Abstract
Objectives: To determine
the percentage, reasons and possible suggested measures to reduce the rate of
cancellation of elective surgical operations.
Methods: This
descriptive study was performed at Queen Alia military hospital (QAH) in the
period between January 1st 2011 and January 1st 2012 by
collecting and analyzing the daily records of cancelled elective operations.
Results: A
total of 7163 patients were scheduled for elective surgeries during the study
period, 6601 patients had their operation performed at the scheduled time. 553 patients
had their operation cancelled at the day of surgery and the percentage of
cancellations was 7.72%.
The highest number of cancellation was observed
in December (70 cases out of 646 scheduled cases 10.84%) whereas February had the
lowest number of cancellations (23 cases out of 572 scheduled cases. 4.02%). General surgery and orthopaedics had the
highest number of cancellation (186 and 177 respectively) whereas ENT and
maxillofacial surgery had the least number of cancellations (38 and 10
respectively). The most common causes for cancellations were patient-related,
around 68% of the cancellations were due to patients’ absence and their medical
fitness for surgery at the day of planned operation, and the other causes of
cancellations were due to lack of time (overbooked list) or lack of necessary
equipments and devices.
Conclusions: The percentage
of surgical cancellation at our hospital is relatively low; most of the
cancellations could be easily avoided by efficient planning, proper
communication with the patients and proper preoperative medical assessment.
Key words: Cancellations,
Elective surgical operations, Operating theatres.
JRMS December 2015; 22(4): 52-56 / DOI: 10.12816/0018557
Introduction
Surgical cancellation is
defined as a scheduled surgery which is not performed at the intended date.
Cancellation of elective scheduled operations leads to an inefficient use of
operating room time, a waste of hospitals' resources and negative social and
psychological impact on both patients and their families.(1,2)
Thus, it is a healthcare problem in most hospitals where scheduled operations
are cancelled at the last minute, even on the day of surgery. Different
scenarios usually occur with regard to the cancellation procedure; in some
cases, patients have been prepared for theatre, and staffs are assembled and
expecting to operate. In others, patients and staff may not be directly
affected especially when a surgeon has cancelled an operation, the patient has
been informed, but the theatre booking has been retained.(3)
The traditional reasons
for cancellations are usually related to patients (ie. if they miss their
appointment, medically not fit for operation and in some instances they refuse
the surgery), organizational procedures (ie. availability of instruments and
tools such as prosthetic joints or ophthalmologic lenses), and clinical staff
(ie. overbooked lists, lack of proper communication between theatre staff and
surgeons).(4,5) One of the most common reasons is the
insufficient pre-operative medical assessment of patients which leads to case
cancellation usually by the anesthetist. Other common causes for cancellations include
ineffective planning and coordination within the clinical units (basically
between surgeons, anesthetists and theatre nurses), surgical list overruns (which
indicates the lack of time for the list to be performed) and the patients'
absence at the day of their scheduled appointment.
There
are many studies in the literature that investigate the rate and reasons of
cancellation and monitor the cancellation procedure of the elective operations.
The average percentage is between 10% to 40%(6-15) and it was
mentioned that more than half of the cancellations could be avoided by
redesigning work processes, improving planning and coordination between
clinical staff, and performing earlier clinical pre- operative assessment of
the patients.(16-18)
This study was conducted
at Queen Alia military hospital in Amman / Jordan to determine the number and
percentage, reasons and possible suggested measures to reduce the rate of
cancellation of elective surgical operations.
Methods
This study was prospectively
conducted at Queen Alia military hospital (QAH) in the period between January 1st
2011 and January 1st 2012.
This hospital is one of
the major hospitals of the Royal Medical Services
(RMS) in Amman/Jordan with a capacity of 200 beds. Surgical operations of
general surgery, orthopedic, otolaryngology, ophthalmology, gynecology and
maxillofacial surgery are routinely performed from Sunday to Thursday in 6
surgery rooms, one of them is usually reserved for emergency cases.
All patients planned for
elective surgery are either admitted before surgery for preoperative medical
assessment by a responsible internist or anesthetist or prepared few days
before surgery and operated as out-patients. The operating list is prepared by
the surgeons a day before the planned surgery then verified by the senior
consultant who is assigned to operate or supervise the other surgeons. A
pre-surgical anesthetic evaluation to assess patient’s fitness for surgery is
not usually performed before the operation unless requested by the senior
surgery consultant a day before surgery.
The Study included all
patients who were scheduled to undergo elective surgery and the operation was
cancelled for specific reason. The collected data from the operating room
included patients’ demographic data, the type of operation cancelled, and
reasons for cancellation. The reasons for cancellation were categorized as lack
of time, medical fitness, instruments availability, patient attendance and
others.
All data were collected
and analyzed using SPSS V. 16.0 (SPSS Inc., Chicago, IL, U.S.A.)
Results
A total of 7163 patients
were scheduled for elective surgery during the study period, 6601 patients had
their operation performed at the scheduled time of which 2449 were
out-patients and 4152 were in-patients. A total of 553 patients had their
operation cancelled at the day of surgery and the rate of cancellations was 7.72%.
The age of patients ranged between 2 to 90 years; average 43.7, there was no
significant difference between males and females in the cancellation group (male
to females ratio was 1:0, 85 and p>0.05).
The highest number of
cancellation was observed in December (70 cases out of 646 scheduled cases 10.84%) whereas February had lowest number of cancellations (23 cases out of 572 scheduled cases. 4.02%) Fig.1, Table I.
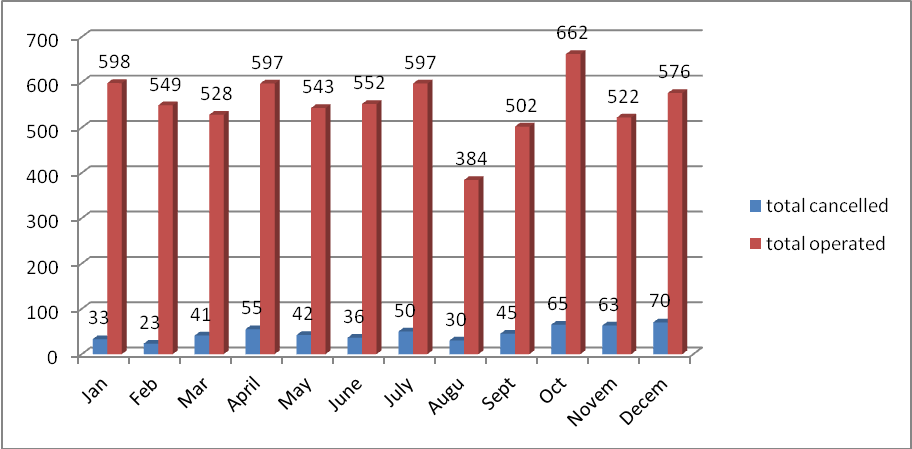
Fig. 1: Monthly operated and
cancelled surgeries
Table I: Contribution of every
specialty in cancellation rate
|
|
Cancelled cases
|
|
Operated cases
|
|
|
|
n
|
%
|
n
|
%
|
|
General surgery
|
186
|
34
|
1850
|
28
|
|
Ophthalmology
|
41
|
7
|
703
|
11
|
|
Gynacology
|
101
|
18
|
2107
|
32
|
|
Orthopedic
|
177
|
32
|
1327
|
20
|
|
ENT
|
38
|
7
|
427
|
6
|
|
Maxillofacial
|
10
|
2
|
187
|
3
|
|
Total
|
553
|
|
6601
|
|
Table II: Causes of cancellations
|
|
not fit
|
Equipments N/A
|
not attended
|
time
|
Other
|
Total %
|
|
General surgery
|
45
|
0
|
66
|
55
|
20
|
33.60
|
|
ophthalmology
|
18
|
0
|
15
|
3
|
5
|
7.40
|
|
Gynaecology
|
35
|
0
|
48
|
10
|
8
|
18.20
|
|
Orthopaedic
|
54
|
14
|
55
|
22
|
32
|
32
|
|
ENT
|
26
|
0
|
7
|
4
|
1
|
6.80
|
|
Maxillofacial
|
3
|
0
|
6
|
0
|
1
|
1.80
|
|
|
|
|
|
|
|
|
Potentially avoidable Non-Avoidable
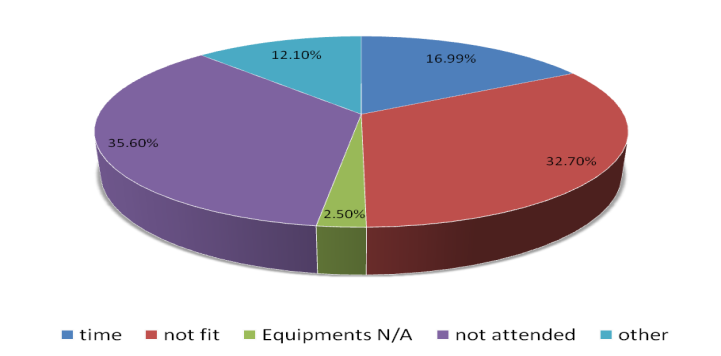
Fig. 2: Causes of
cancellations
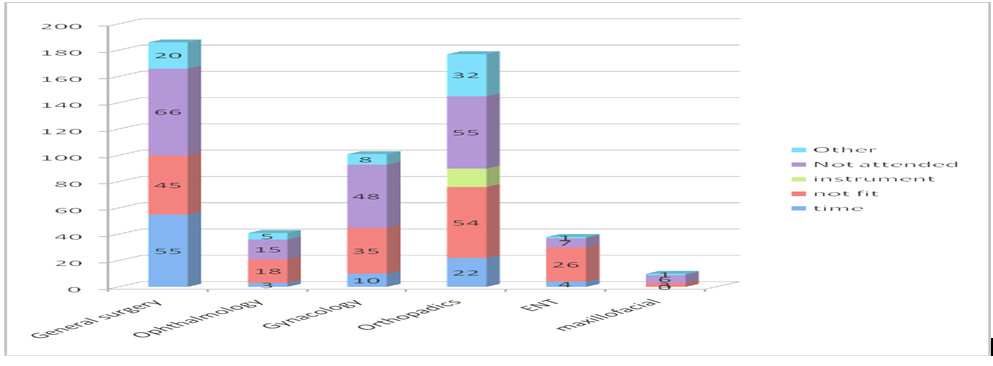
Fig. 3. The pattern of
cancellations of every surgical specialty
General surgery and
orthopaedics had the highest
number of cancellation (186 and
177 respectively) whereas ENT and maxillofacial surgery had the least number of
cancellations (38 and 10 respectively)
The most common causes
for cancellations were patient-related, around 68% of the cancellations were due
to patients’ absence and their medical fitness for surgery at the day of
planned operation, and the other causes of cancellations were due to lack of
time (overbooked list) or lack of necessary equipment and devices. Table II, Fig.
2.
The pattern of
cancellations of every surgical specialty is shown in Fig. 3
Discussion
The cancellation of
elective surgeries is a parameter to assess quality of patient care and quality
of healthcare management system; this is because of the negative impact of
cancellation on both patients and hospital. Thus it is considered by some
authors as a failure of the healthcare system and subsequently, an incident
report should be filled for each surgical cancellation.(14)
Cancellation also has a
major cost implication to the hospitals because of wasted hospital resources
and major impact on patients' health, psychological status and their families.
The Cancellation percentage
(7.72%) reported in our study is considered low
compared to other similar studies in the literature where the cancellation rate
ranged between 9% to 15% (18-22), This could be attributed to the relatively
strict monitoring of the overall operating theatre procedures.
It is clear from our
results that at least two thirds of the cancellations are potentially avoidable
and therefore the cancellation rate could even drop more, it is interesting
that 197 patient (35.60% of the cancellation rate) did not show up at the day
of planned surgery, thus, a strong emphasis on preoperative communication with
patients or their relatives has a paramount importance on decreasing the total
number of cancelled cases, whereas about 33% of the cancellations were due to inadequate
patient
preparation for general anesthesia. This is emphasized by other
investigators who also mentioned the idea of avoidable cancellations.(15)
The preoperative anesthetic
evaluation could also play a significant role in the reduction of the
cancellation rate. In order to avoid cancellations of medically unfit patients,
a thorough preoperative anesthetic assessment is essential.(23)
Unfortunately, preoperative anesthetic clinic for the evaluation of medical and
anesthetic fitness of the patient is not routinely performed in our hospital,
and this is because of the lack of manpower to run such clinics.
Another interesting
point was also noticed in orthopaedic surgery; lack of necessary instruments
such as prosthetic joints or drills and saws contributed in about 3% of the
cancellation rate, therefore sufficient
preparing of the theatres and preoperative arrangement with the relevant
instruments’ providers would surely reduce the cancellation rate attributed to this
cause.
Finally; it was noticed
that general surgery and orthopaedics contributed in about 66% of the
cancellation rate; therefore it might be wise to review the current protocol of
the surgical operation procedures in order to reduce their cancellation.
Based on our results, it
was found that the vast majority of cancellations could be avoided by improving
the hospital procedures and protocols through the following recommendations
1. Establishment of preoperative anaesthesia
clinic to assess the medical fitness of patients undergoing elective surgeries at
least for those who have a remarkable medical history.
2. Ensuring the availability of necessary
instrument and tools especially for orthopaedic surgery patients such as
prosthetic joints and drills and saws before preparing the surgical list.
3.
Preparing the surgery list after proper
communication with patients or their relatives to ensure that they will attend
for the operation.
4. Re-calculating the necessary surgery time
required for the lists to be performed especially by the general surgery staff.
5. Performing a monthly or bimonthly audit
to review the cancelled cases, investigate the reasons of cancellation and
regularly update the hospital protocols to prevent future cancellations
Conclusions
The rate of surgical
cancellation in our hospital is relatively low; most of the cancellations could
be easily avoided by preparing the theatres, proper communication with the
patients and proper preoperative medical assessment. Further improvement of operating
theatre system is highly advised and can be implemented by new guidelines and
more strict enforcement of procedures and regulations.
References
1. Robb WB1, O'Sullivan MJ,
Brannigan AE, et al. Are elective surgical operations
cancelled due to increasing medical admissions? Irish Journal of Medical
Science 2004; 173:129-132.
2. Rakesh G, Anju RB,
Poonam B, et al. Reasons for cancellation of cases on the
day of surgery–a prospective study. Indian Journal of Anaesthesia 2009;
53 (1):35-39.
3.Schofield WN, Rubin G,
Piza M, et al. Cancellation of operations on the day of
intended surgery at a major Australian referral hospital. Medical Journal of
Australia 2005; 182: 612-615.
4. Tait AR,
Voepel-Lewis T, Munro HM, et al. Cancellation
of pediatric outpatient surgery: Economic and emotional implications for
patients and their families. J Clin Anesth 1997; 9(3):213-219.
5. Ivarsson B, Larsson S,
Sjöberg T. Postponed or cancelled heart operations from
the patient's perspective. J Nurs Manag 2004; 12(1):28-36.
6. Ivarsson B, Kimblad PO,
Sjöberg T, Larsson S. Patient reactions to cancelled or postponed
heart operations. J Nurs Manag 2002; 10: 75- 81.
7. Dix P, Howell S. Survey of
cancellation rate of hypertensive patients undergoing anaesthesia and elective
surgery. Br J Anaesth 2001; 86:789-793.
8. Aaserud M, Trommald M,
Boynton J. Elective surgery cancellations, ring fencing
and efficiency. Tidsskr Nor Laegeforen 2001; 121: 2516-2519.
9. Pollard JB, Olson L. Early
outpatient preoperative anaesthesia assessment: does it help to reduce
operating room cancellations? Anesth Analg 1999; 89: 502-525.
10.Chalya PL, Gilyoma JM,
Mabula JB, et al. Incidence, causes and
pattern of cancellation of elective
surgical operations in a University Teaching Hospital in the Lake Zone,
Tanzania. African Health Sciences 2011; 11(3): 438-443.
11.Hussain AM, Khan FA. Anesthetic
reasons for cancellation of elective surgical inpatients on the day of surgery
in a teaching hospital. J Pak Med Assoc 2005 Sep; 55(9):374-378.
12. Singha GC, Aghaa R,
David R. Roberts. Cancellations in day-case ENT surgery. J of
Ambulatory Surgery 2005; 12: 57-60
13. Nabeel S, Rashid A, Abbas SM.
Reasons for cancellation of elective cardiac surgery at Prince Sultan Cardiac
Centre, Saudi Arabia. J Saudi Heart Assoc Jan 2012; 24(1): 29–34.
14.Leslie RJ, Beiko D, Van Vlymen J, Siemens DR. Day of surgery cancellation rates in urology:
Identification of modifiable factors. Can Urol Assoc J 2013 May-Jun;
7(5-6): 167-173.
15. Rajender K, Ritika G. Reasons for
cancellation of operation on the day of intended surgery in a multidisciplinary
500 bedded hospital. J Anaesthesiol Clin Pharmacol 2012 Jan-Mar; 28(1):
66-69.
16.
Hovlid E, Bukve O,
Haug K, et al. Sustainability of
healthcare improvement: what can we learn from learning theory?. BMC Health
Services Research 2012; 12(1):235.
17. Schofield WN, Rubin
GL, Piza M, et al. Cancellation of
operations on the day of intended surgery at a major Australian referral
hospital. The Medical Journal of Australia 2005; 182(12):612- 615.
18. Sanjay P, Dodds A,
Miller E, et al. Cancelled elective operations: an
observational study from a district general hospital. Journal of Health Organization
and Management 2007; 21(1):54-58.
19. Ezike HA, Ajuzieogu VO,
Amucheazi AO. Reasons for elective surgery cancellation in a
referral hospital. Ann Med Health Sci Res 2011 Jul-Dec; 1(2): 197-202.
20. Rai
M, Pandit JJ. Day of surgery cancellation after nurse led
pre-assessment in an elective surgical centre: the first 2 years. Anesthesia 2003; 58:692-9.
21. Dakum NK, Ramyil VM,
Misauno MA, et al. Reasons for
cancellations of urologic day care surgery. Nigerian of Surgical Research
2006; 8(1-2): 30-33.
22. El-Bushra AD, Mohamed
IM, Awadalla MA, et al. Cancelled elective
surgical operations at El Obeid Hospital, Western Sudan. Sudan Med J
2008; 44 (1, 2 & 3):56-61.
23. Sapna B, Anup M, Aikta
G, et al. Cancellation of elective cases in pediatric surgery: An audit. J Indian
Assoc Pediatr Surg 2010; 15(3): 90-92.