Abstract
Objectives: To present the learning
style of surgeons and compare it to their medical colleagues.
Methods: This study was conducted
at King Hussein Medical Center between 1-15/July 2014. An equal number of randomly
selected surgeons and physicians received Honey and Mumford learning style
questionnaire. The participants were asked to fill the questionnaire with their
name initials, age, gender, specialty (surgeon or physician) and scientific medical
level (specialist or consultant). The results between these two groups were
compared using statistical methods.
Results: A total number of 40 participants
filled the questionnaire, 20 in each group. Thirty six (90%) were males, with a
mean age of 37.6 years (SD ± 6.32). There were 7 consultants and 33
specialists. The majority (80-90%) of surgeons and physicians showed reflector
and theorist learning styles. When grouping them into activist/ pragmatist,
reflector/ theorist or mixed learning styles; 80% of surgeons and 90% of
physicians demonstrated mixed learning style.
Conclusion: Both surgeons and
physicians demonstrated a mixed learning style. This means that doctors in both
specialties use all four learning styles which inevitably will bring the best
learning results. We suggest the application and appreciation of all learning
styles in the surgical curriculum as the most educational and practical
approach.
Key
words: Learning style, Surgeons,
Physicians.
JRMS
December 2015; 22(4): 24-30 /DOI: 10.12816/0018546
Introduction
Learning style is the process by which a person
understands and retains information, thereby gaining knowledge or skills.(1)
Learning styles involve the cognitive processes
that are implicated in learning, and can be thought of as "learning habits"
that permit a learner to benefit more from some experiences than from others.(2)
Many types of
learning styles have been described
in the literature,(3) including Gardner's
Multiple Intelligence Theory(4)
and
Kolb's Learning Inventory.(5) The Kolb model is the most widely used,
statistically valid and reliable learning assessment tool. It function as a
well-established model which allows the comparisons of learning styles across
medical specialties and between training levels, and its experiential basis is
particularly relevant to the apprenticeship model of surgical training.(6)
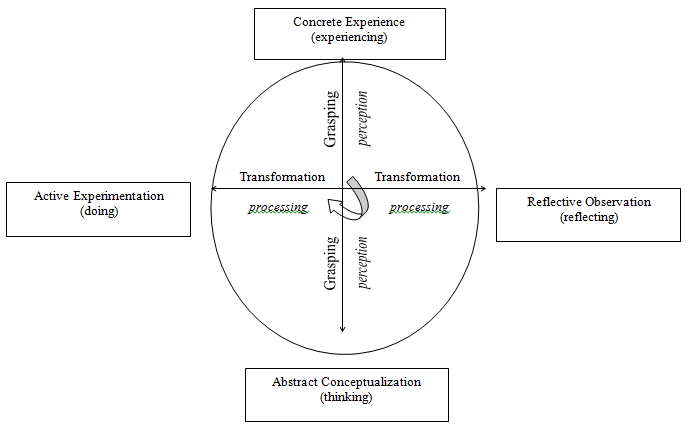
Fig.1. Kolb's learning cycle.
David Kolb(5) hypothesized that differences in the
way people learned had to do with the way they perceive and then process an
experience.
According to Kolb, two dimensions are necessary
for learning to occur. The first dimension is described as a grasping, or
perceiving, and the second one as a transformation, or processing. He developed
these dimensions into a learning cycle as a model of how people learn. The knowledge
is gained by moving around a circular learning process involving four defined
parts: concrete experience (experiencing), reflective observation (reflecting),
abstract conceptualization (thinking) and active experimentation (doing).(6)
Fig. 1.
For example, the surgical trainee would
experience the case during an operation in theater, reflect on this experience,
read about the case and formulate ideas and, finally, experiment by applying
change during his or her next encounter with the learning process.
Derived from experiential learning theory, Kolb
developed a learning styles inventory to measure an
individual’s preferential learning style based on the association between
individual's preference for certain part of the cycle and his or her learning
style.(7) This
inventory or list has been used in a number of studies on the learning styles
of medical students, residents and health care professionals.(8-10)
Subsequently, Honey and Mumford
developed their own validated learning style questionnaire (LSQ)(10)
that is based on Kolb's learning style inventory. They defined four overlapping
learning styles: activist (concrete experience), pragmatist (active
experimentation), reflector (reflective observation) and theorist (abstract
conceptualization), Fig. 2. In their learning styles, activist prefer doing and
experiencing, pragmatist like to "have a go", try things to see if
they work, reflector observes and reflects and theorist wants to understand
underlying reasons, concepts and relations.
The activists and pragmatists are
located on one side of Honey and Mumford learning cycle, they prefer to learn
by concrete experiencing and actively experimenting. On the other side of the
learning cycle are the theorists and reflectors,they prefer learning by abstract conceptualization and reflective observation. Ideally, a learner should be able to use each of the four different kinds of styles in order to gain the most effective learning results for every particular situation. However, individuals tend to develop preferences for one or more of the four learning styles.
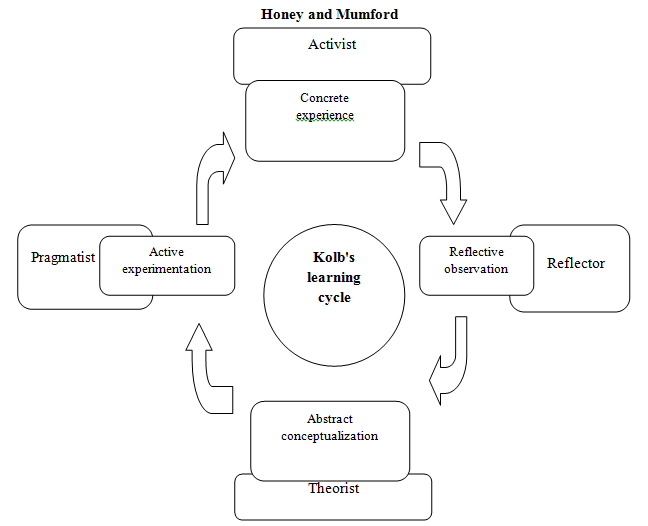
Fig.
2: Kolb's
and Honey and Mumford learning cycles
Most of surgical training involves
"hands on" approach, which might show a preference for
activist-pragmatist style of learning. This contrast to the medical training
where the practice are more logical step-by-step thinking, collecting data,
thoroughly reflecting on it before reaching a conclusion, i.e
reflector-theorist learning styles.(8,11)
The aim of our study was to identify
surgeons' learning style at king Hussein Medical Center, and compare it to
their medical colleagues.
Methods
This study was conducted between 1-15 July 2014 at
King Hussein Medical Center. After obtaining ethical committee approval, the
inclusion criteria to participate in the study was the completion of residency
and achievement of the Jordan board exam in either general surgery or general medicine.
A
Honey and Mumford LSQ was distributed among equal number of randomly selected surgeons
and physicians. Learning styles were assessed anonymously. The participants
were asked to fill the questionnaire with their name initials, age, gender,
specialty (surgery or medicine) and scientific level (specialist or
consultant), and return the questionnaire after completion. All LSQ answers
were marked by one author (AU).
Table I: Demographics of the
study population.
|
|
Surgeons
|
Physicians
|
Total (%)
|
P
|
|
Males
|
19
|
17
|
36(90)
|
0.00005
|
|
Females
|
1
|
3
|
4(10)
|
|
Mean age (years)
|
34.7
|
40.5
|
37.6
|
0.001
|
|
Consultant
|
1
|
6
|
7(17.5)
|
0.007
|
|
Specialist
|
19
|
14
|
33(82.5)
|
Table II: Distribution of
learning style preferences by specialty.
|
Style
|
Surgeons (%)
|
Physicians (%)
|
Total (%)
|
P
|
|
Activist
|
12 (60%)
|
13 (65%)
|
25 (63%)
|
0.74
|
|
Pragmatist
|
13 (65%)
|
11 (55%)
|
24 (60%)
|
0.52
|
|
Reflector
|
18 (90%)
|
18 (90%)
|
36 (90%)
|
NS
|
|
Theorist
|
16 (80%)
|
18 (90%)
|
34 (85%)
|
0.3
|
Table III: Distribution of
learning style preferences by age, gender and scientific level.
|
Style
|
Mean age
(years)
|
Gender
M: F
|
Scientific
level
Consultant:
Specialist
|
|
Activist
|
37.4
|
23: 2
|
5: 20
|
|
Pragmatist
|
37.2
|
22: 2
|
4: 20
|
|
Reflector
|
37.5
|
32: 4
|
6: 35
|
|
Theorist
|
38.2
|
32: 2
|
7: 27
|
This questionnaire consists of 80 questions that
measures respondents' agreement with different statements to analyze their
preference for particular learning style.(12) One
point was scored for the agreement of the statement and no points for
disagreement. Then points were added and each individual's profile calculated
(activist, pragmatist, reflector or theorist). The preference was graded as
follow: very strong, strong, moderate, low and very low preferences. Participants
with a very strong or strong preference for any learning style were selected as
having a preference for that particular style of learning.
They were then grouped into three groups; first
group with an activist / pragmatist preference, second group with reflector/
theorist preference and the last group with mixed learning style preference.
The results were analyzed using SPSS 16 (SPSS
Inc. Chicago, IL, US). Chi-square test was used to determine any relationship
between two variables ie. learning style and either specialty, scientific level,
age and gender. Student's t-test was used to compare between surgeons and
physicians in regard of age, gender and scientific level. P-value less than
0.05 was considered significant.
Results
Overall survey response rate was 100% (40/40); 20
participants from each specialty returned their questionnaire. There were 36 (90%)
males and the mean age for the whole group was 37.6 years (SD 6.32), with a
total of 33 specialists and 7 consultants, Table I.
The
LSQ results showed that reflector and theorist learning styles where favored by
surgeons (90% for reflector and 80% for theorist styles) and by the physicians
(90% for reflector and 90% for theorist styles), with no statistical differences
between the two groups, Table II. The mean age among surgeon and physicians for
different learning styles preference is reported in Table III. The mean age for
the preference for the pragmatist style was 37.2 years, and it was 38.2 years
for the theorist style. The preference of learning styles by gender showed that
half of the female doctors preferred activist, pragmatist and theorist learning
styles, while all 4 of them (100%) showed preference for reflector style. Male doctor’s results ranged
from 61% preference for pragmatist style to 89% preference for reflector style. In addition, all consultants preferred reflector learning style compared to only 82% of specialists, Table III.
Table IV: The difference of
learning styles by specialty, age, gender and scientific level.
|
Style
|
Surgeon (%)
|
Physicians
(%)
|
Mean age (years)
|
Gender
(M: F)
|
Level
(Consultant:
Specialist)
|
|
Activist/ Pragmatist
|
2 (10%)
|
0
|
33.5
|
2: 0
|
0: 2
|
|
Reflector/ Theorist
|
2 (10%)
|
2 (10%)
|
38
|
3: 1
|
0: 4
|
|
Mixed
|
16 (80%)
|
18 (90%)
|
37.8
|
31: 3
|
7: 27
|
When grouping the learning styles into activist/
pragmatist, theorist/ reflector or mixed, we noticed that only two surgeons and
no physicians have the preference for activist/ pragmatist learning styles. In
addition, 2 surgeons and 2 physicians have the preference for theorist /
reflector learning styles. However, 16 surgeons and 18 physicians have mixed
learning styles. There was no
statistical difference between learning style groups and specialty, age, gender
and scientific level, Table IV.
Discussion
In order to produce competent and successful surgeons,
it is important to consider not only what they are learning but how they are
doing so. Many evidence demonstrated that surgical trainees have specific
learning styles and identifying and focusing on these has the
potential to improve the delivery of surgical education.(13,14)
Studies in general surgery have shown that the predominant learning styles of
surgical trainees is activist and pragmatist, i.e they learn by doing,
involve themselves fully and without bias in new experiences, they try
out new ideas, theories and techniques to see if they work. (13- 15)
Our study demonstrated that the main learning
styles of surgeons are reflector and theorist, 90% and 80% respectively. These
two learning styles were also predominant among physicians, 90% each. The
reflector style was prevalent among specialists and consultants. This suggests
that the majority of specialists and consultants in both specialties take time
to think over experiences and observe them from
many different perspectives. They collect data, both first hand and from
others, and prefer to think about it thoroughly before coming to a
conclusion. However, we cannot make any solid conclusions regarding the preferred
learning style of either surgeons or physicians, males or females, consultants
or specialists because the majority showed mixed learning style.
The surgical specialty is a "hands on"
profession. Surgeons spend most of their careers in theaters operating. We
assume that during the first years of the residency, junior trainees learn the
basic concepts of surgery, i.e anatomy, normal and abnormal physiology of the
human body, etc, they see the operation, listen to explanation from the surgeon
and read about it. At this time the theorist/ reflector learning style will
dominate. In more senior years, residents will display the activist/ pragmatist
styles, they will learn from the practical procedure itself. They will be able
to learn efficiently from assisting in a demonstration and then performing the
procedure under direct supervision and later by themselves. A study by Engels
et al 11 showed significant differences in learning styles between
undergraduate medical students and general surgery residents and faculty
members. The undergraduates demonstrated a theorist learning style while the
residents and faculty showed the activist/ pragmatist learning styles.
However, if a resident is struggling to learn
how to perform a procedure in theaters, then it is important to consider if he
or she has a more theorist/ reflector style. In this case, and prior to the
operation, teaching should be focus on discussion of and reading the principles
of the procedure prior to it and formalized reflection afterwards.
Our results showed two main differences to other
reports(1,16) that demonstrated that the
predominant learning style of surgeons are activist and pragmatist. First, only
10% of surgeons showed activist/ pragmatist learning styles and second, the
majority of participants in the survey demonstrated mixed style of learning. These
variations in learning styles among surgeons at our institution that is
different from published literature could be explained by the variety of
learning styles used by senior surgeons, trainers and consultants that are
involved in training the surgical residents. In addition, the resident go
through all learning styles during his progress from year one to year five of
residency. As discussed earlier we presume that he or she starts with reflector/
theorist learning style and finishes with more practical training, i.e
activist/ pragmatist style of learning. We need to understand the learning
styles of the residents and how it evolves during the residency years, and how
to manipulate it in order for the trainees to gain maximum benefit from their
residency program.
Our recommendation is that the LSQ could be used
to assess the learning style of the residents during different stages of
training, and identify changes in the trainees' learning styles. In addition, knowing
the range of the learning styles of residents will help to improve the teaching
and learning process by alteration methods of teaching to adapt individual's
learning capabilities.
Limitations of the study
Small number of participants and single
institution participation in the survey.
Conclusion
Our study demonstrated that both surgeons and
physicians have mixed styles of learning. Using all learning styles during
residency and afterwards inevitably will bring the best learning results. For
surgeons, the reflector/ theorist style will lead to better understanding the
theories of surgical science and its applications, and the activist/ reflector
style will produce a competent and confident surgeons in theaters. Future
studies will highlight the learning styles of the residents and how it changes
during their training years. This will guide to develop the residents' training
curriculum for both specialties taking into consideration different learning
styles.
References
1. Adesunloye BA,
Aladesanmi O, Henriques-Forsythe M, et al.
The Preferred Learning Style among Residents and Faculty Members of an
internal Medicine Residency Program. J Natl Med Assoc 2008; 100:172-175.
2.Valley K. Learning styles and courseware design. ALT
J 1997; 5: 42-51.
3.Romanelli F, Bird E,
Ryan M. Learning
Styles: A Review of Theory, Application, and Best Practices. American
Journal of Pharmaceutical Education 2009, 73:1-5.
4.Windsor JA, Diener S,
Zoha F. Learning
style and laparoscopic experience in psychomotor skill performance using a
virtual reality surgical simulator. The American Journal of Surgery 2008,
195:837-842.
5. Kolb D. Experiential Learning: Experience as the
Source of Learning and Development. Englewood Cliffs, NJ: Prentice Hall, 1984.
6.Armstrong E, Parsa-Parsi
R. How Can
Physicians’ Learning Styles Drive Educational Planning? Acad Med 2005;
80:680-684.
7.Kolb D, Kolb A. The Kolb Learning Style Inventory-Version
3.1 Technical Specifi cations. Experience Based Learning Systems, Inc. Hay
Group, 2005.
8.Samarakoon L, Fernando T, Rodrigo C, et al. Learning styles and approaches to
learning among medical undergraduates and postgraduates. BMC Medical
Education 2013, 13:42; 1-6.
9.Bitran M, Zuniga D, Pedrals N, et al. Medical students' change in learning
styles during the course of the undergraduate program: from ‘thinking and
watching’ to ‘thinking and doing’. CMEJ
2012, 3(2):e86–e97.
10. Wilkinson T, Boohan M, Stevenson M Does learning style influence academic performance in
different forms of assessment? J ANAT 2014; 224: 304-308.
11.Engels P, de Gara C. Learning styles of medical students,
general surgery residents, and general surgeons: implications for surgical
education. BMC Medical Education 2010; 10(51):1-6.
12.Honey P,
Mumford, A. The Learning Styles Questionnaire, 80-item version. Maidenhead,
UK, Peter Honey Publications, 2006.
13.Contessa J, Ciardiello
KA, Perlman S. Surgery
Resident Learning Styles and Academic Achievement. Curr Surg 2005;
62:344-347.
14.Kneebone R, Aggarwal R. Surgical training using simulation. BMJ
2009; 338:1220-1221.
15.Osborne A, Hawkins S,
James A, et al.
Training in current medical education: surgeons are different from their
medical colleagues. Ann R Coll Surg Engl (suppl) 2012; 94: 242-245.
16. Mammen J, Fischer D,
Anderson A, et al.
Learning styles vary
among general surgery residents: analysis of 12 years of data. J Surg Educ
2007; 64: 386-389.