/13/7
|
|
Age ( Years± SD)
|
36.4±7.2
|
38.8±4.8
|
37.2±5.6
|
|
Weight (Kg)
|
72.7±6.8
|
69.8±5.7
|
73.5±5.921
|
|
Type of Surgery
|
|
|
|
|
Forearm Graft
|
7
|
8
|
9
|
|
Bracheo-Axillary
Graft
|
10
|
11
|
10
|
|
Bracheo-Brachial
Graft
|
2
|
1
|
1
|
|
Cubital Fossa
Fistula
|
3
|
4
|
3
|
|
Basilic Vein
Transposition
|
2
|
1
|
2
|
|
Axillo-axillary Graft
|
2
|
3
|
3
|
|
The
motor block was assessed with a scale from 0 to 5 (0 = complete paralysis to 5 =
normal muscular force). If sensory gaps
were present at 20 minutes from the time of needle withdrawal (completion of
block procedure), the surgeon was informed to add local subcutaneous anesthetic
at the site if needed, and or we
considered the addition of analgesics and sedatives (fentanyl 50 mcg, ketamine
10-50 mg with midazolam 1-2 mg)
intravenously.
Venous
and/or arterial puncture, complications from overdose and/or inadverant
intravenous local anesthetics, such as convulsion, arrhythmia or pneumothorax
were recorded. Further follow up for late complications such as paresthesia or
prolonged nerve injury, pain, infection or retrospective bad experience from
anesthesia or surgery was carried out by the surgeon using a Liker scale
ranging from 0=no satisfaction to 5=very satisfied.
Statistical
analysis was performed descriptively using means, standard deviations and
frequencies. The Chi-square statistical test was used for bivariate analysis. The
level of significance was set at P>0.05.
Results
All groups were comparable in relations to
age weight and gender. Table I shows all groups demographic and surgical data.
The
time to perform the ICB (group II) block was significantly shorter (3.6±1.4 min)
than the two other groups (5.2 ±1.3, P<0,001 for group I and 6.3 ± 1.6, P<0.001
for group III).
The
onset time was almost similar for the three groups. It was 18.9 minutes for group I, 19.8 minutes
for group II, and 18.3 minutes for group III.
The
success rate was 80.7% for group I, 89.28% for group II and 92.8% for group
III. Five patients of group I complained
of pain sensation from incision at lateral or mediolateral aspect of the arm;
supplementation of xylocaine was done by the surgeon at the site of incision. Two
of these patients needed extra supplementation of analgesics and sedatives
during the procedure. Three patients of group II required supplementation of
xylocaine at the incision site and intravenous analgesics and sedatives at the
beginning of the procedure, later on no analgesics nor xylocaine subcutaneously
were needed.
Two
patients of group III complained of pain sensation at the beginning of operations,
the addition of 10-50mg ketamine with 1-2mg midazolam intravenously appear to
be sufficient to continue the procedure with no further complaints.
Blood
tap (venous or arterial puncture) was recorded in two patients of group I and
two other patients in group III with no clinical consequences. No clinical
consequences from vascular absorption or overdose of local anesthetics were
observed in all groups.
A
high degree of satisfaction was recorded in 96.4% of group III versus 88.4% of
group I and 92.8% of group II.
Discussion
In
this study we report the efficacy of combining infraclavicular and axillary
plexus block by single elctrostimulation for each block. The combination method
in our study led to a high degree of satisfaction. In our technique, a single stimulation is
required for each block, which led to high success rate for blocking the
musculocutaneous, intercostobrachial and medial nerves of the arm and forearm in
addition to the other nerves (radial, median and ulnar) forming the brachial
plexus.
The
reported success of axillary block alone by single elctrostimulation varies
widely (43-85%),(8-10) this may be explained by the
difficulty of identifying and blocking the musculocutaneous nerve, which leaves
the plexus high in the axilla. In the axillary block, despite the higher success
rate from multiple stimulations technique, withdrawal and redirection of the
stimulating needle to elicit the different muscular twitches increases the
patients’ discomfort and the mean time to perform the block, as well as it
causes a more vascular puncture.(8,9)
Many
studies comparing single elctrostimulation ICB with single stimulation axillary
block, suggest a higher success rate (97-100% vs. 80-85%)(2,11,12)
possibly due to better blockade of the radial and musculocutaneous nerves,
however, Borgeat, reported a success rate of 44% when a proximal motor response
was accepted for local anesthetic injection.(13,14) In order
to increase the success rate, many authors advocated a dual or triple
stimulation technique; however, while this method increases the success rate,
the time needed for its performance was slightly greater (9±3 minutes).
In
our study, we have found that there was no significant difference in success
rate in multiple stimulation axillary block (92.8% vs. 93%, P≤0,005)(10,17)
or dual stimulation infraclavicular block (92.8% vs. 92%, P≤0.005).(17,18)
The mean performance time was also similar for dual stimulation infraclavicular
block (6.3 vs. 4.5-6.2 minutes, P≤0.005),(14,17) and
significantly less than performing quadruple axillary block (6.3 vs.
8.4- 9.8 minutes, P≥0.05).(9,10,17) However, because of the reduced number of
needle stimulations and injections, combining both blocks resulted in greater
patient satisfaction and fewer side effects such as arterial and venous
puncture.(5,10,19) In addition, Orlowski and his colleagues,(20)
using high resolution scanning, were able to demonstrate contrast leakage
outside the brachial plexus sheath along the chest wall once a volume of 20ml
or more contrast medium had been injected in cadavers in the supine
position. Therefore, we assumed that by
dividing the local anesthetic volume in two a site block may reduce the leakage
volume, which may results in a better success rate and better dissemination of
the local anesthetics along the brachial plexus course.
Conclusion
Combining
both single stimulation axillary block and infraclavicular block is simple,
very effective, has a high success rate with few side effects, and is very well
tolerated by patients.
References
1.
Lavoie J, Martin R, Tetrault JP, Cote DJ, Colas MJ. Axillary
plexus block using a peripheral nerve stimulator: single or multiple
injections. Can J Anesth 1992; 39: 583-6.
2.
Kapral S, Jandarasits
O, Schabenig C, et
al.Lateral
Infraclavicular plxus block versus axillary block for hand and forearm surgery.
Acta Anesthesiol Scand 1999; 43:1047-52.
3.
Bloc S,Garnier T, Komly B, et
al.
Single-stimulation low- volume Infraclavicular plexus block: influence of
evoked response on success rate. Reg Anesth Pain Med 2006; 31:
433-7.
4.
Lecamwasam H, Mayfield J, Rosow
I, et al. Stimulation
of the posterior cord predicts successful Infraclavicular block. Anesth
Analg 2006; 102; 1564-8.
5.
Koscielniak-Nielsen ZJ,
Hesselbjerg I, Fejlberg V. Comparison of transarterial and multiple nerve
stimulators for an initial axillary block by 45 ml of mepivacaine 1% with
adrenaline. Acta Anesthesiol Scand 1998; 42: 570-5.
6.
Handoll HH, Koscielniak-Nielsen ZJ. Single, double, or multiple injection
techniques for axillary brachial plexus block for hand, wrist or forearm
surgery. Cochrane Database Syst Rev 2006; 1CD003842.
7.
Youssef MS, Desgrand DA. Comparison of two methods of axillary brachial plexus anesthesia. Br J
Anesthesia 1988; 60: 841-4.
8.
Fanelli G, Casati A, Garancini P,
Torri G. Nerve
stimulator and multiple injection technique for upper and lower limb blockade;
failure rate, patients acceptance, and neurological complications. Anesth
Analg 1999; 88: 847-52.
9.
Sia S, Lepri A, Campolo MC,
Fiaschi R.
Four-injection brachial plexus block
using peripheral nerve stimulator: a comparison between axillary and humeral
approaches. Anesth Analg 2002; 95: 1075-9.
10. Lavie
J, Martin R, Tetralaut JP, Cote DJ, Colas MJ. Axillary plexus
block using peripheral nerve stimulator:
single or multiple injections. Eur J Anesthesiol 1997; 14:164-71.
11. Rettig
HC, Gielen JM, Boerma E, Klein J. A comparison of the vertical
Infraclavicular and axillary approaches for brachial plexus anesthesia. Acta Anesthesiol Scand 2005; 49:1501-8.
12. Heid FM, Jage J, Guth M Bauer N, Brambrink AM. Efficacy
of vertical Infraclavicular plexus block vs. modified axillary plexus block: a
prospective, randomized, observer-blinded study. Acta Anesthesiol Scand
2005; 49: 677-82.
13. Borgeat
A, Ekatodramis G, Dumont C. An evaluation of
the Infraclavicular block via a modified approach of the Raj technique. Anesth
Analg 2001; 93: 436-41.
14. Gaertner
E, Estebe JP, Zamfir A, Cuby C, Macaire P. Infraclavicular plexus block:
multiple injections versus single injection. Reg Anesth Pain Med 2002;
27:590-4.
15. Rodriguez
J, Barcena M, lagunilla J, Alvarez J. Increased success rate with
Infraclavicular brachial plexus block using a dual- injection technique. J
Clin Anesthesiol 2004; 16: 251-6.
16. Rodriguez
J, Tabonda M, DelRio S, Barcena M, Alvarez J. A comparison of four stimulation
pattern in axillary block. Reg Anesth Pain Med 2005; 30: 324-8.
17. Minville V, Amathieu R, Luc N, et al. Infraclavicular
brachial plexus versus humeral approach: comparison of anesthetic time and efficacy.
Anesth Analg 2005; 101:1198-201.
18. Minville
V, Fourcade O, Idabouk I, et al. Infraclavicular
brachial plexus block versus humeral canal block in trauma patients: a
comparison of patient discomfort. Anesth Analg 2006; 102: 912-5.
19. Koscielniak-Nielsen
ZJ, Rotboll Nielsen P, Risby Mortensen C. A comparison of coracoid and
axillary approach to the brachial plexus. Acta Anesthesiol Scand 2000;
44: 274-9.
20. Orlowski
O, Bullmann V, Vieth V, et al. Perivascular axillar brachial plexus
block and patient positioning: the influence
of the lateral, head-down position. Anesthesia
2006; 61: 528-35.