Abstract
Objective: To
evaluate the effectiveness of endoscopic repair of congenital choanal atresia
by removing the posterior aspect of the vomer bone along with the atretic plate
without stenting.
Methods: This
retrospective study included 16 children aged (6 days-13 years) who presented
or referred to Queen Rania Hospital with congenital choanal atresia. Patients
who had unilateral, bilateral, primary or revision cases were included in the
study. All patients underwent endoscopic repair by removing the posterior
aspect of the vomer bone along with the atretic plate without stenting. All
patients were followed up for 18 months.
Results: Four patients were males, 12 were females. Three cases had bilateral
atresia, one of them was revision. 13 cases were unilateral, 5 of them were
revision cases. In unilateral cases the right side was involved in 8 cases and
5 in the left side. All cases were repaired endoscopically without stenting,
only one patient out of 16 patients needed revision surgery.
Conclusion: Endoscopic
repair of choanal atresia (unilateral or bilateral, primary or secondary)
without stenting is an effective and safe method of treating choanal atresia
with a high success rate.
Key words: Choanal atresia, Endoscopic, Stenting
JRMS December 2015; 22(4): 40-43 /DOI: 10.12816/0018551
Introduction
Congenital
choanal atresia is a congenital anomaly of the posterior nasal aperture that
prevents airflow from the nose to the nasopharynx.(1) It is
caused by failure in rupture of the nasobuccal membrane of Hochstetter which is
normally reabsorbed during the sixth week of gestation.(2)
Although it is a
rare condition, it is the most common congenital nasal malformation with
incidence of one in every 8000-10000 live births. (3) It was
first described by Johann Roederer in 1755.
Females are affected more than males. (4) It may be
unilateral or bilateral, isolated or associated with other craniofacial
anomalies, with CHARGE syndrome being the most commonly associated anomaly.(2)
Since infants are
obligate nasal breathers for the first few days after birth and have no ability
to breathe through mouth, bilateral choanal atresia presents as medical
emergency at birth with symptoms of respiratory distress and cyanosis which is
relieved by crying. (5) Diagnosis is suspected immediately at
birth after failure to pass nasogastric tube and confirmed by CT scan.
Immediate airway management is necessary by insertion of oropharyngeal airway,
orotracheal intubation or definite treatment by surgical repair.(6)
Unilateral cases may remain undetected till late adulthood with symptoms of
nasal obstruction and mucoid nasal secretions.(3) Its
composition may be bony, membranous or mixed (bony and membranous) which is the
most common type.(7)
Many surgical
approaches have been used with endoscopic transnasal being the most preferred.(2)
There is a great controversy regarding placing stents or not.(5)
The aim of our study is to evaluate the effectiveness of repair of congenital
choanal atresia endoscopically without stenting.
Methods
This
retrospective descriptive study was conducted at Queen Rania Pediatric
Hospital. The case notes for all patients who had choanal atrersia and
underwent surgery from September 2009- September 2014 have been reviewed and
the following data have been collected from the case notes: age, gender,
presenting symptoms, type of anesthesia, prior surgery, CT scans, type of
choanal atresia, surgical technique, associated malformations, recurrence and
complications.
The surgical
technique used is done under general anesthesia via orotracheal intubation. In
all patients, packs soaked with adrenaline 1/10000 were inserted in both nasal
cavities. Then infiltration with adrenaline 1/100000 was done in both sides of
the septum, the atretic plate and through the mouth to the palate midway
between the midline of the palate and the deepest gingiva. Using the zero
degree 2.7mm sinus telescope, a puncture was done at the infero-medial side,
then by using the french backbiter the posterior part of the vomer bone was
removed in peices. The choana was widened using the backbiter, same was done
for the other side then the posterior end of the septum was removed to make
both choanae communicate together in a common wide neochoana, Fig. 1. In all
our bony cases, using puncture and french backbiter was enough to open and
widen the cavity, but if thick or hard bone was found using drill may be
needed. Using microdebrider, trimming
the mucosa of the edges of the common choana was done.
All patients were
discharged with nasal decongestants and nasal saline lavage. All patients
enrolled in the study were followed up for 18 months to detect patency of
posterior choana by nasal endoscopy. The study population was comprised of 16
patients with age ranges (6 days-13 years).

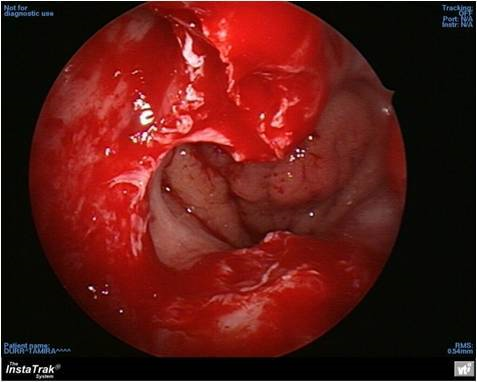
Fig. 1: Wide common neochoana after removal of the vomer bone
and posterior septum
Results
Sixteen patients
aged (6 days-13 years) were enrolled in the study. 4 patients were males with
mean age of 6.2 years and 12 were females with mean age of 7.8 years, Table I. Three
cases were bilateral, 2 of them were primary cases and one of them had previous
surgery at other peripheral hospital (revision cases). Thirteen cases were
unilateral, 8 of them were primary cases and 5 were revision cases. In
unilateral cases the right side was involved in 8 (62%) cases and 5 (38%)
patients had the left side involved. Regarding the nature of the atresia, 12
cases were found to be of a mixed type, 4 cases were pure bony and none were of
the membranous type, Table II. Two patients had associated malformations, one
had CHARGE syndrome and the other had atrial septal defect.
Follow up for
these patients was done for 18 months. All patients had patent posterior
choana, except one male patient with right side primary mixed type developed
re-stenosis after 6 months and needed revision surgery. Only one patient
developed bleeding post operatively and was managed by a nasal pack.
Discussion
The surgical technique used to repair all patents in our study patients
was done by endoscopic removal of the atretic plate with wide resection of the
vomer bone and the posterior septum to obtain a large choana without stenting.
Only one patient developed restenosis; out of the 16 patients, 12 were
females, 13 were unilateral with the right side involved in 8 of them and 12 patients were of mixed type.
Congenital choanal atresia is the
most common congenital nasal anomaly.(1) Its presentation
varies from respiratory difficulty, only during infection, to complete
obstruction. Bilateral atresia presents early with respiratory distress while
unilateral atresia may remain asymptomatic until first upper respiratory tract
infection develops.(8)
It is more common in females,(3) in our study we also
found that females (75%) are more affected than males (25%), although some
studies showed no gender difference, as in a study done by Hengerer AS, et
al on 73 patients.(9) In unilateral cases higher prevalence was
found in the right side,(1) also in our study right side was
involved in 62% of patients.
Congenital choanal atresia is classified according to composition into:
Bony, membranous and mixed (bony and membranous). The most common type is
mixed, in a study done by Manica et al(1) mixed type
was found to be (77.8%). In our study 3 cases out of 14 (19%) were found to be
pure bony. While 13 patients were of mixed type (81%) and none of our patients
were of membranous type. It may be an isolated anomaly or one feature of
associated anomalies as CHARGE syndrome. In our study only one case was
associated with CHARGE syndrome which is female with bilateral mixed type.
Different approaches for surgical repair are used. Endoscopic, transnasal,
transpalatal and transseptal. The transpalatal approach has many drawbacks: time
consuming, increased bleeding risk, maxillofacial growth problems, palatal
dysfunction and palatal fistulas.(3) The transseptal approach
is rarely used for younger patients with unilateral atresia and now the
transnasal approach is the preferred approach.(5)
In our study, only one patient out of 16 patients developed re-stenosis
(6%), so, the success rate was 94%. In a study done by Schoem SR, they analyzed
13 children who underwent transnasal endoscopic repair without stenting, there
were no recurrent cases.(10) Another study done by Ibrahim
AA, et al on 21 patients using the same approach showed that 3 patients
developed restenosis.(11) Also, Cedin AC, et al used
stentless folded -over-flap technique and no recurrent cases were found.(12)
A study done by El-Ahl MA, et al using the same technique showed a zero recurrence rate.(13)
Also Magdy ES in his comparative
study between stent and non-stent groups found that the use of stents didn't
decrease the re-closure or restenosis rate.(5) On the other hand
in Sun P, et al study on 15 patients
using stents for 3 months, no recurrence rate was found.(14)
All revision cases in our study were done primarily in peripheral
hospitals using stents and all were revised endoscopically without stenting. No
recurrent cases were found.
Using stents has many disadvantages; it causes discomfort, localized
ulceration, erosion of the nares, needs long-term antibiotics use, stent
blockage and the unsightly aspect of having stents protrude from the nose.(5)
Mitomycin, which is
an antiproliferative agent, that prevents granulation formation by inhibiting
fibroblast formation, has not been applied to our patients. Success rate was
excellent without applying it.
The limitation of
our study was the small number of patients; to get more reliable result we
recommended a prospective study with large number of patients.
Conclusion
Endoscopic repair
of congenital choanal atresia (unilateral or bilateral, primary or secondary)
by removing the posterior aspect of the vomer bone along with the atretic plate
without stenting is an effective and safe method of treating choanal atresia
with high success rate.
References
1. Manica D, Schweiger C, Netto CCS, et al. Retrospective study of a series of choanal atresia patients. Int Arch Otorhinolaryngol 2014; 18:2-5.
2. Llorente JL, López F, Morato M, et al. Endoscopic treatment of choanal atresia. Acta Otorhinolaryngol Esp. 2013; 64(6): 389-395.
3. Rodríguez H, Cuestas G, Passali D. A 20-year experience in microsurgical treatment of choanal atresia. Acta Otorhinolaryngol Esp 2014; 65(2):85-92.
4. Velegrakis S, Mantsopoulos K, Iro H, Zenk J. Long-term outcomes of endonasal surgery for choanal atresia: 28 years experience in an academic medical centre. Eur Arch Otorhinolaryngol 2013; 270:113-116.
5. Magdy S. Endoscopic management of congenital bilateral posterior choanal atresia: value of using stents. Eur Arch Otorhinolaryngol 2013; 270: 129-134.
6. Kumar S, Gupta S, Naglot S, Sahni JK. Bilateral choanal atresia: is it really a surgical emergency? Indian J Otolaryngol Head Neck Surg 2013; 65; 205-209.
7. Ceylan K, Emir H, Kizilkaya Z, Samim E. Bilateral congenital choanal atresia in a 7-day-old patient: transnasal endoscopic repair with stent. Eur Arch Otorhinolaryngol 2007; 264: 837-840.
8. Asma A, Roslenda AR, Suraya A, et al. Management of congenital choanal atresia after multiple failures: A Case Report. Med J Malaysia 2013; 68 (1):76-78.
9. Hengerer AS, Brickman TM, Jeyakumar A. Choanal atresia: embryologic analysis and evolution of treatment, a 30-year experience. Laryngoscope 2008; 118(5): 862-866.
10. Schoem SR. Transnasal endoscopic repair of choanal atresia: why stent? Otolaryngol Head Neck Surg 2004; 31(4): 362-366.
11. Ibrahim AA, Magdy EA, Hassab MH. Endoscopic choanoplasty without stenting for congenital choanal atresia repair. Int J Pediatric Otorhinolaryngol 2010; 74(2): 144-150.
12. Cedin AC, Fujita R, Laércio MCO. Endoscopic transseptal surgery for choanal atresia with a stentless folded-over-flap technique. Otolaryngol Head Neck Surg 2006; 135(5): 693-698.
13. EL-Ahl MA, EL-Anwar MW. Stentless endoscopic transnasal repair of choanal atresia starting with resection of vomer. Int J Pediatric Otorhinolaryngol 2012; 76(7): 1002-1006.
14. Sun P, Ge W, Liu W. et al. Transnasal endoscopic choanal plasty for repairing congenital choanal atresia. Chinese J of Otolaryngology Head and Neck Surgery 2014; 49(7): 564-567.