ABSTRACT
Objectives: To determine if central
corneal thickness influences Intra Ocular Pressure (IOP) lowering response of Selective
Laser Trabeculoplasty (SLT) in patients with medically uncontrolled primary open
angle glaucoma.
Methods: Consecutive patients who received selective laser
trabeculoplasty during May 2011 through June 2013 were enrolled in this
retrospective chart review study. Information gathered included age, gender,
race, central corneal thickness and type of glaucoma. Number of glaucoma
medications, visual acuity, and IOP were assessed before and after treatment.
Results: Data from 48 patients (77
eyes) were used in the analysis. There
were no significant differences in the number of glaucoma medications used or
visual acuity before or after treatment.
IOP measurements decreased 10.3% over preoperative levels through 18-months
from a mean preoperative pressure of 18.4 ±
5.5 to 16.5 ± 4.7 mmHg (P < 0.0005). The mean central corneal thickness was 533.8 ±
38.0 mm. The treated eyes were divided into two groups
by central corneal thickness: thin
(<555mm), and thick (>555mm).
There was no difference in mean IOPs of the groups preoperatively, but
during the 18 months follow-up there was a significant mean change in intraocular pressure within the thin group (-2.5 mmHg, 95%CI
[-3.8, -1.2], p=0.0002) but not in the
thick group (-1.6mmHg, 95% CI [-3.4, +0.2], p=0.08). However, the difference
between the central corneal thickness
groups was not statistically significant.
Conclusions: Selective laser
trabeculoplasty was more effective in reducing IOP, when used as an adjunct to
medical therapy for glaucoma, in patients with thin central corneal thickness (<555mm)
than those with thick central corneal
thickness (>555mm).
Key words: Central Corneal Thickness (CCT), Intraocular Pressure (IOP), Primary Open
Angle Glaucoma (POAG), Selective Laser Trabeculoplasty (SLT).
JRMS
December 2015; 22(4): 6-11 / DOI: 10.12816/0018543
Introduction
Selective laser
trabeculoplasty (SLT) has been shown to be both an effective and safe method
for reducing intra ocular pressure (IOP) in patients with primary open angle
glaucoma (POAG)(1-4) and as efficacious as the previous
laser-procedure of choice, argon laser trabeculoplasty (ALT).(5-7)
It is also well known that a thinner central
corneal thickness (CCT) is an important risk factor for development of primary
open angle glaucoma (POAG) and increased glaucoma severity.(8-10)
The role of SLT as a
first line mode of treatment has been studied in patients with POAG and ocular
hypertension with positive results.(11) More recently, Shazly
and associates have shown that patients with thinner CCT showed better IOP
control when SLT was used as a primary therapy.(12)
However, the interplay between
SLT and CCT is not well understood when SLT is used as an adjunct to medical
therapy in glaucoma. This information would be useful to predict response to SLT
based on CCT. We addressed these questions by retrospectively reviewing the outcome
of patients with who had undergone SLT at our institution. We hypothesized that
SLT would reduce IOP further when used in conjunction with medical therapy and patients
with thinner CCT would show greater IOP reduction.
Methods
After approval by the
Institutional Review Board of the University of Texas Southwestern Medical
Center (UTSW), a retrospective chart review of consecutive patients who had
undergone SLT for open angle glaucoma at the UT Southwestern Medical Center was
performed. Medically uncontrolled patients
with open angle glaucoma or pseudoexfoliation glaucoma who underwent the
procedure between May 2011 and June 2013 and who were older than 18 years of
age were included. Patients were
excluded if they had: any identifiable secondary glaucoma other than
pseudoexfoliation, intraocular surgery (cataract, glaucoma or retina),
follow-up data less than 3 months, use of systemic or topical steroids and
prior ALT within two years. We adhered to the tenets of the Declaration of
Helsinki.
Baseline information
gathered included patient age, gender, race, type of glaucoma, number of
glaucoma medications used preoperatively, previous ALT, visual acuity, IOP, and
CCT. Baseline IOP was defined as the IOP
measured immediately prior to performing SLT.
Intra-ocular pressure measurements were made using Goldmann applanation
tonometry, and the CCT measurements were made using the Corneo-Gage Plus
pachymeter (Sonogage, Inc., Cleveland, OH). The observers taking the IOP or CCT
measurements were not masked. Eyes were divided into thin cornea if the CCT was
less than 500mm, average cornea if
between 500-568mm and thick cornea if
the CCT was greater than 568mm.
Selective laser trabeculoplasty (SLT) was performed by one surgeon (KSK) in a
standard fashion in all cases at UTSW as follows. All patients provided written
informed consent after the potential risks, benefits, and alternatives to the
procedure were explained. Selective laser trabeculoplasty was
delivered with the Selecta II Glaucoma Laser System, a Q-switched 532-nm frequency-doubled
Nd: YAG laser (Lumenis Inc., Santa Clara, CA, USA). The subjects were pre-medicated with topical
proparacaine 0.5% and apraclonidine 0.5%.
A Latina gonio-lens (Ocular Instruments, Bellevue, WA, USA) was placed
on the eye coupled with methylcellulose 1%.
The helium-neon aiming beam was focused on the pigmented trabecular
meshwork with a pre-adjusted spot size of 400 mm.
To deliver the least amount of energy possible, the pulse energy was adjusted
by increments of 0.1 mJ to the smallest amount until “champagne” bubble
formation became just invisible. Each
treatment area consisted of non-overlapping laser spots over 180°, 270°,
or 360° of the visible angle. Immediately following the conclusion of the
procedure, drops of topical apraclonidine 1% and either prednisolone acetate 1%
or loteprednol 0.5% were instilled.
Postoperatively, IOP was
measured in both eyes at 1 hour. If the
IOP was elevated by more than 5 mmHg, the pressure was treated medically and
rechecked before discharging the patient.
Anterior chamber reaction was assessed by slit lamp bio-microscopy.
Discharge medications
included loteprednol 0.5%, fluoromethalone 0.25%, or diclofenac 0.1% four times
daily for one week. Patients were
continued on their preoperative anti-glaucoma therapy. Follow-up information
included IOP measurements at 1 week, and 1-, 3-, 6-, 12-, and 18-months. Additional information gathered were the last
recorded IOP measurement, number of glaucoma medications, visual acuity, and if
repeat SLT was performed.
All postoperative complications were documented
and treated appropriately.
Statistical
Analyses
The statistical analysis
was performed using SAS 9.4 (SAS, NC, USA). Descriptive statistical analysis
was done to characterize clinical and functional data. Mean values for visual
acuity were calculated after transforming the mean angle of resolution values
to-log MAR values. A mixed-effects linear model was used to assess trends over
the repeated measurements and to compare the means of the two CCT groups. To
account for the correlation between paired eyes of one individual, each subject
was modeled as a random effect. A mixed effects model for change in IOP was
also constructed, modeling CCT as a continuous variable and controlling for
preoperative IOP at each follow-up visit.
A P value less than 0.05 was considered
statistically significant.
Results
Out of a total of 107
patients, thirty-two patients were excluded due to insufficient follow-up data
(less than 3 months following SLT), and 27 patients were excluded for previous
intraocular surgery. Data from the 48 remaining patients were used
for the study. Twenty-nine patients had
the procedure repeated in the contralateral eye for a total of 77 eyes treated.
Patient demographics and
baseline characteristics are listed in Table I. Fourteen patients (29.2%) had ALT prior to
receiving SLT. Using the Log MAR scale,
the mean preoperative visual acuity was 0.24± 0.4 (range, 0-1.3).
The average number of
SLT pulses placed in each treated eye was 79.4 ±
27.3 (range, 50-150), of which only 19 eyes (24.7%) were treated with greater
than 100 pulses. Thirty-two eyes (42%)
received 180° of treatment, 7 (9%)
received 270°, and the remaining 38
(49%) received 360° of treatment.
Two eyes (2.6%)
experienced postoperative complications, both of which were anterior chamber
inflammation that responded well to topical corticosteroid drops without
further sequelae. Five eyes (6.5%)
underwent repeat SLT after 1 year.
Table 1: Baseline characteristics of patients (n = 77
eyes of 48 patients)
|
Variables
|
|
|
Sex
|
|
|
Male
|
16 (33%)
|
|
Female
|
32 (67%)
|
|
Age, years
|
65.2 ± 10.5
|
|
Total eyes treated
|
|
|
Right
|
40 (52%)
|
|
Left
|
37 (48%)
|
|
Race
|
|
|
White
|
21 (44%)
|
|
Black
|
22 (46%)
|
|
Hispanic
|
4 (8%)
|
|
Other
|
1 (2%)
|
|
Glaucoma type
|
|
|
Primary open-angle
|
42 (88%)
|
|
Pseudoexfoliation
|
6 (12%)
|
|
Anti-glaucoma medications
|
1.9 ± 0.8
|
|
Intraocular pressure, mm Hg
|
18.4 ± 5.5
|
|
Central corneal thickness, µm
|
533.8 ± 38.0
|
Data are presented as the number of patients (%)
and mean ± standard deviation
In the follow-up period,
patients were using a mean of 1.9 ±
0.8 anti-glaucoma medications with no change in the number of medications from
preoperatively (P = 0.69). Latest visual acuity assessed in the
postoperative period (mean = 16 months) using the scale above was 0.21 ± 0.2, which was unchanged when compared
to the preoperative visual acuity (P
= 0.64).
IOP measurements in the
follow-up period showed a sustained decrease over preoperative levels (Fig. 1).
Each follow-up mean IOP (week 1 to month 18) was decreased compared to baseline
(P= 0.0005, time effect from mixed model repeated measures analysis).
From a mean preoperative IOP of 18.4 ±
5.5 mmHg, the reduction postoperatively was significant
at the 1-week (16.5 ± 4.0mmHg, P < 0.0005), 1-month (16.0 ±
4.7mmHg, P < 0.0002), 3-month
(16.4 ± 4.7mmHg, P < 0.0002), 6-month (16.1 ± 4.8mmHg, P < 0.0006), 12-month (16.5 ±
4.7mmHg, P < 0.0004) and 18-month
follow up (16.6 ± 4.7 mmHg, P = 0.01).
The mean CCT of the 77 eyes
was 533.8 ± 38.0mm.
Fifty one eyes (66.2%) had thin cornea, and 26 eyes (33.8%) had thick
cornea.
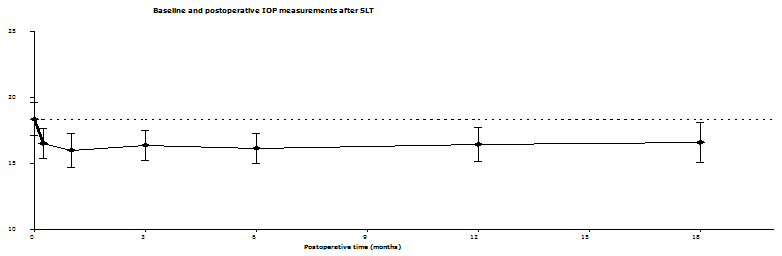
Fig. 1: Mean intraocular
pressure at baseline and in the follow-up period. Vertical error bars represent 95% confidence
intervals. The dashed line is the
baseline mean preoperative intraocular pressure measurement. IOP = intraocular pressure; SLT= selective
laser trabeculoplasty. Each follow-up
mean IOP (week 1 to 18) was decreased compared to baseline, (P=0.0005)
Table II: Effect of CCT on selective laser
trabeculoplasty IOP measurements
|
Variables
|
Preop
|
1 wk.
|
1 mo
|
3 mo
|
6 mo
|
12 mo
|
18 mo
|
|
CCT < 555
N=51 eyes
Pts=32
|
17.6
|
15.7
(-14.3%)
|
15.1
(-8.1%)
|
15.3
(-10.2%)
|
15.3
(-9.0%)
|
15.4
(-13.3%)
|
15.0
(-11.9%)
|
|
CCT>=555
N=26 eyes
Pts=16
|
19.8
|
18.3
(-9.0%)
|
17.4
(-9.7%)
|
18.8
(-5.6%)
|
17.7
(-8.1%)
|
18.0
(-6.8%)
|
18.8
(-4.8%)
|
|
⃰P
value between groups
|
0.07
|
0.37
|
0.68
|
0.34
|
0.81
|
0.44
|
0.64
|
⃰ P
value comparing the two CCT groups from mixed-effect model repeated measure
analysis.
CCT, central corneal thickness; IOP, intraocular
pressure; preop, preoperatively; wk, week; mo, month(s); thin group, CCT <
555 µm; thick group, CCT >555 µm; pts, patients.
Results are presented as mean (percent change
from baseline)
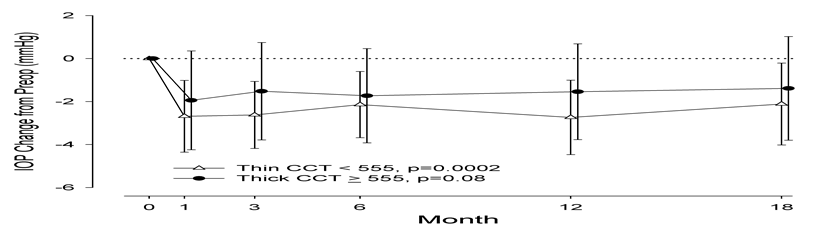
Fig.
2:
Intraocular pressure change after selective laser trabeculoplasty from
pre-operative value over time (1 week - 18 months) in the two central corneal
thickness groups.
Thin
CCT = < 555 mm. Thick CCT= > 555 mm. Symbols and error bars represent mean
and standard deviation, respectively
The measurements of the IOP at baseline and in
the follow-up periods of the two CCT groups are listed in Table II. The baseline IOP in the two groups was similar
(P=0.07). The thin group had greater
reduction of IOP at each visit.
The differences in mean
IOP values by CCT groups at baseline and postoperatively were also explored. The
changes from baseline were not statistically different among the two CCT groups
(P=0.37). Fig. 2 illustrates the
change of IOP over the 18 months of the study stratified by the two CCT groups.
Treating CCT as a
continuous variable and controlling for preoperative IOP as a covariate, we
observed significant associations between CCT and change in IOP at month 6
(adjusted regression coefficient (β) =0.06 ΔmmHg/µm, P=0.002) and month 12 (β)
=0.05, P=.008),
indicating that larger IOP decreases are
associated with lower CCT. Less robust associations were observed at month 1
(β) =0.02, P=0.18), month 3 (β) =0.03, P=0.055), and month 18 (β)
=0.05, P=0.052).
Discussion
In our medically
uncontrolled patients with glaucoma, we found that SLT reduced preoperative IOP
by 10.3% through 18-months of follow-up from the mean preoperative pressure of
18.4 ± 5.5 to 16.5 ± 4.7 mmHg (P < 0.0005). These
results are in line with the meta-analysis report of several SLT studies which
found IOP reduction of 6.9% to 35.9%.(4)
In terms of the role of
CCT in influencing the outcome of SLT, we found that in patients with thin CCT
(<555µm) there was a significant mean change in IOP during the 18 months follow-up
(-2.5mmHg, 95% CI [-3.8, -1.2], p=0.0002) but not in the thick (>555µm)
group (-1.6 mmHg, 95% CI [-3.4, +0.2], p=0.08).
The pre-op IOPs in both groups were similar but we did not detect any
significant difference in the post-SLT IOPs in the thin and thick groups.
Larger numbers of patients are needed to address this question. Our results do
confirm the findings of Shazly and associates who have shown that eyes with
thinner cornea experience greater reduction of IOP following SLT as a primary
procedure in patients with POAG and ocular hypertension.(12)
Previous groups have
hypothesized that differences in response by corneal thickness to ocular
hypotensive medications may be from differences in corneal compliance, lower
baseline IOP in thicker corneas, and inherent pharmacokinetic variations.(10,13-14)
Although pharmacokinetic differences do not apply directly to SLT, the amount
of laser energy that is able to penetrate the cornea to the trabecular meshwork
may be influenced by CCT. In our study,
this effect could explain why patients with thin corneas had a more robust
response to SLT while patients with thick corneas had less response. This would be in agreement with a study that
found 180° of SLT to be more
effective at lowering IOP than 90°
of SLT.(15) Although that study did not investigate whether
there was a relationship between the amount of energy delivered per pulse
versus IOP reduction, the total amount of energy delivered to the meshwork may
play an important role in the efficacy of SLT and may be influenced by CCT. Finally, there may be inherent differences
between eyes with a thin CCT versus eyes with a thick CCT in the production and
drainage of aqueous humor, that is, patients with thin corneas may have a
higher predisposition for increased aqueous humor production or decreased
drainage, causing an increased risk for POAG and decreased response to
treatment.
Our results are in
agreement with much of the literature on the successfulness of SLT in lowering
of IOP.(1-7,11-12)
Although the difference between the preoperative mean IOP and
postoperative measurements were not as large as previous studies, there was a
statistically significant decrease in IOP seen during the study follow-up.
Selective laser trabeculoplasty was a safe procedure in our study, with only
two patients experiencing complications that were readily treated without
sequelae. Additionally, although there
was no change in the amount of anti-glaucoma medications used after SLT, it was
encouraging that no further anti-glaucoma medications were added and visual
acuity remained the same in the follow-up period from preoperatively.
Although this study is limited
by its retrospective nature and small sample size in the CCT groups, our
results may provide guidance to clinicians in choosing treatment modalities and
providing patients with an improved understanding about possible outcomes after
SLT. Central corneal thickness may also help to explain the differences in IOP
response of some patients to one modality of treatment versus another. Future directions of study include a
prospective study to confirm the results of our investigation and whether
patients with differences in CCT have structurally different corneo-scleral
angles. Thin CCT has been found to be a
risk factor for the development of glaucoma, and it remains to be determined if
CCT may also serve as a surrogate marker for anatomical differences in angle
anatomy.
Conclusion
Our study has
demonstrated that SLT is a viable and safe option for patients with medically
uncontrolled glaucoma.
Patients with CCT < 555µm had significant reduction in
IOP over 18 months than those with CCT >555µm. The results comparing both groups were
inconclusive because of small number of patients. A larger, prospective study
is necessary to answer the influence of CCT and SLT in patients with medically
uncontrolled glaucoma.
Acknowledgements
Supported in part by
unrestricted grant from the Research to Prevent Blindness New York, NY, Visual
Science Core Grant EY 020799 and NIH CTSA Grant UL1-RR024982
References
1. Latina MA, Sibayan
SA, Shin DH, et al. Q-switched 532-nm Nd:
YAG laser trabeculoplasty (selective laser trabeculoplasty): a multicenter,
pilot, and clinical study. Ophthalmology
1998; 105:2082-2088.
2.Lai JS, Chua JK,
Tham CC, Lam DS. Five-year follow up of
selective laser trabeculoplasty in Chinese eyes. Clin Experiment Ophthalmol 2004; 32:368-372.
3. Leahy KE, White AJR. Selective laser
trabeculoplasty: current perspectives.
Clinical Ophthalmology 2015; 9: 833-841.
4. Wong MO, Lee JW, Choy BN, et al. Systematic review and
meta-analysis on the efficacy of selective laser trabeculoplasty in open-angle
glaucoma. Surv Ophthalmol. 2015; 60(1):36–50.
5. Juzych MS, Chopra V, Banitt MR, et al. Comparison of long-term
outcomes of selective laser trabeculoplasty versus argon laser trabeculoplasty
in open-angle glaucoma. Ophthalmology
2004; 111:1853-1859.
6.Damji KF, Bovell AM, Hodge WG, et al. Selective laser
trabeculoplasty versus argon laser trabeculoplasty: results from a 1-year randomized
clinical trial. Br J Ophthalmol 2006;
90:1490-1494.
7.Wang W, He M, Zhou M, Zhang X. Selective Laser
Trabeculoplasty versus Argon Laser Trabeculoplasty in Patients with Open-Angle
Glaucoma: A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8(12): e84270.
8.Gordon MO, Beiser
JA, Brandt JD, et al. The Ocular Hypertension
Treatment Study: baseline factors that predict the onset of primary open-angle
glaucoma. Arch Ophthalmol 2002;
120:714-720.
9. Herndon LW, Weizer
JS, Stinnett SS. Central corneal
thickness as a risk factor for advanced glaucoma damage. Arch Ophthalmol 2004; 122:17-21.
10. European Glaucoma Prevention Study (EGPS) Group,
Miglior S, Pfeiffer N, Torri V, Zeyen T, Cunha-Vaz J, Adamsons I. Predictive
factors for open-angle glaucoma among patients with ocular hypertension in the
European Glaucoma Prevention Study. Ophthalmology
2007; 114:3-9.
11.McIlraith I, Strasfeld M, Colev G, Hutnik CM. Selective laser
trabeculoplasty as initial and adjunctive treatment for open-angle glaucoma. J
Glaucoma 2006; 15:124-130.
12. Shazly TA, Latina MA, Dagianis JJ, Chitturi S. Effect of central
corneal thickness on the long-term outcome of selective laser trabeculoplasty
as primary treatment for ocular hypertension and primary open-angle glaucoma. Cornea 2012; 31(8):883-886. DOI:
10.1097/ICO.0b013e318243f684
13.Brandt JD, Beiser JA, Gordon MO, Kass MA. Ocular Hypertension
Treatment Study (OHTS) Group. Central corneal thickness and measured IOP
response to topical ocular hypotensive medication in the Ocular Hypertension
Treatment Study. Am J Ophthalmol 2004; 138:717-722.
14.Hirneiß C, Sekura K, Brandlhuber U, Kampik A,
Kernt M.
Corneal biomechanics predict the outcome of selective laser trabeculoplasty in
medically uncontrolled glaucoma. Graefes
Arch Clin Exp Ophthalmol 2013 251:2383–2388. DOI 10.1007/s00417-013-2416-2.
15. Chen E, Golchin S, Blomdahl S. A comparison between 90
degrees and 180 degrees selective laser trabeculoplasty. J Glaucoma
2004; 13:62-65.